Exploration of factors associated with turnaround time when evaluating non-tuberculous mycobacterium cultures
Xingxing Lou, Sheng Zhao, Sipei Wang, Shanshan Jin, Tinghua Ye, Xinling Pan

TL;DR
This study identifies factors affecting the time it takes to diagnose non-tuberculous mycobacteria infections, aiming to improve clinical decision-making.
Contribution
The study identifies acid-fast bacilli smear results as the key determinant of culture turnaround time for non-tuberculous mycobacteria.
Findings
Rapidly growing mycobacteria have shorter turnaround times than slow-growing mycobacteria.
Acid-fast bacilli smear results are the only independent factor affecting turnaround time.
Clinical diagnoses and imaging findings correlate with shorter turnaround times.
Abstract
A positive culture of non-tuberculous mycobacteria (NTM) is a key diagnostic criterion for NTM disease. Due to the slow growth rate of NTM, the turnaround time (TAT) for culture specimens is often lengthy, posing significant challenges for the diagnosis and treatment of related diseases. This study aimed to explore factors influencing TAT in NTM culture testing, assess its potential clinical value, and identify ways to expedite clinical decision-making. NTM identified by HSP65 sequencing in a tertiary hospital from June 2022 to May 2024 were retrospectively included, and patients’ data were collected. TAT was defined as the time between specimen receipt and report issuance. Differences in TAT between groups were analyzed using the rank-sum test. Correlations were evaluated using Spearman’s correlation analysis, and a generalized linear model was applied to identify independent factors…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
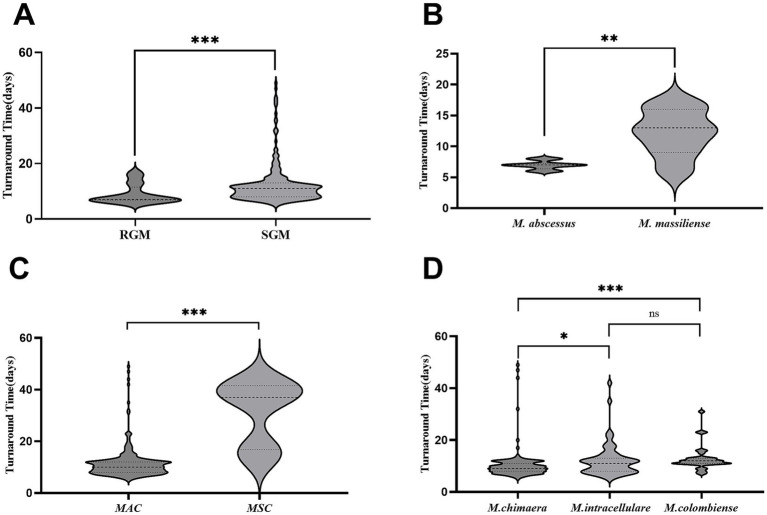 Figure 1
Figure 1| Mycobacterial complexes | Species | Count |
|---|---|---|
| MAC ( |
| 124 |
|
| 33 | |
|
| 65 | |
|
| 3 | |
|
| 6 | |
|
| 5 | |
|
| 8 | |
| MABC ( |
| 14 |
|
| 7 | |
| MSC ( |
| 4 |
|
| 2 | |
| Others ( |
| 3 |
|
| 3 | |
|
| 2 | |
|
| 2 | |
| 8 |
| Features | Variable (number) | Median TAT (IQR), day | ||
|---|---|---|---|---|
| Sex | Male (154) | 10.25 (8–12.25) | −0.053 | 0.958 |
| Female (135) | 10 (8–13) | |||
| Age | ≤60 (48) | 10 (9–13) | 0.514 | |
| 61–70 (80) | 12.25 (8–12.75) | |||
| 71–80 (109) | 10 (7.5–12) | |||
| >80 (51) | 12 (8–13) | |||
| Smoke history | Yes (143) | 11 (8–13) | −1.066 | 0.287 |
| No (146) | 10 (8–12) | |||
| Tuberculosis history | Yes (33) | 9 (7.25–12) | −1.919 | 0.055 |
| No (236) | 11 (8–13) | |||
| NTM-PD | Yes (71) | 8 (7–10) | −5.66 | <0.001 |
| No (278) | 11 (9–13) | |||
| HIV | Yes (20) | 10 (7.25–12) | −0.762 | 0.446 |
| No (269) | 10 (8–13) | |||
| COPD | Yes (55) | 11 (8–13) | −1.105 | 0.269 |
| No (234) | 10 (8–12) | |||
| Bronchiectasis | Yes (81) | 9 (7.25–12) | −2.658 | 0.008 |
| No (208) | 11 (8–13) | |||
| Pulmonary cavity | Yes (55) | 8 (7–10) | −5.03 | <0.001 |
| No (234) | 11 (9–13) | |||
| Lung nodules | Yes (36) | 10.5 (8–12) | −0.09 | 0.928 |
| No (253) | 10 (8–13) | |||
| Tumor | Yes (56) | 1 1 (8–13) | −0.652 | 0.514 |
| No (233) | 10 (8–12) | |||
| Pulmonary surgery | Yes (17) | 9 (7–13) | −0.778 | 0.436 |
| No (272) | 10 (8–12.75) | |||
| Albumin | Normal (72) | 10 (8–12) | −0.003 | 0.998 |
| Low (278) | 10 (8–13) | |||
| Antinuclear antibodies | Positive (68) | 10 (8–12.75) | −0.3 | 0.764 |
| Negative (96) | 10.75 (9–13) | |||
| Rheumatoid factor | Abnormal (28) | 10.5 (7.6–12) | −0.92 | 0.358 |
