Unique presentation of superficial siderosis of the central nervous system following pituitary tumor surgery: a case report and literature review
Tengyao Liang, Jiangqin Song, Fengzhu Zhao, Weifang Zhu, Hui Wei

TL;DR
A rare case of superficial siderosis of the central nervous system is reported in a patient after pituitary tumor surgery, highlighting diagnostic challenges and the need for awareness.
Contribution
This case report documents a rare and atypical presentation of SSCNS following pituitary tumor surgery.
Findings
The patient exhibited progressive neurological symptoms over two years, likely due to chronic subarachnoid hemorrhage.
Susceptibility-weighted imaging was crucial in identifying subtle iron deposition patterns characteristic of SSCNS.
The case emphasizes the need for interdisciplinary collaboration to improve diagnosis and management of SSCNS.
Abstract
Superficial Siderosis of the Central Nervous System is an infrequent neurological disorder resulting from hemosiderin deposition due to chronic and recurrent subarachnoid hemorrhage, leading to significant neurological impairments including sensorineural hearing loss, cerebellar ataxia, and pyramidal signs. This case report presents a 50-year-old male patient with a history of pituitary tumor surgery, manifesting progressive neurological symptoms over 2 years, thereby highlighting the potential long-term complications associated with SSCNS. The atypical clinical presentation, coupled with a surgical background, underscores the diagnostic challenges faced by clinicians, who may misattribute symptoms to more common neurological conditions. Advanced imaging modalities, particularly susceptibility-weighted imaging (SWI), have proven essential in enhancing the diagnostic accuracy for SSCNS,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
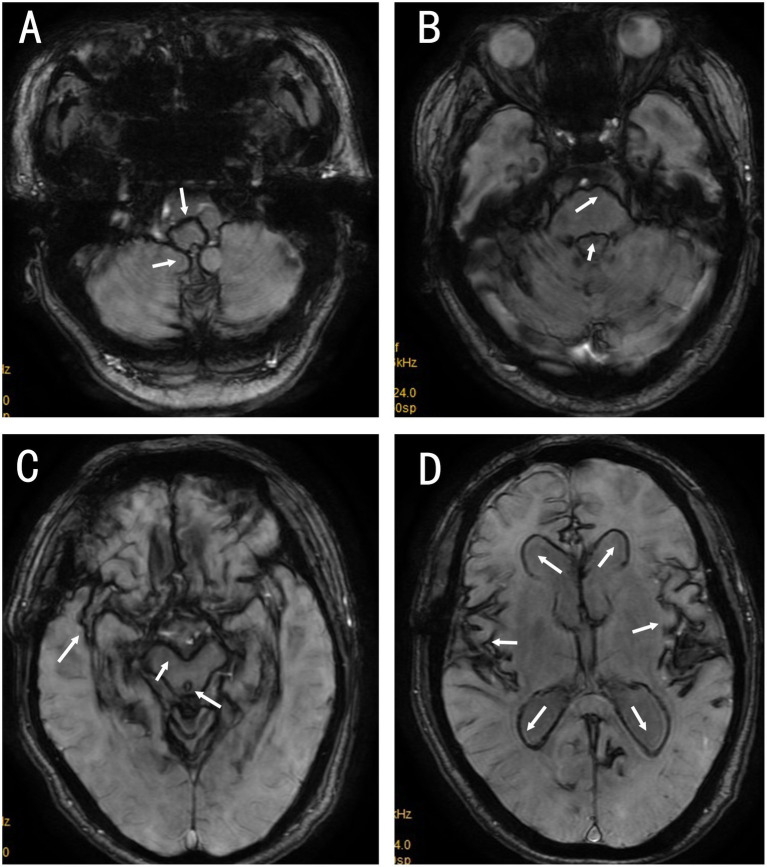 Figure 1
Figure 1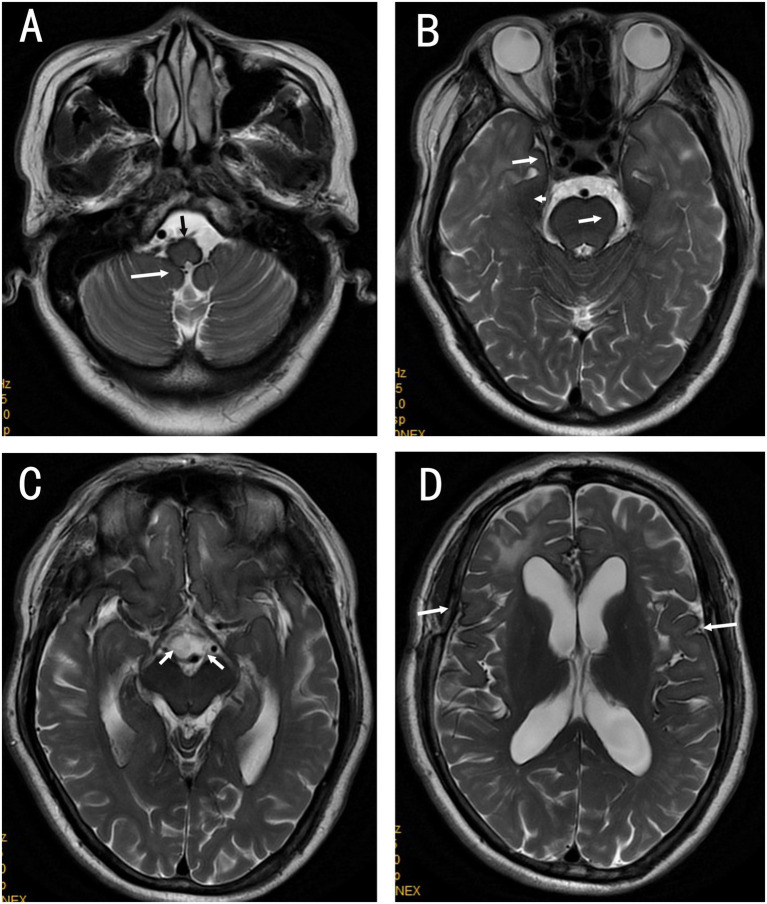 Figure 2
Figure 2| Reference | Year | Age/sex | Predisposing conditions | Presentation | Diagnosis | Etiology | Therapy/duration | Outcome |
|---|---|---|---|---|---|---|---|---|
|
| 2004 | 37/F | Remote transsphenoidal subtotal resection of a pituitary adenoma (19 years earlier) | Progressive bilateral sensorineural hearing loss; cerebellar ataxia | Superficial siderosis of the central nervous system (SS) | Long-term, surgery-related recurrent microbleeding in the sellar region causing chronic subarachnoid hemorrhage | No iron chelation; conservative follow-up (duration not specified) | Hearing loss and ataxia continued to progress |
|
| 2013 | 43/M | Giant invasive prolactinoma with pituitary apoplexy | Headache; visual dysfunction; progressive hearing loss | Apoplexy-associated SS | Hemorrhagic pituitary macroadenoma leading to chronic/recurrent subarachnoid hemorrhage | Not reported | Not reported |
|
| 2015 | 69/M | Papillary craniopharyngioma of the third ventricle | Headache; gait instability; blurred vision; progressive hearing loss | Papillary craniopharyngioma with SS | Intratumoral hemorrhage leaking into the CSF circulation, resulting in a chronic hemorrhagic burden | Microsurgical tumor resection | Further postoperative decline in hearing |
|
| 2018 | 50/M | Papillary craniopharyngioma of the third ventricle | Intermittent vertigo and headache | Papillary craniopharyngioma with SS | Preoperative intratumoral hemorrhage with subarachnoid dissemination | Tumor resection | Postoperative death |
|
