Effect of Belimumab on the Cutaneous Manifestations of Patients With Lupus Erythematosus
Diana Schellin, Sarah Rösing, Nick Zimmermann, Nicolai Leuchten, Martin Aringer, Claudia Günther

TL;DR
Belimumab significantly reduces skin symptoms in lupus patients over time, especially those with acute or discoid cutaneous lupus.
Contribution
This study provides evidence of belimumab's long-term efficacy in managing cutaneous lupus symptoms.
Findings
Belimumab significantly reduced CLASI and RCLASI scores over 60 months of treatment.
30% of patients achieved a CLASI 100 response after 60 months.
Patients with acute or discoid cutaneous lupus showed the most significant improvement.
Abstract
The aim was to assess the long‐term effect of belimumab on the cutaneous manifestations of patients with systemic lupus erythematosus (SLE). The retrospective analysis included 29 patients with SLE. Cutaneous disease activity was assessed using the Cutaneous Lupus Erythematosus Disease Area and Severity Index (CLASI) and the Revised CLASI (RCLASI) activity scores before treatment with belimumab and at 3, 6, 12, and up to 60 months of treatment. Eleven patients were treated for the whole observation period; however, only 8 patients were evaluable at 48 months, and only 6 at 60 months due to loss of follow‐up. Compared to the baseline score, a significant reduction of the CLASI and RCLASI activity score was seen during the treatment (mean CLASI baseline 8.76 ± 5.12, after 3 months 5.59 ± 3.87, p < 0.001, after 60 months 4.67 ± 3.86, p = 0.017; mean RCLASI baseline 10.93 ± 6.57, after 3…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
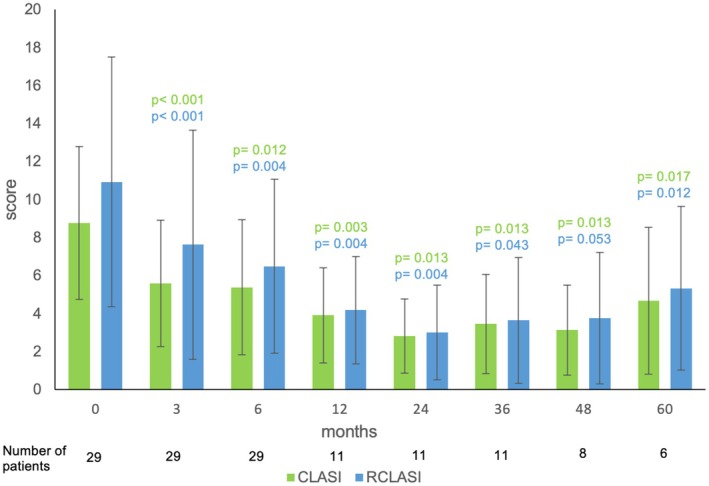 FIGURE 1
FIGURE 1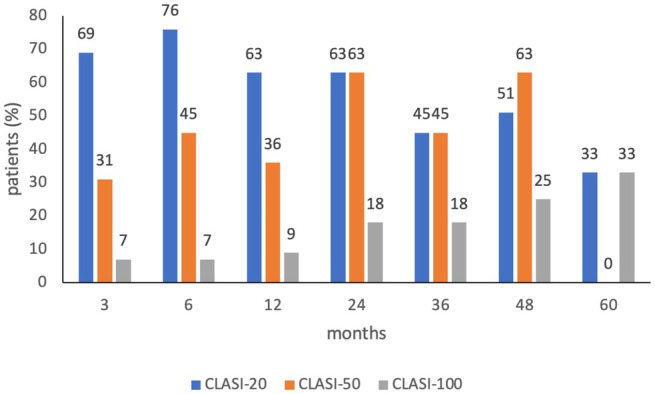 FIGURE 2
FIGURE 2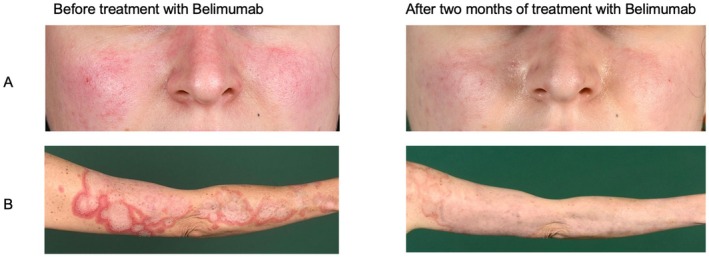 FIGURE 3
FIGURE 3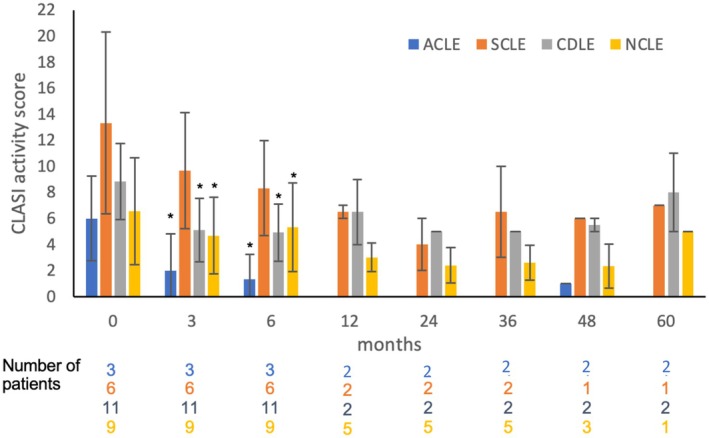 FIGURE 4
FIGURE 4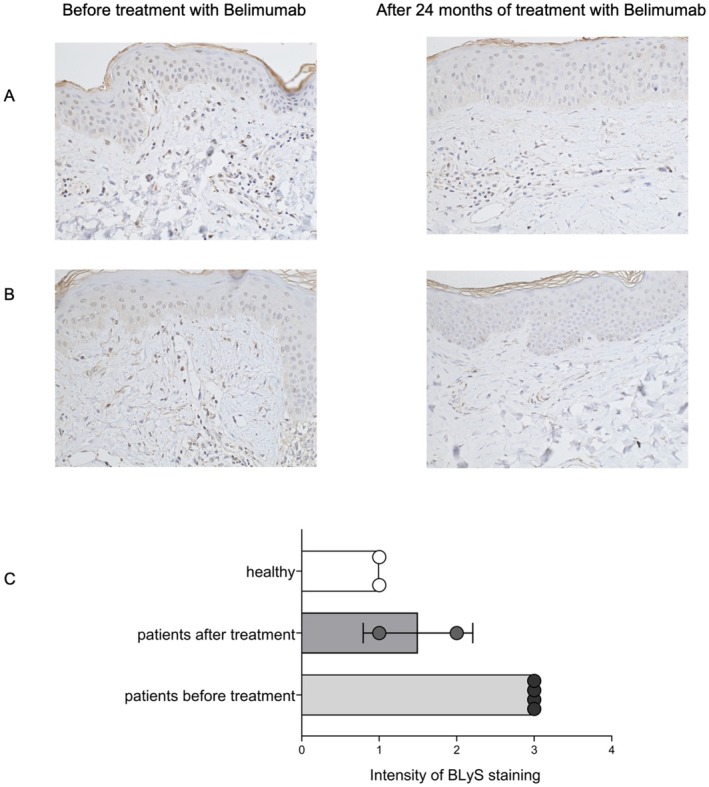 FIGURE 5
FIGURE 5| Total | 29 (100) |
|---|---|
| Gender, | |
| Female | 28 (97) |
| Male | 1 (3) |