| Normal (115) | 11 (9–13) |
| Microscopic smear* | Median TAT (IQR), day |
|---|---|
| Negative ( | 11 (9–13) |
| Few ( | 7.5 (6.1–8) |
| 1 + ( | 8 (7–9) |
| 2 + ( | 7 (6–8) |
| 3 + ( | 7 (7–8) |
| 4 + ( | 7.25 |
| Variable | Coefficient (B) | IRR (95% CI) | |
|---|---|---|---|
| AFB smear (positive vs. negative) | −0.493 | 0.61 (0.52–0.71) | <0.001 |
| Mycobacterial species (RGM vs. SGM) | −0.098 | 0.91 (0.74–1.11) | 0.346 |
| NTM-PD (yes vs. no) | 0.067 | 1.07 (0.93–1.23) | 0.340 |
| Pulmonary cavity (yes vs. no) | −0.046 | 0.96 (0.84–1.09) | 0.521 |
| Bronchiectasis (yes vs. no) | −0.068 | 0.93 (0.84–1.04) | 0.230 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMycobacterium research and diagnosis · Tuberculosis Research and Epidemiology · Diagnosis and treatment of tuberculosis
Introduction
1
Non-tuberculous mycobacteria (NTM) refer to mycobacteria other than members of the Mycobacterium tuberculosis complex and Mycobacterium leprae (1). NTM are classified into rapidly growing mycobacteria (RGM) and slow-growing mycobacteria (SGM) (2). Further categorization includes specific complexes or groups, such as the Mycobacterium avium complex (MAC), Mycobacterium abscessus complex (MABC), and Mycobacterium simiae complex (MSC) (3).
NTM are opportunistic pathogens that can cause lesions in various tissues and organs, collectively referred to as NTM disease. Among these, NTM pulmonary disease (NTM-PD) is the most common and is increasing in incidence worldwide (4). In some countries, NTM infection rates currently exceed those of the M. tuberculosis complex (5). Therefore, efficient isolation and detection of NTM are essential. In the majority of hospitals, particularly primary care facilities, NTM detection relies on conventional mycobacterial culture. Due to the slow growth of NTM, it often takes several days or weeks for laboratories to issue reports, resulting in prolonged turnaround time (TAT). This delay poses significant challenges for the timely diagnosis and treatment of NTM-related diseases. TAT, defined as the interval from specimen receipt to report delivery (6), is a widely used metric for assessing laboratory efficiency (7, 8). However, few studies have explored TAT specifically for NTM.
Previous studies have shown that the time to positive (TTP) in mycobacterial culture is negatively correlated with acid-fast bacilli (AFB) smear grades and colony numbers (9). In addition, TTP has the potential to be a predictive biomarker for M. avium pulmonary disease (10). Unlike TTP, TAT encompasses the entire process from specimen receipt to report issuance, providing a more comprehensive metric. Despite its significance, the impact of various NTM species and host factors on TAT remains poorly understood, prompting this study to investigate these relationships.
Materials and methods
2
Mycobacterial culture and reporting process
2.1
Upon receipt, mycobacterial culture specimens were stored at 4 °C and processed the following morning. Isolation and culture were performed according to standard operating procedures, and the BACTEC MGIT 960 system (BD, USA) was used to detect mycobacteria. Once the instrument reported a positive result, Ziehl–Neelsen staining was performed. For specimens with positive AFB results, MPB64 antigen detection (Chuangxinshengwu, Hangzhou, China) was used for mycobacterial identification. If the MPB64 antigen test was negative, the obtained strains were reported as NTM.