| 2020 | 58/M | Suspected pituitary macroadenoma with hyperprolactinemia | Three months of headache; no hearing loss at initial visit | Pituitary macroadenoma–related CNS SS | Presumed recurrent microbleeding from the adenoma; no alternative bleeding source identified | Cabergoline; MRI surveillance every 6 months | Clinically stable; adenoma decreased in size; superficial siderosis persisted |
|
| 2022 | 75/M | Upper thoracic spinal dural defect (identified source of bleeding) | Progressive gait ataxia and hearing loss | SS due to dural defect | Dural tear causing chronic hemorrhagic CSF leakage | Surgical repair of the dural defect; symptoms stabilized postoperatively | No further progression after repair |
|
| 2023 | 70/M | Large nonfunctioning pituitary adenoma; SS present preoperatively | Headache; postoperative cerebral vasospasm and cerebral infarction | SS with postoperative vasospasm/infarction | Pituitary adenoma–related subarachnoid hemorrhage leading to SS; intraoperative hematoma entering the subarachnoid space may have increased hemorrhagic load | Endoscopic endonasal resection; CSF shunt for communicating hydrocephalus; antiepileptic therapy | Persistent impaired consciousness; poor functional recovery |
| Present case | 2020 | 50/M | Prior pituitary adenoma interventions: Gamma Knife in 2016 and craniotomy for tumor resection in June 2018; symptom onset after surgery | Two-year history of dizziness and unsteady gait without true vertigo; bilateral sensorineural hearing loss; memory decline (MMSE 22); positive Romberg; no focal deficits | Superficial siderosis of the central nervous system | Presumed chronic/recurrent subarachnoid hemorrhage related to prior pituitary surgery; bleeding source not identified | Therapies to improve cerebral circulation and neurotrophic support; slight symptomatic improvement; duration not specified | At 2-year follow-up: near-complete hearing loss and marked cognitive decline with loss of independent self-care |
| Dimension | SSCNS | CAA-related cortical superficial siderosis (cSS) | Acute/subacute subarachnoid hemorrhage (SAH) | Cavernous malformation/microbleeds | Calcification | Melanin-related leptomeningeal disease | Cortical vein thrombosis |
|---|---|---|---|---|---|---|---|
| Typical location | Cerebellar folia, brainstem, CPA cisterns; may involve cranial nerves and spinal leptomeninges; infratentorial predominance, often symmetric. | Cortical convexities, occipito-parietal tendency; infratentorial uncommon; often coexists with lobar CMBs. | Basal cisterns or regional sulci by source; migrates with time. | Intraparenchymal clustered lesions; often adjacent to DVA. | Deep nuclei, choroid plexus, pineal region patterns. | Diffuse or patchy leptomeningeal involvement; pan-neuroaxis possible. | Along cortical venous trajectories. |
| T2*/SWI morphology | Continuous linear/laminar hypointensity hugging the surface; best seen with 3D-SWI/GRE; cranial nerves or spinal dura may be involved. | Convexity-limited linear or patchy hypointensity; SWI more sensitive than GRE-T2* for disseminated cSS. | Transient, discontinuous low signal that fades over time. | Round/ovoid blooming foci with a “popcorn” core; thin hemosiderin rim. | Marked low signal but typically non-leptomeningeal; confirm with phase or CT. | Low signal may be present but is nonspecific; prioritize T1 and enhancement. | Linear hypointensity along one or more cortical veins; intraluminal thrombus blooming; SWI highly sensitive. |