| Age, years | |
| Mean (SD) | 41.3 (12.2) |
| Median (range) | 39.0 (25.0–74.0) |
| Duration of disease | |
| Mean (SD), years | 9.9 (10.7) |
| Median (range), years | 5.0 (1.0–47.0) |
| ≤ 5 years, | 15 (51.7) |
| > 5 years, | 14 (48.3) |
| LE subtype, | |
|
Acute cutaneous LE Subacute cutaneous LE Chronic discoid LE Non‐specific skin lesions in LE |
3 (10.3) 6 (20.7) 11 (37.9) 9 (31.0) |
| CLASI activity | |
| Mean (SD) | 8.76 (5.12) |
| Median (range) | 8 (2–28) |
| RCLASI activity | |
| Mean (SD) | 10.93 (6.57) |
| Median (range) | 10 (1–28) |
| Severity | |
| Mild | 20 (68.97) |
| Moderate to severe | 9 (31.03) |
| Adverse events |
| % |
|---|---|---|
| None | 8/29 | 28 |
| Swelling of the lip | 1/29 | 3 |
| Loss of appetite | 2/29 | 7 |
| Increase of appetite | 2/29 | 7 |
| Arthralgia | 4/29 | 14 |
| Occurrence of warts | 1/29 | 3 |
| Autoinflammatory syndrome | 1/29 | 3 |
| Vomiting | 2/29 | 7 |
| Exanthema | 1/29 | 3 |
| Queasy feeling | 1/29 | 3 |
| Urinary tract infection | 4/29 | 14 |
| Herpes zoster | 2/29 | 7 |
| Headache | 5/29 | 17 |
| Circulatory insufficiency | 1/29 | 3 |
| Local erythema | 1/29 | 3 |
| Local itching | 2/29 | 7 |
| Local wheals | 1/29 | 3 |
| Metallic taste after injection | 1/29 | 3 |
| Fatigue | 1/29 | 3 |
| Upper respiratory infection | 11/29 | 38 |
| Pneumonia | 1/29 | 3 |
| Fungal infection | 2/29 | 7 |
| Foetor ex ore | 1/29 | 3 |
| Swelling of the face, tongue | 1/29 | 3 |
| Vertigo | 2/29 | 7 |
| Nausea | 1/29 | 3 |
- —GlaxoSmithKline10.13039/100004330
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSystemic Lupus Erythematosus Research · Rheumatoid Arthritis Research and Therapies · Multiple Sclerosis Research Studies
Introduction
1
Systemic lupus erythematosus (SLE) is a chronic inflammatory autoimmune disease. The skin of patients with SLE is very frequently affected. These cutaneous manifestations have a broad spectrum, ranging from acute to subacute to chronic, and include non‐specific lupus lesions, such as vasculitis [1].