NTM species identification
2.2
Specimens with AFB-positive microscopy but negative MPB64 antigen tests were retained for further NTM species identification. After centrifugation at 10,000 g for 5 min and washing with 500 μL of phosphate-buffered solution (PBS), 200 μL of Tris-EDTA buffer was added, followed by heating at 100 °C for 10 min to prepare the template for polymerase chain reaction (PCR) amplification. The HSP65 gene was amplified, after which the amplification products were verified by gel electrophoresis and processed for Sanger sequencing. Sequences were analyzed using NCBI BLAST, with the highest scoring match being identified as the strain’s species, as described in our previous study (11).
Definition of TAT
2.3
TAT was defined as the time from specimen receipt to NTM report issuance. It included pre-processing, mycobacteria culture, AFB smear, MPB64 antigen testing, and final result delivery (12).
Data collection
2.4
NTM strains were collected between June 2022 and May 2024. For serial strains of the same species from the same patient during a single hospitalization, the mean TAT was used. Collected data included patient demographics, comorbidities, medical history, imaging findings, and laboratory results.
Statistical analyses
2.5
Statistical analyses were performed using SPSS version 26.0. As TAT was non-normally distributed, results were expressed as medians and quartiles. The rank-sum test was used to assess group differences, and Spearman’s correlation analysis was used to assess correlations. The threshold for statistical significance was set at a p-value of < 0.05. Based on the univariate analysis, variables with statistical significance (p < 0.05) or clinical relevance were selected for inclusion in the generalized linear model with a gamma distribution and log link function, to identify independent factors associated with TAT.
Results
3
NTM species identification
3.1
A total of 289 NTM strains were included in the study, comprising RGM (n = 22) and SGM (n = 267). The majority were MAC (n = 244, 84.4%), followed by MABC (n = 21, 7.3%) and MSC (n = 6, 2.1%) (Table 1). Within MAC, the most prevalent species were M. chimaera (n = 124), M. intracellulare (n = 65), and M. colombiense (n = 33).
TAT distributions for different NTM species
3.2
The median TAT for RGM was 7 days [interquartile range (IQR): 6.9–11.5], while the median TAT for SGM was 11 days (IQR: 8–13), representing a statistically significant difference (p < 0.001) (Figure 1A). Among the RGM, the median TAT for M. abscessus (MAB) was 7 days (IQR: 6.4–7.3), which was significantly shorter than that for Mycobacterium massiliense, which was 13 days (IQR: 9–16) (p = 0.005) (Figure 1B). Among SGM, the median TAT for MAC was 10 days (IQR: 8–12), which was significantly shorter than that for MSC, which was 37 days (IQR: 16.8–41.5) (p < 0.001) (Figure 1C). Within the MAC group, the median TAT for M. chimaera was 9 days (IQR: 8–11), which was shorter than that for M. intracellulare (11 days, IQR: 8–13; p = 0.015) and M. colombiense (12 days, IQR: 11–13; p < 0.001). However, there was no statistically significant difference between the median TATs of M. intracellulare and M. colombiense (p = 0.166) (Figure 1D).
*TAT comparisons among bacterial species. (A) TAT comparisons for RGM and SGM. (B) TAT comparisons for M. abscessus and M. massiliense. (C) TAT comparisons for MAC and MSC. (D) TAT comparisons for M. chimaera, M. intracellulare, and M. colombiense. Data are presented as medians, quartiles, maximums, and minimums. Data were compared among independent groups using the Mann–Whitney U test (two groups) and the Kruskal–Wallis test (multiple groups), followed by multiple comparisons using Dunn’s post-hoc test. *p < 0.05, **p < 0.01, **p < 0.001, ns, not significant. TAT, turnaround time; RGM, rapidly growing mycobacteria; SGM, slow-growing mycobacteria; MAC, Mycobacterium avium complex; MSC, Mycobacterium simiae complex.
Clinical factors related to TAT
3.3
TAT values varied significantly among different patient populations. Patients with NTM-PD had a median TAT of 8 days (IQR: 7–10), those with bronchiectasis had a median TAT of 9 days (IQR: 7.25–12), and those with lung cavitation had a median TAT of 8 days (IQR: 7–10). These groups exhibited shorter TATs compared with patients without these conditions (p < 0.05) (Table 2). Additionally, a negative correlation was observed between AFB smear grade and TAT (Spearman’s correlation coefficient = −0.49, p < 0.001) (Table 3).