| Other sequences/contrast | None or mild enhancement; non-specific T1. Recommend brain + whole-spine SWI/3D-FLAIR/spine MRI; selective CT-myelography or DSM to localise a dural tear when suspected. | Distribution confined to convexities; often with white-matter markers (e.g., CSO-PVS, WMH-MS). Use SWI when available. | CT: acute hyperdensity; FLAIR sulcal hyperintensity; clear temporal evolution per guidelines. | Mixed T1/T2 core; possible thin rim enhancement. | CT first-line; d-SWI/p-SWI and phase images improve discrimination between calcium and blood products. | Unenhanced T1 hyperintensity plus diffuse leptomeningeal enhancement; FLAIR hyperintensity possible. | Confirm filling defect on MRV/CTV; venous infarct/hemorrhage may coexist. |
| Clinical context | Progressive sensorineural hearing loss and ataxia; chronic low-grade bleeding from spinal dural defect is common. | Older adults; TFNE; CAA background. | Thunderclap headache, meningeal signs; acute onset. | Seizures or focal deficits; familial forms exist. | Often incidental; non-specific symptoms | Associated melanocytic tumors or neurocutaneous syndromes. | Headache with focal deficits; prothrombotic states, infection, pregnancy/postpartum. |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntracerebral and Subarachnoid Hemorrhage Research · Neurological and metabolic disorders · Cerebrospinal fluid and hydrocephalus
Introduction
Superficial siderosis of the central nervous system (SSCNS) is an uncommon neurological disorder caused by chronic or recurrent bleeding into the subarachnoid space, leading to persistent exposure of the leptomeninges and subpial tissues to hemoglobin breakdown products and subsequent hemosiderin deposition on the surface of the brain, cranial nerves, and spinal cord (Lobo et al., 2022). Clinically, SSCNS is a progressive and potentially disabling condition that can markedly compromise quality of life and functional independence (Kharytaniuk et al., 2022). Although initially described by Hamill in 1908, systematic clinicopathological characterization and recognition of its typical clinical course and etiologic spectrum were established in the seminal work by Fearnley, Stephens, and Rudge (Katoh and Watanabe, 2023; Fearnley et al., 1995). More recently, a mechanistic framework has been refined, emphasizing iron-mediated neurotoxicity (including oxidative injury and secondary neuronal/glial damage) driven by ongoing or intermittent subarachnoid hemorrhage, thereby explaining the insidious progression and the importance of identifying and eliminating the bleeding source (Wilson et al., 2017).
The classical clinical phenotype predominantly comprises progressive sensorineural hearing loss, cerebellar ataxia, and pyramidal tract signs (often with additional myelopathic features) (Fearnley et al., 1995), which may mimic more common neurodegenerative or cerebrovascular disorders and contribute to underrecognition. Magnetic resonance imaging (MRI), particularly blood-sensitive sequences (e.g., T2*-weighted GRE or SWI), is central to diagnosis by demonstrating a characteristic hypointense rim along the pial surfaces and/or cranial nerves consistent with hemosiderin deposition; however, subtle or overlooked imaging findings can delay diagnosis (Wilson et al., 2017). Importantly, contemporary management paradigms increasingly stress a “source-directed” strategy—actively searching for persistent bleeding sources such as dural defects and considering definitive repair when feasible—given emerging evidence that targeted dural repair may reduce ongoing subarachnoid bleeding and potentially alter disease trajectory.
