Long-term follow-up study on nutritional problems and health-related quality of life among head and neck cancer survivors more than 5 years after diagnosis
Camilla Wallmander, Hedda Haugen Cange, Ewa Silander, Helen Larsson, Malin Börjesson, Leif Johansson, Ingvar Bosaeus, Eva Hammerlid

TL;DR
This study examines long-term nutritional issues and quality of life in head and neck cancer survivors more than five years after diagnosis.
Contribution
The study provides new insights into long-term nutritional rehabilitation needs and HRQoL in HNC survivors.
Findings
Many survivors needed dietary adjustments like extra liquid and moist food.
Survivors reported severe HNC-specific symptoms compared to a normal population.
Nutritional problems were linked to worse role and social functioning.
Abstract
Few studies have evaluated the long-term effects of head and neck cancer (HNC) and its treatment. Therefore, the objective was to study nutritional rehabilitation needs by assessing nutritional problems, dietary adjustments, muscle mass, muscle strength, physical performance, prevalence of sarcopenia, and health-related quality of life (HRQoL) among long-term HNC survivors. This cross-sectional study included HNC survivors more than 5 years after diagnosis. Nutritional status, sarcopenia, and physical performance were assessed through questions about dietary adjustments, muscle mass (bioelectrical impedance analysis), grip strength, and maximum walking speed measurements. HRQoL and nutrition impact symptoms (NISs) were assessed using quality of life questionnaires from the European Organization for Research and Treatment of Cancer (EORTC), QLQ-C30 and QLQ-HN35, and were compared with…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
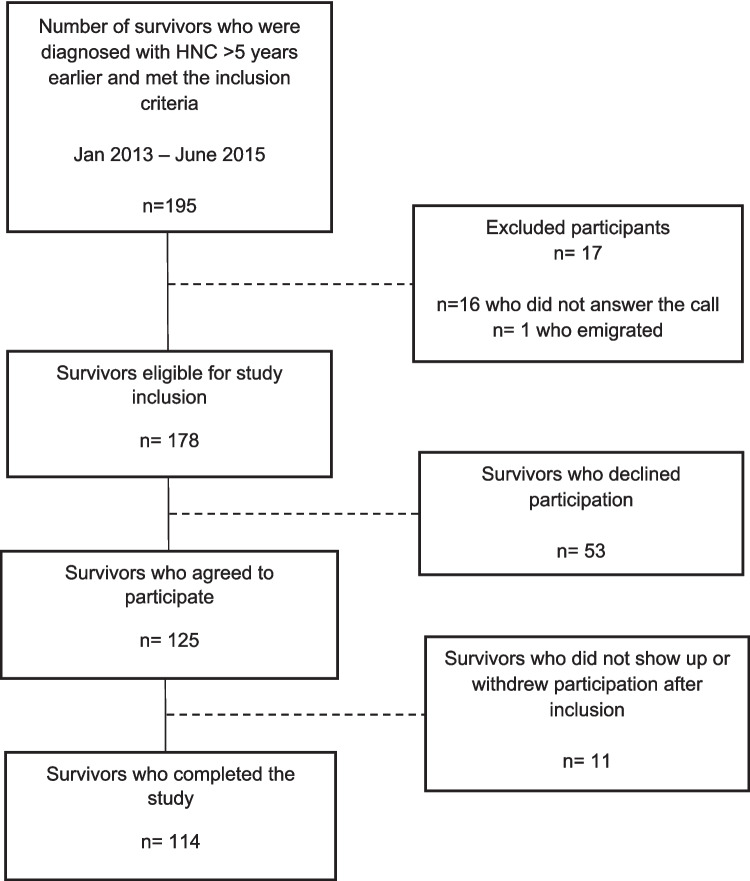 Figure 1
Figure 1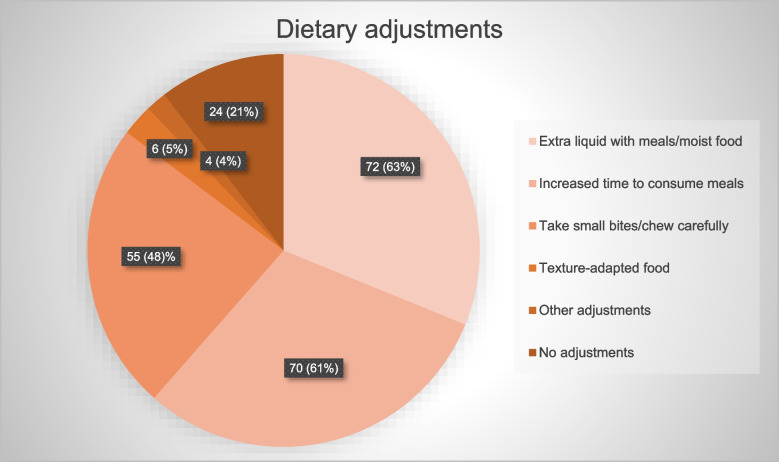 Figure 2
Figure 2- —the Local Research and Development Council Gothenburg and Södra Bohuslän
- —the Operational Healthcare Committee, Region Västra Götaland in Sweden
- —the Swedish state under the agreement between the Swedish government and the county councils Västra Götaland Region, the ALF agreement
- —University of Gothenburg
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNutrition and Health in Aging · Oral health in cancer treatment · Head and Neck Cancer Studies
Introduction
Head and neck cancer (HNC) includes tumors of the lip, oral cavity, salivary glands, oropharynx, hypopharynx, larynx, nasopharynx, and nasal sinuses. HNC is the seventh most common cancer diagnosis worldwide, with a 5-year survival rate of approximately 50–60%, which varies greatly depending on the tumor site and presents discrepancies across countries [1–3]. Treatment includes surgery, radiation, and chemotherapy, either alone or in combination [4]. Treatment side effects often lead to the development of nutrition impact symptoms (NISs), which affect the ability to eat, and common NISs are pain, dry mouth, sticky saliva, dysphagia, and problems with teeth, chewing, or opening the mouth wide [5, 6]. Nutritional problems can lead to the need for dietary adjustments, insufficient food intake, weight loss, loss of muscle mass, and malnutrition and can negatively affect health-related quality of life (HRQoL) [5–8]. It is common for patients to experience acute NISs before and during treatment, but