Cutaneous lupus manifestations can be very painful, mutilating, and stigmatizing, often representing a great psychological burden for the patients [2]. Even maximal standard therapy can sometimes not adequately control the disease [3]. Biologics such as belimumab can reduce cutaneous lesions but are currently only approved for antibody‐positive SLE [4].
Belimumab is a human IgG1 antibody that blocks the soluble B‐lymphocyte stimulator protein (BLyS), also known as BAFF, thereby preventing BLyS from binding to its receptor on B cells [5]. In the pivotal studies of belimumab (BLISS‐52, BLISS‐76), positive effects on the skin were observed, but no validated activity scores for skin lesions were used [6]. There are still very few retrospective studies on the effects of belimumab explicitly on the skin [7, 8]. In particular, long‐term results in a real‐world setting are rare. Therefore, this analysis aimed to examine the effect of belimumab on cutaneous manifestations in SLE patients.
Methods
2
Analysis and Design
2.1
A total of 29 patients with SLE were included in the retrospective analysis. All patients were recruited from the Department of Dermatology and the Division of Rheumatology, Department of Medicine III, at the Center for Autoimmune and Rheumatic Diseases, University Medical Centre Dresden, Germany. Patients gave their informed consent, and ethical approval was obtained. The patients were either given 200 mg belimumab subcutanously per week or intravenously in a dosage of 10 mg/kg body weight on Days 0, 14, 28, and every 4 weeks after that. All of the 29 patients were treated with belimumab for at least 6 months. The patients' skin was assessed using the Cutaneous Lupus Erythematosus Disease Area and Severity Index (CLASI) and the Revised CLASI (RCLASI) scores before treatment with belimumab and at 3, 6, 12, 24, 36, 48, and 60 months after treatment. Eleven patients were treated for 60 months, but only 8 patients were evaluable at 48 months and only 6 at 60 months due to loss of follow‐up.