Independent factors influencing TAT
3.4
In the generalized linear model, the AFB smear result was the only independent factor significantly associated with TAT (Wald χ^2^ = 39.71, p < 0.001). The incidence rate ratio was 0.61 (95% CI: 0.52–0.71), indicating that positive AFB smears were associated with a 39% reduction in TAT. Other variables, including mycobacterial species, NTM-PD, pulmonary cavity, and bronchiectasis, did not show significant independent effects (all p > 0.05) (Table 4).
Discussion
4
Advancements in technology have identified more than 200 types of NTM, but the primary pathogens of NTM disease include MAC, MABC, and Mycobacterium kansasii (13, 14). MABC, which is part of the RGM, typically grows within 3–5 days, whereas MAC, a member of the SGM, requires 1 week or more to grow. Our results align with these observations, with a median TAT of 7 days for MABC and 10 days for MAC, which is consistent with the TTP values reported by Uwamino et al. (15). These findings suggest that TAT reflects strain growth rates, providing useful diagnostic insights.
MABC includes the subspecies MAB, M. massiliense, and Mycobacterium bolletii, which differ in drug susceptibility, making subspecies identification crucial for treatment (15). Our data indicate that MAB grows faster than M. massiliense does, allowing TAT to distinguish between these subspecies—a feature not previously emphasized in the literature. Similarly, TAT can differentiate Mycobacterium chimaera from other MAC subspecies, despite an earlier report suggesting no differences in TTP among MAC members (16). However, the previous study involved smaller sample sizes, potentially introducing bias. Our findings, supported by a larger dataset, highlight the potential of TAT for distinguishing these strains.
MSC, a large complex within the NTM, contains approximately 20 strains (17), which exhibit varying growth requirements (18–20). Despite being SGM, the calculated TAT for MSC was significantly longer than that for MAC. This discrepancy may stem from the limited number of MSC cases (n = 6) in our study, which included only Mycobacterium lentiflavum and Mycobacterium paraense, potentially biasing the results. Another explanation could be the rarity of MSC-associated NTM-PD (21), which complicates isolation and prolongs TAT.
In our study, TAT was significantly correlated with NTM-PD and bronchiectasis. Patients with NTM-PD require at least two positive sputum samples or one positive lavage sample for diagnosis (22). This diagnostic criterion implies a greater bacterial load in the respiratory tract, leading to shorter TTPs, higher AFB smear grades, and consequently shorter TATs. Our data confirmed a strong correlation between TAT and AFB smear grade, and the acid-fast smear result was identified as the key independent factor influencing TAT. Notably, acid-fast bacilli (AFB) smear results were categorized into six grades in the correlation analysis (Table 3). In the generalized multiple linear regression model, however, the AFB smear results were dichotomized into negative and positive (few to 4+) to facilitate clinical interpretation and ensure model stability (Table 4). Although bronchiectasis is not a common susceptibility factor for tuberculosis (13), it is closely associated with NTM disease (23, 24). Conversely, despite previous reports linking NTM disease to underlying conditions such as tuberculosis, chronic obstructive pulmonary disease, and autoimmune diseases (25), our data did not suggest an association between these conditions and the TAT. We hypothesize that the bacterial load in samples has a more direct impact on TAT than the underlying conditions.
According to the American Thoracic Society and the Infectious Diseases Society of America, NTM-PD diagnosis requires a combination of clinical, imaging, and microbiological findings (22, 26). The imaging criteria included nodules or cavitations in the lungs (26). Our data suggest that lung cavitation affects the TAT more than pulmonary nodules do, which may be due to the lack of distinction between nodule size and quantity in our analysis. Additionally, the median TAT in the population with pulmonary cavities was 8 days in our study, which contrasts with the previously reported TTP of 12 days in a smaller cohort (n = 12) (10), suggesting that our larger sample size (n = 55) provides more reliable estimates.
The TTP for the BACTEC MGIT 960 system, which uses an oxygen-quenching fluorescence sensor and a specific algorithm to detect culture positivity (27), has been shown to correlate negatively with AFB smear grade (9, 10), and pretreatment TTP correlates negatively with treatment response (28). Our findings further revealed that TAT correlates with bacterial load, suggesting its potential as a biomarker for therapeutic efficacy, although further research is needed.