complications can also persist after treatment and become chronic [5]. In HNC survivors, NISs and impaired HRQoL have been reported to persist for up to 5 years after diagnosis, with the greatest deterioration occurring during treatment [9–11]. There have been few long-term follow-up studies on nutritional problems, nutritional status, and HRQoL more than 5 years after diagnosis, and the majority have included a small sample of HNC survivors [12–18]. With the increasing incidence of HNC and improved survival rates, research focusing on the growing population of HNC survivors is warranted. The need for nutritional rehabilitation, e.g., the need for optimization of energy and nutrient intake, management of NISs and unfavorable changes in body weight, body composition, and function, after routine clinical tumor controls at specialist clinics have ceased has not been sufficiently researched [19]. The primary objective of this study was therefore to evaluate whether nutritional rehabilitation is needed for long-term HNC survivors diagnosed more than 5 years earlier, by assessing the need for dietary adjustments, use of oral nutritional supplements, and enteral nutrition, and to evaluate muscle mass, muscle strength, physical performance, sarcopenia, and HRQoL. The secondary aims were to describe and analyze a subgroup of participants with self-reported problems swallowing solid food and to compare the survivors’ HRQoL with reference values from a normal Swedish population.
Method and materials
Study design and study population
This cross-sectional long-term follow-up study of HNC survivors was conducted in four hospitals in western Sweden. This study is part of a multinational study conducted by the Quality of Life Group and the HNC Group of the European Organization for Research and Treatment of Cancer (EORTC), which aimed to describe late toxicity and HRQoL in HNC survivors, after clinical tumor controls have ceased at the specialist clinic 5 years after diagnosis [20]. The inclusion criteria were a diagnosis of cancer of the lip, oral cavity, oropharynx, nasopharynx, hypopharynx, larynx, salivary glands, or HNC of unknown primary (HNCUP) > 5 years earlier; ≥ 18 years of age; and the ability to attend clinics and complete questionnaires in Swedish. Patients with ongoing HNC or other cancers were excluded. Participants diagnosed from 2013 to 2015 were identified consecutively via the register available from the multidisciplinary tumor board at Sahlgrenska University Hospital. Information about the study was sent by mail to eligible participants, and after 1–2 weeks, they were contacted by telephone and asked about their participation. An invitation for a physical visit was sent by mail to those who agreed to participate. The participants received oral and written information and gave their written consent to participate in the study that took place between April 2021 and December 2021. The study visit included a clinical examination by a physician from the Department of Otorhinolaryngology or Oncology; measurements of body composition, muscle strength and physical performance; questions about dietary adjustments, oral nutritional supplements (ONSs), and enteral nutrition; and quality of life (QoL) questionnaires. The QoL questionnaires were sent to the participants in advance and returned at the study visit.