Patient Population
2.2
The inclusion criteria were clinically and/or histologically confirmed lupus erythematosus (EULAR/ACR criteria), age over 18 years, and active cutaneous manifestations of lupus erythematosus (CLASI ≥ 2). Patients were excluded if the following criteria were met: treatment with belimumab for less than 3 months, no consistent description of skin activity in the patient file, non‐compliant patients, or patients with lupus erythematosus but without skin involvement. A patient flowchart is shown in Figure S1. The key clinical and demographic characteristics of the patients are presented in Table 1.
Measurement Instruments
2.3
In the present analysis, the CLASI activity score [9, 10], was used as a measurement tool for assessing skin lesions and was measured prior to treatment with belimumab.
The Revised Cutaneous Lupus Erythematosus Disease Area and Severity Index (RCLASI) is a revised score of the CLASI. It enables a more detailed assessment of rare CLE subtypes [11]. Both the CLASI and the RCLASI activity scores were used in this analysis as measurement instruments for the therapeutic response.
Immunohistochemistry
2.4
Skin tissue samples were deparaffinized and incubated with the rat anti‐human BAFF antibody (Novus Biologicals, NBP1‐97622) for 60 min at room temperature. As a secondary antibody, goat anti‐rat IgM HRP (ThermoFisher, 31,476) was used for 20 min at room temperature. Thereafter, the slides were washed with PBS and stained with ImmPACT DAB Peroxidase Substrate (VectorLabs). The slides were then incubated in Mayer's hemalum solution (Engelbrecht Medizin‐und Labortechnik GmbH) for 50 s. After dehydration, the slides were mounted in CellTexx mounting medium (Engelbrecht Medizin‐und Labortechnik GmbH) and analyzed with a microscope. Scoring was defined as 3 for intense staining, 2 for medium staining, and 1 for low staining intensity. The findings were validated by two independent and blinded investigators through the analysis of staining of different CLE lesions before and after therapy.
Statistical Analysis
2.5
Data were tested for normal distribution by the Shapiro–Wilk test. Means and standard deviations of the CLASI and RCLASI activity scores were calculated for the time points t = 0, 3, 6, 12, 24, 36, 48, and 60 months, and then compared to the respective mean value at t = 0. Afterward, the ANOVA was used due to multiple measurement time points. In all performed tests, values of p ≤ 0.05 were considered statistically significant. As a post hoc test, Bonferroni's least significant difference was used.
Results
3
Cutaneous Lesions Improve During Treatment With Belimumab
3.1
Patients with uncontrolled SLE and cutaneous involvement were treated with belimumab and had their CLASI scores routinely assessed every 3 months for 1 year and annually thereafter. During the treatment, the CLASI activity score decreased significantly at all measured time points. Mean CLASI before treatment was 8.76, and RCLASI was 10.93. By 3 months, CLASI and RCLASI declined to 5.59 (p < 0.001) and 7.62 (p < 0.001), respectively, after 6 months to 5.38 (p = 0.012) and 6.48 (p = 0.004), respectively, after 12 months to 3.91 (p = 0.003) and 4.18 (p = 0.004), respectively, after 24 months to 2.82 (p = 0.013) and 3.00 (p = 0.004), respectively, after 36 months to 3.45 (p = 0.013) and 3.64 (p = 0.043), respectively, after 48 months to 3.13 (p = 0.013) and 3.75 (p = 0.053), respectively, and after 60 months to 4.67 (p = 0.017) and 5.33 (p = 0.012), respectively. The time course of the CLASI and RCLASI activity score during the treatment is shown in Figure 1.
CLASI and RCLASI activity scores before and during treatment with belimumab. The means and SD are demonstrated. The number of patients is indicated. Differences were tested against time point 0 before treatment and assessed by ANOVA.