Notably, given the limited number of TAT studies in the NTM, we only compared TAT with the TTP in previous literature. The TAT in this study was reduced by 2–3 days to calculate the corresponding TTP. However, there were a small number of cases (n = 6) in which we sequenced the specimens before issuing the report due to unclear smear morphology or findings that were inconsistent with historical results. Therefore, the TAT for these samples was prolonged. In addition, compared with the TTP, the TAT is easily accessible and can be obtained directly from the report sheet (12). The Chinese Basic Technical Standards for Clinical Microbiology Testing (WS/T805-2022) mandates that the laboratory is obligated to report the TAT of the sample. Thus, our exploration of TAT provides valuable insights for the clinical management of NTM.
As an indicator reflecting laboratory efficiency (6, 12), we recommend that each laboratory using the BACTEC MGIT 960 System establishes species-specific TAT benchmarks based on its own circumstances. For instance, the TAT benchmark for RGM could be set at 7–10 days and that for MAC at 10–14 days. When the actual TAT exceeds the benchmark, the laboratory can promptly investigate potential issues (e.g., sample quality, instrument status, or operational errors) to improve testing efficiency.
There are several limitations in this study, despite the meaningful findings. First, this was a retrospective study conducted in a single hospital, so the results might vary in other regions due to heterogeneity in species composition. Second, the sample size of RGM is significantly smaller than that of SGM, which constitutes an inherent limitation of the present research. Third, TAT in this study does not include species identification because species identification is not routinely performed in our clinical laboratory. In the future, the collection of RGM strains from multicenter collaboration will further verify the generalizability and robustness of our conclusions.
In summary, the TAT of NTM varies significantly by species. Patients with NTM-PD, bronchiectasis, or lung cavitation exhibit shorter TATs. Additionally, the AFB smear result was identified as the only independent factor significantly associated with TAT in the generalized linear model. These findings can be helpful in optimizing the laboratory detection workflow of mycobacteria and reasonably predicting the detection cycle. They may also provide support for clinical decision-making among physicians.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Porvaznik I SolovičI MokrýJ. Non-tuberculous mycobacteria: classification, diagnostics, and therapy. Adv Exp Med Biol. (2017) 944:19–25. doi: 10.1007/5584_2016_4527826888 · doi ↗ · pubmed ↗
- 2Ruan J. Bergey's manual of systematic bacteriology (second edition) volume 5 and the study of actinomycetes systematic in China. Wei Sheng Wu Xue Bao. (2013) 53:521–30.24028053 · pubmed ↗
- 3Fedrizzi T Meehan CJ Grottola A Giacobazzi E Fregni SG Tagliazucchi S . Genomic characterization of nontuberculous mycobacteria. Sci Rep. (2017) 7:45258. doi: 10.1038/srep 4525828345639 PMC 5366915 · doi ↗ · pubmed ↗
- 4Kumar K Ponnuswamy A Capstick TG Chen C Mc Cabe D Hurst R . Non-tuberculous mycobacterial pulmonary disease (NTM-PD): epidemiology, diagnosis and multidisciplinary management. Clin Med. (2024) 24:100017. doi: 10.1016/j.clinme.2024.100017, 38387207 PMC 11024839 · doi ↗ · pubmed ↗
- 5Jarchow-Mac Donald A Smith M Seagar AL Russell CD Claxton P Laurenson IF . Changing incidence and characteristics of nontuberculous mycobacterial infections in Scotland and comparison with Mycobacterium tuberculosis complex incidence (2011 to 2019). Open Forum Infect Dis. (2023) 10:c 665. doi: 10.1093/ofid/ofac 665, 36726549 PMC 9879710 · doi ↗ · pubmed ↗
- 6Goswami B Singh B Chawla R Gupta VK Mallika V. Turn around time (TAT) as a benchmark of laboratory performance. Indian J Clin Biochem. (2010) 25:376–9. doi: 10.1007/s 12291-010-0056-4, 21966108 PMC 2994570 · doi ↗ · pubmed ↗
- 7Färber J Kaasch AJ Schalk E. Shorter time-to-positivity and turnaround time with mycosis blood culture bottles when detecting Candida albicans. Infection. (2024) 52:701–3. doi: 10.1007/s 15010-024-02216-x, 38393640 PMC 10955001 · doi ↗ · pubmed ↗
- 8Lee S Yoon S Lee W Chun S Min WK. Strategies to shorten turnaround time in outpatient laboratory. J Clin Lab Anal. (2022) 36:e 24665. doi: 10.1002/jcla.24665, 36036784 PMC 9550964 · doi ↗ · pubmed ↗