Nutritional status and physical performance
Nutritional status and physical performance were assessed by measuring body weight, body composition, muscle strength, and walking speed. Body weight was measured to the nearest 0.1 kg, height was measured to the nearest 0.5 cm, and body mass index (BMI) was calculated. BMI was categorized according to cutoffs for underweight (< 18.5 kg/m^2^), normal weight (18.5–24.9 kg/m^2^), overweight (25–29.9 kg/m^2^), and obesity (> 30 kg/m^2^). A BMI < 20 kg/m^2^ for those aged < 70 years or < 22 kg/m^2^ for those aged ≥ 70 years is also often used as a cutoff for low BMI and was thus also presented [21]. Body composition was measured via bioelectrical impedance analysis (BIA) (Nutribox, Data Input, Lindenberg 7 82343 Pöcking, Germany) [22, 23]. BIA assessments were performed in a standardized manner with participants in the supine position, with two surface electrodes on the right hand and two on the right foot [23]. Participants were instructed not to eat or drink 2 h prior to the study visit, and before measurement was conducted, participants were required to lie supine for 5–10 min. The equation by Dey et al. [24] was used to calculate fat-free mass (FFM). The fat-free mass index (FFMI) was calculated by dividing the FFM (kg) by the height^2^ (m), and FFMI < 17 kg/m^2^ for men and < 15 kg/m^2^ for women were considered reduced muscle mass [21]. Muscle strength was assessed by measuring grip strength with a digital hand dynamometer (JAMAR® Plus+). The participants sat upright in a chair; in total, three attempts for each hand were performed, and the best result was recorded [25]. Hand grip strength < 27 kg for men and < 16 kg for women indicated reduced muscle strength [26]. Physical performance was assessed through a 10-m walk at maximum pace with acceleration and deceleration phases of 2 m each [27]. Participants were instructed to walk from the starting point to a visual cone placed at 14 m. Two attempts were made, and the best result was recorded. Sarcopenia was assessed using the diagnostic criteria of the European Working Group on Sarcopenia in Older People (EWGSOP2), where low muscle strength together with low muscle mass is required for diagnosis [26]. The study dietitian asked participants about the use of dietary adjustments to facilitate food intake, if they had an enteral feeding tube, and if they used oral nutritional supplements (ONSs). There were four questions about dietary adjustments: “Do you feel that it takes a long time to eat a meal?”; “Do you need to drink extra liquid with meals and/or do you need food to be moist?”; “Do you need to take small bites/chew carefully?”; “Do you need to adjust the texture of your food?” All the questions were based on participants’ perceptions of their need for dietary adjustments, and there was no definition of “a long time” in the question “Do you feel that it takes a long time to eat a meal?” All questions were dichotomous (yes or no), and if participants answered yes to a question, they were identified as having a need for that adjustment. Responses were not ranked if survivors answered yes to multiple questions.
Health-related quality of life
Patients answered two HRQoL questionnaires from the European Organization for Research and Treatment of Cancer (EORTC) [28, 29]. The EORTC core questionnaire (EORTC QLQ-C30) consists of five functional scales, nine symptom scales, and one global QoL scale. The HNC module (EORTC QLQ-HN35) includes questions related to symptoms and problems specific to patients with HNC and includes 18 symptom scales. Both questionnaires have been validated and are used extensively in research. Most of the questions are answered on a 4-point Likert scale with the answers “not at all,” “a little,” “quite a bit,” and “very much.” Through linear transformation, the answers were converted to a score ranging from 0 to 100. High scores on the functional scales and on the global QoL scale indicated a high level of QoL, whereas high scores on the symptom scales indicated poor QoL with a high level of symptoms or problems. A difference in score of 10 or more points was considered to indicate a clinically relevant difference [30].
For this study, scales related to nutritional problems and general HRQoL were analyzed. From the EORTC QLQ-C30 scales regarding global QoL, physical, role, emotional, and social functioning, fatigue, and appetite loss were presented together with scales regarding problems with local pain, swallowing, senses, social eating, teeth, opening mouth, dry mouth, and sticky saliva from the EORTC QLQ-HN35. The participants’ HRQoL was compared to age- and sex-matched reference values from a normal Swedish population [31]. A subgroup representing participants with most difficulty swallowing solid food was analyzed separately and included participants who answered, “quite a bit” or “very much” to the question “Have you had problems swallowing solid food?” from the EORTC QLQ-HN35.
Statistical analysis
Continuous variables are presented as the mean and standard deviation (SD). Categorical variables are presented as numbers and percentages (%). The reference values from the normal population were age- and sex-matched with those of the study group using a greedy group matching approach. Matching was performed by iteratively selecting the closest individuals from the normal population with the minimum t statistic tested against the study population. For the HRQoL questionnaires, at least 50% of the items on a scale needed to be answered to qualify for analysis. For comparisons between groups, Fisher’s exact test was used for dichotomous variables, the Mantel–Haenszel chi square test for ordered categorical variables, and the chi square test for nonordered categorical variables. Continuous variables were compared using Fisher’s nonparametric permutation test and the mean and SD are presented together with the mean difference and confidence interval. The threshold for statistical significance was a two-sided p value of 0.05. Analyses were performed via SAS*®* version 9.4 TS Level 1M6 (Cary, NC, USA).