A CLASI‐20 response, indicating at least 20% reduction of CLASI, was achieved in 19 patients (64%) after 3 months, in 21 patients (72%) after 6 months, in 8 patients (72%) after 12 months, in 9 patients (81%) after 24 months, in 7 patients (63%) after 36 months, in 6 patients (76%) after 48 months, and in 4 patients (66%) after 60 months, respectively (Figure 2). A CLASI‐50 response, indicating at least 50% reduction of CLASI, was achieved in 5 patients (16%) after 3 months, in 13 patients (44%) after 6 months, in 4 patients (36%) after 12 months, in 7 patients (63%) after 24 months, in 5 patients (45%) after 36 months, in 5 patients (63%) after 48 months, and in 2 patients (33%) after 60 months, respectively (Figure 2). A CLASI‐100 response, i.e., complete remission of lupus activity in skin, was achieved in 4 patients (13%) after 3 months, in 4 patients (13%) after 6 months, in 1 patient (9%) after 12 months, in 2 patients (18%) after 24 months, in 2 patients (18%) after 36 months, in 2 patients (25%) after 48 months, and in 2 patients (33%) after 60 months, respectively (Figure 2).
CLASI‐20, CLASI‐50, and CLASI‐100 during treatment with belimumab. Values indicate the percentage of patients achieving 20%, 50%, or 100% improvement of CLASI.
Examples of the clinical response in acute and subacute CLE lesions are demonstrated in (Figure 3).
Clinical images before and after treatment with belimumab. Patient A presented with a distinct butterfly rash on her face prior to starting belimumab treatment. After 2 months of treatment with belimumab, the butterfly rash started to resolve. The right arm of Patient B showed rounded, garland‐like erythema with a central lightening and slight scaling. After 2 months of treatment with belimumab, the erythema and scaling had decreased significantly.
After measuring the improvement of cutaneous lupus lesions during treatment with belimumab, we asked whether subgroups of CLE responded differentially to therapy. Therefore, the CLASI and RCLASI response was assessed separately for ACLE (acute cutaneous lupus erythematosus, n = 3), SCLE (subacute cutaneous lupus erythematosus, n = 6), CDLE (chronic discoid lupus erythematosus, n = 11), and NCLE (non‐specific skin lesions in lupus erythematosus, n = 9) (Figure 4). Data show that patients with ACLE, CDLE, and NCLE had a significant reduction in CLASI activity score after 3 months (p = 0.018, p = 0.002, p = 0.033) and after 6 months (p = 0.037, p = 0.003, p = 0.033), respectively. In contrast, no significant reduction in CLASI activity score was observed in SCLE patients after 3 or 6 months of treatment (p = 0.121, p = 0.115). After 12 months, no significant reduction was observed in either subtype. A limitation of the analysis is the small number of patients in each subset.
CLASI activity scores of the lupus subtypes ACLE, SCLE, CDLE, and NCLE during treatment with belimumab. ACLE—acute cutaneous lupus erythematosus, SCLE—subacute cutaneous lupus erythematosus, CDLE—chronic discoid lupus erythematosus, NCLE—non‐specific cutaneous skin lesions in lupus erythematosus. Shown are the mean and SD. Differences were tested against time point 0 before treatment and assessed by ANOVA. p < 0.05.
Cutaneous BLyS Expression Is Reduced During Belimumab Therapy
3.2
Skin biopsies were available from four patients before and two patients 2 years after treatment. In each of the samples, BLyS was immunohistochemically stained. The evaluation was based on a score with 1 = weak expression of BLyS, 2 = moderate expression of BLyS, and 3 = high expression of BLyS. The skin samples of healthy subjects showed no to little expression of BLyS. In contrast, SLE skin samples exhibited obvious BLyS expression, consistent with the study by Wenzel et al. (2018) [12], which demonstrated that BLyS is not only elevated in the serum of lupus patients but also in their skin lesions. After 2 years of treatment with belimumab, the amount of BLyS detected by immunohistochemistry staining in skin was reduced (Figure 5). This suggests that BLyS expression in skin is reduced by systemic application of belimumab in lupus patients.