Results
Patient characteristics
Among the 178 eligible survivors, 114 completed the study, and a flowchart of the inclusion process is presented in Fig. 1. Time since diagnosis ranged from 6.0 to 11.6 years. The mean age at the time of the study was 67 years and ranged from 38 to 89 years, and the majority were male (Table 1). The most common tumor sites were the oropharynx (46%) and oral cavity (29%). Compared with the entire study group, participants with oropharyngeal cancer were younger, and most of those in the oral cancer group were women. Stage III–IV cancer was most common in the study group, but stage I–II disease was most common among oral cancer survivors. Most participants had received radiotherapy (RT) + systemic therapy, followed by surgery alone and surgery + RT. Compared with the entire study group, more participants with oropharyngeal cancer received RT + systemic therapy, whereas most of the participants with oral cancer had been treated with surgery. The majority of participants had a Karnofsky performance status (KPS) score of 100, and most of the participants who lived alone and were former smokers had been diagnosed with oral cancer (Table 1).Fig. 1. Flowchart of study inclusionTable 1Participant characteristicsVariableTotal n = 114Oropharynx n = 52Oral cavity n = 33Years since diagnosis7.5 (SD 0.7)7.6 (SD 0.5)7.3 (SD 1.0)Age (years at follow-up)67.2 (SD 9.9)65.1 (SD 7.6)68.8 (SD 11.9) < 70 years65 (57)39 (75)12 (36) ≥ 70 years49 (43)13 (25)21 (64)Female41 (36)11 (21)18 (54.5)Male73 (64)41 (79)15 (45.5)Tumor siteOropharynx52 (46)Oral cavity33 (29)Larynx10 (9)HNC of unknown primary6 (5)Salivary glands5 (4)Nasal cavity/sinus4 (3)Hypopharynx2 (2)Nasopharynx2 (2)Stage* I–II43 (38)4 (8)26 (79) III–IV71 (62)48 (92)7 (21)Treatment** Surgery23 (20)0 (0)21 (64) Radiotherapy (RT)12 (10)5 (9)0 (0) Surgery + RT ± systemic therapy27 (24)3 (6)12 (36) RT + systemic therapy52 (46)44 (85)0 (0)Karnofsky performance status score 10068 (60)33 (63.5)20 (61) 9027 (24)12 (23)6 (18) 8014 (12)6 (11.5)4 (12) 704 (3)1 (2)2 (6) 601 (1)0 (0)1 (3)Living situation Alone39 (34)14 (27)16 (48) Together with partner and/or children75 (66)38 (73)17 (52)Smoking Never smoker51 (45)29 (56)11 (33) Former smoker59 (52)22 (42)19 (58) Current smoker4 (3)1 (2)3 (9)For continuous variables, the mean (SD) is presented, and for categorical variables, the number (%) is presented.SD standard deviation*Staging according to the Union for International Cancer Control TNM classification of malignant tumors, 7th edition**Treatment: 10 participants had received treatment for recurrence. Out of the 50 participants receiving surgery, 36 had resection of the primary tumor and neck dissection, 10 had only primary tumor resection, and 4 only neck dissection. In total, 15 reconstructions (regional or free flap) were performed; 11 as part of the primary treatment, and 4 as part of recurrence treatment. Out of 91 participants receiving radiation, 87 were treated with IMRT and 4 participants with larynx cancer received 3D conformal RT. Out of 62 patients receiving systemic therapy, 55 were treated with cisplatin, 5 with cetuximab, and 2 with cisplatin and cetuximab. Two patients were treated with laryngectomy—one hypopharyngeal cancer and one oropharyngeal cancer after recurrence. For the remaining two participants with oropharyngeal cancer who received surgery, one received neck dissection, and one underwent resection of recurrence, including reconstruction with free flap and neck dissection
Nutritional status and physical performance
In total, 87 participants reported that they used dietary adjustments to facilitate food intake (Fig. 2). Thirty-five participants reported using three adjustments to facilitate food intake, while 30 participants reported a need for two adjustments. The two most common adjustments were the need for extra liquid with meals and/or the need for moist food and increased time to consume meals. Only six participants reported that they needed to adjust the texture of the food; of those, five needed mashed/soft food, and one needed pureed food (Fig. 2). Twelve participants used ONSs regularly as a complement to their diet, three participants received nutrition via percutaneous endoscopic gastrostomy (PEG), and 16 participants had contact with a dietitian at least yearly.Fig. 2. Among 114 participants, 87 reported a need for dietary adjustments to facilitate food intake. These 87 survivors reported a total of 207 adjustments. Three dietary adjustments were most common, followed by 2 adjustments. The answers to the questions about adjustments were solely based on the participants’ perceptions. “Other adjustments” included the use of saliva gel and not eating warm food. The three patients with PEG could not answer the questions, as their oral intake was nonexistent or sparse (taste portions), and they were not included in the figure. Two of these three participants stated that the small amount of food taken orally needed to be adjusted to a puree or liquid consistency
The participants’ body weight ranged widely from 45.5 to 141 kg, their BMI ranged from 17.9 to 48.1 kg/m^2^, and approximately 50% were considered overweight or obese (Table 2). The FFMI ranged from 13.9 to 23.7 kg/m^2^, and seven women and seven men were considered to have reduced muscle mass. In total, 20 participants had a low BMI and/or reduced muscle mass. Of those 20, seven had contact with a dietitian. Muscle strength varied from 13.1 to 67.2 kg, and one female and one male were considered to have reduced muscle strength. Maximum walking speed ranged from 0.8 to 4.1 m/s. No participants were diagnosed with sarcopenia. More participants with lower average weight, low BMI, and reduced FFMI were observed in the oral cancer group. The average muscle mass, muscle strength, and maximum walking speed were similar between the two tumor groups (Table 2). Table 2. Nutritional status and physical performance for the total study population and for the tumor locations of the oropharynx and oral cavityTotal *n *= 114Oropharynx n = 52Oral cavity n = 33Body weight (kg)76.2 (16.4)78.0 (12.8)73.0 (22.2)BMI (kg/m^2^)25.3 (4.0)25.2 (3.1)24.8 (5.1)BMI categories, n (%) < 18.52 (2%)0 (0%)2 (6%)18.5–24.957 (50%)27 (52%)19 (58%)25–29.941 (36%)22 (42%)7 (21%) > 3014 (12%)3 (6%)5 (15%)Low BMI, n (%)16 (14%)4 (8%)9 (27%)FFMI (kg/m^2^)Male19.2 (1.8)19.1 (1.4)19.4 (3.0)Female16.4 (1.4)16.4 (1.1)16.2 (1.1)Reduced FFMI, n (%)14 (12%)3 (6%)7 (21%)Muscle strength (max value, kg)Male45.1 (9.5)46.0 (7.9)44.4 (13.5)Female26.7 (6.4)28.5 (8.0)26.3 (6.1)10-m max walk (m/s)Male2.2 (0.6)2.6 (0.5)2.1 (0.5)Female1.9 (0.5)2.1 (0.5)1.9 (0.4)For continuous variables, the mean (SD) is presented, and for categorical variables, the number (%) is presented. Low BMI = < 20 kg/m^2^ for age < 70 years and < 22 kg/m^2^ for age ≥ 70 years. Reduced FFMI = < 17 kg/m^2^ for men and < 15 kg/m^2^ for women. Missing values: FFMI n = 5.n number, BMI body mass index, FFMI fat-free mass index
Health-related quality of life
Compared with the age- and sex-matched reference values from a normal population, the study participants reported both clinically and significantly greater symptom burden on all scales from the EORTC QLQ-HN35 (Table 3). From the EORTC QLQ-C30, only appetite loss differed significantly, with more problems in the study group than in the reference group, but the difference did not reach 10 points. Prominent problems in the entire study group and in the specific tumor location groups were dry mouth and sticky saliva, with the highest scores reported by the survivors in the oropharyngeal cancer group. Compared with the survivors of oropharyngeal cancer, the participants with oral cancer reported more appetite loss, with a 7.9-point difference. Moreover, problems with swallowing were more severe in the oropharyngeal cancer group, whereas problems with teeth were worse in the oral cancer group (Table 3). Table 3. Health-related quality of life for the total study population and for the tumor locations of the oropharynx and oral cavity, including comparisons to reference values from a normal populationTotal n = 113Reference values n = 456p valueMean difference and CIOropharynx n = 51Oral cavity n = 33EORTC QLQ-C30 Global QoL74.1 (21.0)76.3 (21.8)0.35−2.2 (−6.5; 2.4)77.6 (22.3)73.0 (19.1) Physical functioning88.6 (14.7)86.7 (20.2)0.341.9 (−1.9; 6.0)92.8 (11.7)84.2 (17.5) Role functioning88.6 (22.9)84.8 (27.0)0.173.8 (−1.5; 9.4)92.0 (19.1)86.4 (25.2) Emotional functioning84.1 (20.9)85.1 (19.8)0.60−1.1 (−5.1; 3.2)86.4 (20.3)82.8 (20.2) Social functioning87.0 (23.8)89.1 (21.5)0.39−2.0 (−6.4; 2.6)87.3 (22.8)88.9 (22.3) Fatigue20.6 (22.9)20.0 (22.0)0.760.7 (−4.0; 5.1)18.1 (22.0)22.2 (22.9) Appetite loss8.3 (18.7)4.1 (13.9)0.00914.2 (1.1; 7.1)5.2 (12.2)13.1 (24.9)EORTC QLQ-HN35 Local pain13.4 (18.4)2.9 (8.9) < 0.000110.5 (8.0; 12.7)13.4 (17.3)16.5 (21.7) Swallowing18.6 (19.5)2.3 (7.9) < 0.000116.3 (13.9; 18.5)23.5 (18.2)13.1 (19.5) Senses17.3 (25.5)5.5 (15.4) < 0.000111.7 (7.9; 15.2)17.3 (26.0)15.7 (21.2) Social eating14.1 (21.3)2.9 (10.2) < 0.000111.2 (8.3; 13.7)12.1 (19.0)17.0 (23.6) Teeth21.4 (31.6)10.4 (21.7)0.000211.1 (5.9; 15.9)17.0 (30.1)27.3 (32.8) Opening mouth19.0 (27.5)1.9 (11.1) < 0.000117.2 (13.8; 20.3)19.6 (26.0)19.2 (31.2) Dry mouth48.5 (35.2)14.4 (24.2) < 0.000134.1 (28.5; 39.5)54.9 (32.5)44.4 (36.0) Sticky saliva37.8 (33.0)7.6 (18.5) < 0.000130.2 (25.5: 34.8)43.1 (33.5)26.3 (29.8)For continuous variables, the mean (SD) is presented. For comparisons between the entire study group and the age- and sex-matched reference values from a Swedish normal population, the Fisher’s nonparametric permutation test for continuous variables was used and presented with the mean difference and CI. EORTC QLQ-C30 and QLQ-HN35: A higher score for the global quality of life scale and the function scales reflects better function, and a higher score for the symptom scales represents more problems. Differences between the two groups were considered statistically significant if *p *< 0.05, and clinically relevant if >10 points. CI confidence interval, EORTC QLQ-C30 The European Organization for Research and Treatment of Cancer Quality of Life Questionnaire-Core 30, EORTC QLQ-HN35 The European Organization for Research and Treatment of Cancer Quality of Life Questionnaire-Head and Neck 35
Comparison between survivors with or without problems swallowing solid food
The participants who reported “quite a bit” or “very much” on the question “Have you had problems swallowing solid food?” from the EORTC QLQ-HN35 (n = 26) were compared to the remaining study group (n = 86); two participants did not answer the question (Table 4). Among the 86 participants, 46 reported no problems, and 40 answered “a little” to the question “Have you had problems swallowing solid food?”. Lower KPS scores were more prevalent among the participants with swallowing difficulties. Age, sex, tumor site, stage, and treatment did not differ significantly, but the group with swallowing problems tended to have more survivors with stage III–IV oropharyngeal cancer and multimodal treatment (Table 4). Table 4. Comparison of demographics between survivors with or without problems swallowing solid foodProblems swallowing solid food n = 26No problems swallowing solid food n = 86p valueAge at study follow-up (years)66.7 (SD 11.1)67.4 (SD 9.7)0.77 < 70 years15 (58)49 (57) ≥ 70 years11 (42)37 (43)1.00Female8 (31)33 (38)Male18 (69)53 (62)0.64Tumor site Oropharynx14 (54)37 (43) Oral cavity6 (23)27 (31) Larynx2 (7.5)7 (8) HNC of unknown primary2 (7.5)4 (5) Salivary glands1 (4)4 (5) Nasal cavity/sinus1 (4)3 (4) Hypopharynx0 (0)2 (2) Nasopharynx0 (0)2 (2)0.92Stage* I–II8 (31)37 (43) III–IV18 (69)49 (57)0.11Treatment** Surgery1 (4)22 (26) Radiotherapy (RT)4 (15)7 (8) Surgery + RT ± systemic therapy7 (27)21 (24) RT + systemic therapy14 (54)36 (42)0.096Karnofsky performance status 10013 (50)55 (64) 907 (27)18 (21) 802 (7.5)12 (14) 703 (11.5)1 (1) 601 (4)0 (0)0.048Participants with swallowing problems defined by reporting “quite a bit” or “very much” on the question “Have you had problems swallowing solid food?” from the EORTC QLQ-HN35. For continuous variables, the mean (SD) is presented, and for categorical variables, the number (%) is presented. For comparisons between the groups, Fisher’s exact test was used for dichotomous variables, the Mantel–Haenszel chi-square test for ordered categorical variables, chi-square test for nonordered categorical variables, and Fisher’s nonparametric permutation test for continuous variables. Differences between the two groups were considered statistically significant if p <0.05.SD standard deviation*Staging according to the Union for International Cancer Control TNM classification of malignant tumors, 7th edition
All participants with most difficulties swallowing solid food reported a need for dietary adjustments to facilitate food intake, and the need for three adjustments (61%) was most common. In comparison, 73% of the participants with no or few swallowing difficulties needed to adapt their food intake, with the need for two adjustments (29%) being the most common. In both groups, the most common adjustments were the need for extra liquid with meals and/or the need for moist food and increased time to consume meals. In the group with swallowing problems, seven survivors had contact with a dietitian (including the three survivors with PEG) and four participants used ONSs. None of the nutritional or physical performance variables differed significantly between the two groups (Table 5). However, a greater proportion of participants in the group with swallowing problems had a low BMI and a reduced FFMI (Table 5). Table 5. Comparisons of nutritional status, physical performance, and health-related quality of life between survivors with or without problems swallowing solid foodProblems swallowing solid food n = 26No problems swallowing solid food n = 86p valueMean difference and CIBMI categories (kg/m^2^),* n* (%) < 18.51 (4%)1 (1%)0.84 18.5–24.913 (50%)44 (51%) 25–29.99 (34.5%)32 (37%) > 303 (11.5%)9 (11%)Low BMI, n (%)6 (23%)10 (12%)0.26FFMI (kg/m^2^) Male18.9 (1.6)19.3 (1.9)0.47−0.4 (−1.4; 0.6) Female16.4 (2.0)16.4 (1.2)0.93−0.05 (−1.2; 1.1)Reduced FFMI, n (%)5 (19%)9 (11%)0.45Muscle strength (max value, kg) Male45.0 (10.4)45.3 (9.1)0.92−0.3 (−5.5; 4.8) Female24.6 (4.4)27.3 (6.7)0.29−2.7 (−7.9; 2.2)10-m max walk (m/s) Male2.1 (0.4)2.3 (0.6)0.29−0.2 (−0.5; 0.1) Female1.7 (0.5)2.0 (0.5)0.23−0.2 (−0.6; 0.2)EORTC QLQ-C30 Global QoL72.1 (23.7)75.0 (20.1)0.56−2.9 (−12.0; 6.6) Physical functioning85.1 (19.4)89.6 (13.0)0.20−4.5 (−10.8; 2.2) Role functioning79.5 (33.1)91.4 (18.1)0.037*−11.9 (−21.3; −1.0)* Social functioning75.6 (31.4)90.3 (20.0)0.011*−14.7 (−24.6; −4.2)* Fatigue27.4 (29.0)18.5 (20.5)0.118.9 (−1.7; 18.5) Appetite loss12.8 (19.0)7.0 (18.5)0.245.8 (−3.2; 13.3)EORTC QLQ-HN35 Local pain20.2 (18.6)11.5 (18.0)0.048**8.7 (0.3; 16.3) Senses25.6 (32.1)14.7 (22.8)0.07310.9 (−0.8; 21.7) Social eating31.7 (22.2)8.91 (18.1) < 0.0001**22.8 (13.9; 30.8) Teeth33.3 (37.7)17.8 (28.8)0.045**15.5 (1.6; 28.8) Opening mouth35.9 (33.9)14.0 (23.1)0.0010**21.9 (10.0; 33.3) Dry mouth60.3 (32.7)45.0 (35.3)0.06315.3 (0.0; 31.2) Sticky saliva50.0 (38.0)34.1 (30.7)*0.040**15.9 (1.7; 30.2)Participants with swallowing problems defined by reporting “quite a bit” or “very much” on the question “Have you had problems swallowing solid food?” from the EORTC QLQ-HN35. For continuous variables, the mean (SD) is presented, and for categorical variables, the number (%) is presented. For comparisons between the groups, Fisher’s exact test was used for dichotomous variables and the Mantel–Haenszel chi-square test for ordered categorical variables. The Fisher’s nonparametric permutation test was used for continuous variables and is presented together with the mean difference and CI. EORTC QLQ-C30 and QLQ-HN35: A higher score for the global quality of life scale and the function scales reflects a better function, and a higher score for the symptom scales represents more problems. Differences in HRQoL variables between the two groups were considered clinically relevant if >10 points. Differences between the two groups were considered statistically significant if p <0.05.BMI body mass index, CI confidence interval, FFMI fat-free mass index, EORTC QLQ-C30 The European Organization for Research and Treatment of Cancer Quality of Life Questionnaire-Core 30, EORTC QLQ-HN35 The European Organization for Research and Treatment of Cancer Quality of Life Questionnaire-Head and Neck 35No significant difference but a clinically relevant difference
The participants with swallowing problems reported significantly worse role and social functioning on the EORTC QLQ-C30 (Table 5). They also reported more problems with fatigue, but the difference of 9 points was not statistically significant. For the EORTC QLQ-HN35, the group with swallowing problems reported more problems on all seven scales, and the differences for five of the scales were also statistically significant. The greatest differences between the two groups were found for trouble with social eating and problems with opening the mouth (Table 5).
Discussion
Survivors of HNC are a growing population facing many challenges, and the long-term effects of HNC and its treatment have not been sufficiently researched. To our knowledge, this is one of the first studies to evaluate and describe survivors’ nutritional problems, muscle mass, muscle strength, physical performance, and HRQoL more than 5 years after diagnosis. Survivors were assessed an average of 7.5 years after diagnosis. Almost 80% of participants used dietary adjustments, which is consistent with previous findings from qualitative studies, where HNC survivors, who were mainly assessed within 5 years post-treatment, reported a need for extra liquid, increased time to consume meals, smaller bites, and cutting food into smaller pieces [32–34]. Surprisingly, only six participants in our study reported the need to adjust the texture of the food, suggesting that the other adjustments were sufficient to facilitate eating. Almost 25% of the survivors reported difficulty swallowing solid food, and all of these participants required dietary adjustments. In a large study from the EORTC working group, difficulty swallowing was the second most common self-reported problem among long-term survivors of HNC [35], and in a systematic review of NISs in HNC survivors, dysphagia was the most common long-term side effect described after chemoradiotherapy [5]. These findings suggest that dysphagia and the need for dietary adjustments may persist for a long time and may indicate a need for nutritional support more than 5 years after diagnosis.