Immunohistochemical staining of BLyS. Magnification 200×. Expression of BLyS (brown) is seen in epidermis and dermis and is reduced after 24 months of treatment with belimumab. Intensity of BLyS staining is demonstrated.
Belimumab Was Well Tolerated During Treatment
3.3
Belimumab was well tolerated by all patients included in the retrospective analysis. Eight patients had no adverse effects. Common adverse events included upper respiratory infections (n = 11), headache (n = 5), urinary tract infections (n = 4), and arthralgia (n = 4). Two patients had to pause belimumab for a short time due to respiratory infections, but were then able to continue treatment without complications. No patient had to discontinue the therapy completely due to intolerance or adverse effects. However, several patients stopped treatment due to personal reasons. One patient discontinued therapy early due to a planned pregnancy. All reported adverse events are listed in Table 2.
Discussion
4
Herein, we present a retrospective long‐term analysis of cutaneous lupus manifestations in patients receiving belimumab for up to 60 months in a real‐life setting at a university center. Overall, we observed a continuous and significant response of cutaneous lupus lesions under belimumab treatment. This finding aligns with previous reports demonstrating a decrease in CLASI and RCLASI activity scores after three and 6 months [13]. Iaccarino et al. also performed an analysis of the response in CLE subtypes and showed a significant reduction of the CLASI activity score in patients with ACLE and SCLE during treatment with belimumab. While our data support the finding in ACLE, the SCLE subgroup analysis did not show a significant decline during treatment. This may be related to the small number of SCLE patients analyzed in the study by Iaccarino (n = 5) and our analysis (n = 6). Interestingly, in a larger cohort, preliminary data from the same group showed a significant reduction in CLASI activity score in acute and subacute CLE after 6 months [14]. In this analysis, cutaneous involvement was limited as indicated by mean CLASI activity scores at baseline between 3.5 and 6. After 6 months, the scores declined to a mean value of 2. Further analysis did not demonstrate a further significant reduction in ACLE and SCLE, which is most likely related to the low level of cutaneous involvement. Though the sizes of the subgroups are small, they should be interpreted with caution.
The findings in this work suggest that belimumab continues to reduce skin activity even after long‐term use, which supports the study by Zen et al. (2023) [8]. Zen et al. showed that 4.5% of patients achieved CLASI remission after 6 months and 20% of patients after 24 months. Our data showed a slightly higher CLASI remission rate after 6 months of treatment, but a nearly identical percentage of CLASI remission after 36 months. We can also demonstrate that even after 60 months of treatment, 33% of patients achieved a CLASI‐100 score. The CLASI‐50 results in our work are similar to those reported by Zen et al., with our data also showing a 33% reduction in CLASI‐50 scores for patients after 60 months.
This strengthens the long‐term results of our observation. However, a limitation of our analysis is the small sample size as well as the retrospective design. More studies with a larger patient population are needed to confirm the findings in this work.
We confirmed that in the subjects from whom skin samples were taken, BLyS was elevated in lesional skin samples before treatment. Cutaneous BLyS expression had been shown previously by Wenzel et al. (2018) [12], who demonstrated that BLyS is not only elevated in the serum of lupus patients. During treatment with belimumab, the BLyS expression in skin was reduced, indicating that lesional BLyS expression might be suitable as a biomarker. Due to the small patient cohort, this finding is preliminary and should be confirmed in larger trials.
In comparison to anifrolumab, which induced fast CLASI reduction following a four‐week treatment period [15, 16], the effects of belimumab appear to be achieved at a more gradual rate. However, it is worth noting that there is currently a lack of direct comparative studies between the two treatments. Here, it was demonstrated that belimumab led to a further reduction in CLASI activity score with increasing duration of treatment. It is essential to note that long‐term data for anifrolumab are not yet available.
Deucravacitinib, a tyrosine kinase 2 inhibitor, has been shown to achieve a CLASI‐50 response in a phase II trial [17]. However, long‐term efficacy and safety have yet to be analyzed, making belimumab, as of now, a preferred option in the treatment of systemic lupus with cutaneous involvement.
Overall, belimumab was well tolerated. Common adverse events included upper respiratory infections, headache, and arthralgia, among others. In two patients, treatment was briefly paused due to adverse events but could be continued without complications after the symptoms had subsided. No patient required total discontinuation of belimumab due to side effects. The adverse event profile in this analysis was consistent with recent studies on the safety of belimumab [18, 19].
In conclusion, these real‐world data demonstrated an effective and safe long‐term improvement of the cutaneous manifestations of patients with lupus erythematosus treated with belimumab. Nevertheless, further investigation is warranted to substantiate these observations with larger sample sizes.
Funding
This study was partially funded by a research grant from GSK awarded to Claudia Günther.
Conflicts of Interest
C.G. received honoraria for presentations and advisory boards from GSK, AstraZeneca, Boehringer Ingelheim, Janssen, and UCB.
Supporting information
Figure S1: Patient flowchart. ACLE‐ Acute Cutaneous Lupus Erythematosus. SCLE‐ Subacute Cutaneous Lupus Erythematosus. CDLE‐ Chronic Discoid Lupus Erythematosus. NCLE‐ Non‐specific skin lesions in Lupus Erythematosus. Table S1: Number of evaluable patients and reasons for missing data.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1M. Aringer , “Kurze Einführung in Klinik, Diagnose Und Aktivitätsmessung,” in Aktuelle Therapieoptionen Beim Systemischen Lupus Erythematodes, 4th ed., ed. M. Aringer , T. Dörner , S. Finzel , R. Fischer‐Betz , W. B. Graninger , and C. Günther (UNI‐MED Verlag, 2022).
- 2P. Vashisht , K. Borghoff , J. R. O'Dell , and M. Hearth‐Holmes , “Belimumab for the Treatment of Recalcitrant Cutaneous Lupus,” Lupus 26, no. 8 (2017): 857–864, 10.1177/0961203316682097.28121495 · doi ↗ · pubmed ↗
- 3R. Fruchter , D. Kurtzman , M. Patel , et al., “Characteristics and Alternative Treatment Outcomes of Antimalarial‐Refractory Cutaneous Lupus Erythematosus,” JAMA Dermatology 153, no. 9 (2017): 937–939, 10.1001/jamadermatol.2017.1160.28636714 PMC 5817470 · doi ↗ · pubmed ↗
- 4European Medicines Agency , “Benlysta,” (2021), https://www.ema.europa.eu/en/medicines/human/EPAR/benlysta.
- 5H. A. Blair and S. T. Duggan , “Belimumab: A Review in Systemic Lupus Erythematosus,” Drugs 78, no. 3 (2018): 355–366, 10.1007/s 40265-018-0872-z.29396833 · doi ↗ · pubmed ↗
- 6A. Fanouriakis , M. Kostopoulou , A. Alunno , et al., “2019 Update of the EULAR Recommendations for the Management of Systemic Lupus Erythematosus,” Annals of the Rheumatic Diseases 78, no. 6 (2019): 736–745, 10.1136/annrheumdis-2019-215089.30926722 · doi ↗ · pubmed ↗
- 7A. J. Petty , L. Floyd , C. Henderson , and M. W. Nicholas , “Cutaneous Lupus Erythematosus: Progress and Challenges,” Current Allergy and Asthma Reports 20, no. 5 (2020): 12, 10.1007/s 11882-020-00906-8.32248318 PMC 7548961 · doi ↗ · pubmed ↗
- 8M. Zen , M. Gatto , R. Depascale , et al., “Early and Late Response and Glucocorticoid‐Sparing Effect of Belimumab in Patients With Systemic Lupus Erythematosus With Joint and Skin Manifestations: Results From the Belimumab in Real Life Setting Study‐Joint and Skin (Be R Li SS‐JS),” Journal of Personalized Medicine 13, no. 4 (2023): 691, 10.3390/jpm 13040691.37109077 PMC 10146447 · doi ↗ · pubmed ↗