The HRQoL of the survivors was compared with age- and sex-matched reference values from a normal population, and the participants scored worse on all scales of the QLQ-HN35, which was consistent with the results observed in a previous study with a follow-up of 5 years after treatment [36]. The HRQoL reported by HNC survivors in the study by Abel et al. [36] was comparable to that of our participants, except for problems with loss of appetite, senses, and dry mouth, for which there was a tendency for fewer symptoms in our study. The high burden of nutrition impact symptoms observed on the QLQ-HN35 might also explain why many patients needed to adjust their food intake. Dry mouth and sticky saliva were pronounced problems in the study group, and a systematic review of nearly 1400 oropharyngeal cancer survivors found clinically important deterioration of these symptoms at least 1 year after treatment (range 1–26 years) [37]. For the two most common tumor locations in the study, oropharyngeal and oral cancer, the results of the QLQ-HN35 were either equal or better for the participants with oral cancer, except for problems with teeth. This difference may be explained by the treatment regimen; most of the participants diagnosed with oropharyngeal cancer had advanced cancer and received combination therapy, whereas the majority in the oral cancer group had stage I–II cancer and received treatment with a single modality. Similarly, the EORTC 1629 study that compared HRQoL between single and multimodal treatments for long-term HNC survivors revealed no differences in functional scale scores, but survivors treated with a single modality reported similar or lower symptom burden [20].
Relatively few participants in the study group used ONS and enteral nutrition, and relatively few had a low BMI, reduced muscle mass, and muscle strength, and none had sarcopenia. Furthermore, no differences in these variables were observed between participants with the most problems swallowing solid food and survivors without swallowing difficulties. Additionally, the mean values for grip strength and maximum walking speed were comparable to reference values [27, 38]. These findings may imply that many survivors may adapt and compensate for their NISs with adjustments to facilitate food intake, and we speculate that this adaptation allows the majority to meet energy and nutritional needs and thereby maintain body mass and function. The survivors with most problems swallowing solid food had a greater need for dietary adjustments, poorer social and role function, and significantly greater NIS burden. Subgroups of survivors with affected swallowing ability, high NIS burden, and reduced muscle mass may be nutritionally vulnerable, which may imply a need for nutritional rehabilitation. Adaptation to nutritional problems may also result in a “new normal,” where survivors do not recognize that they are still suffering from long-term side effects from treatment [34, 39]. Healthcare professionals may also have to ask questions about dietary adjustments to identify HNC survivors who might need nutritional treatment. In contrast to our results, a pilot study revealed that a lower NIS burden after RT was associated with greater muscle mass and better functional, physical, emotional, and total quality of life [40]. Nevertheless, comparison is difficult since the sample size of the pilot study was small, and the follow-ups varied from 6 months to 9 years after diagnosis. Although the findings in our study suggest that many survivors compensate for their nutritional problems, we do not know whether diet quality might be affected. A hypothesis for future research could be to investigate whether long-term nutritional problems experienced by HNC survivors may lead to negative effects on nutritional intake, for example, a high intake of saturated fat and low intake of vegetables, fruit, and fiber. Other studies have reported lower diet quality scores among HNC survivors than reference values and that higher diet quality is associated with a lower NIS burden and better survival [40–42].
The strengths of this long-term follow-up study are that all HNC survivors were evaluated more than 5 years after diagnosis, and the number of participants included was relatively large, which is uncommon in this patient population. To our knowledge, this was also one of the first long-term follow-ups to evaluate body composition, muscle strength, physical performance, and sarcopenia. Limitations include the cross-sectional study design, with no information about causality or changes over time. No information was collected on survivors who declined participation, and we do not know whether these differed from the study group, which poses a risk of selection bias. The questions about dietary adjustments were based on extensive clinical experience but were not validated. The subgroups that were based on tumor location and swallowing difficulties were relatively small, and the analyses were explorative, which may have affected the generalizability of the study.
Conclusion
In conclusion, this cross-sectional study revealed that many long-term survivors of HNC, on average 7.5 years after diagnosis, experienced chronic nutrition impact symptoms and worse HRQoL than a matched reference group from the normal population. Relatively few patients used ONSs and enteral nutrition, and relatively few were considered to have reduced BMI, muscle mass, and muscle strength. The findings suggest that the majority of survivors with nutritional problems may have developed coping strategies and used dietary adjustments to ease food intake. However, for some survivors, nutritional rehabilitation may be needed long after treatment has ended, focusing on nutrition impact symptoms related to HRQoL and the management of eating difficulties.