The case of a 50-year-old male patient with a history of pituitary tumor surgery presents a unique instance of SSCNS, underscoring the importance of considering this diagnosis in patients exhibiting chronic neurological symptoms following subarachnoid hemorrhage. The progressive nature of this patient’s condition over two years emphasizes the potential long-term complications associated with SSCNS, including irreversible neurological damage. This case not only contributes to the existing literature by highlighting a rare presentation of SSCNS in a patient with a specific surgical background but also reinforces the necessity for heightened awareness among clinicians regarding the condition’s atypical presentations and the implications for treatment and management strategies (McMahon et al., 2022).
Case report
A 50-year-old man was admitted to the neurology department of our hospital in August 2020 with a 2-year history of dizziness and progressive unsteadiness while walking. He reported that the symptoms began after treatment for a pituitary adenoma and were accompanied by bilateral hearing decline and gradual cognitive complaints, predominantly affecting recent memory. He denied true spinning vertigo, nausea, vomiting, diplopia, dysphagia, choking on liquids, limb weakness, aphasia, seizures, or other focal neurological symptoms. He had sought medical attention at multiple institutions without meaningful improvement (details of prior medications were unavailable) and was therefore referred to our hospital for further evaluation. His medical history was notable for a pituitary adenoma diagnosed in 2016, treated with Gamma Knife radiosurgery, followed by craniotomy with tumor resection in June 2018. No interval MRI surveillance was obtained between 2016 and 2018 (between Gamma Knife treatment and craniotomy), mainly because of suboptimal follow-up compliance. He denied a history of hypertension, diabetes mellitus, stroke, coronary artery disease, head trauma, or toxic/drug exposures. There was no relevant family history and no known drug allergies.
Upon physical examination, the patient’s blood pressure was recorded at 124/82 mmHg, and no significant abnormalities were noted in the general medical examination. He was fully conscious and cooperative, though there was mild cognitive impairment indicated by a Mini-Mental State Examination (MMSE) score of 22. His speech was fluent, and both pupils were equal and reactive to light, measuring 2.5 mm. Ocular movements were normal, with no nystagmus observed. The nasolabial folds were symmetrical, tongue protrusion was midline, and bilateral hearing loss was evident. Muscle strength and tone in the limbs were normal, as were deep tendon reflexes. The finger-to-nose test was normal, but a positive Romberg test was noted. Both superficial and deep sensory functions were intact, and there were no pathological reflexes or signs of meningeal irritation. Bedside assessment revealed no spontaneous or gaze-evoked nystagmus. Orthostatic vital signs (supine-to-standing blood pressure measurement) did not meet criteria for orthostatic hypotension, and a supine roll test was negative for positional vertigo. Formal vestibular function testing (e.g., vHIT/HIMP or caloric testing) was not performed.
Laboratory tests revealed normal ranges for complete blood count, liver and kidney function, myocardial enzyme profile, coagulation function, D-dimer, homocysteine, and lipid profile. Tests for hepatitis B, hepatitis C, syphilis, and HIV were negative. Thyroid function tests indicated elevated thyroid-stimulating hormone (TSH) at 4.470 mIU/L (reference 0.4–4.0 mIU/L) and decreased free thyroxine (fT4) at 11.92 pmol/L (reference 12–22 pmol/L). Blood glucose indices showed an elevated hemoglobin A1c of 6.90% (diabetes diagnostic threshold ≥6.5%) and fasting plasma glucose of 6.33 mmol/L (ADA reference: normal <5.6 mmol/L, prediabetes 5.6–6.9 mmol/L, diabetes ≥7.0 mmol/L; WHO reference: normal <6.1 mmol/L, impaired fasting glucose 6.1–6.9 mmol/L, diabetes ≥7.0 mmol/L). Audiometry (Aug 4, 2020) showed bilateral high-frequency sloping sensorineural hearing loss. The pure-tone average (PTA; 0.5/1/2 kHz) was 36 dB HL in the right ear and 43 dB HL in the left ear (air conduction), with corresponding bone-conduction PTAs of 31 dB HL (right) and 38 dB HL (left). The air–bone gap was <10 dB HL bilaterally, supporting a sensorineural pattern. Based on PTA, hearing impairment was mild on the right and moderate on the left, with marked deterioration at higher frequencies (approximately 2–8 kHz) where thresholds reached the moderately severe to severe range. At the 2-year follow-up, the patient reported near-complete loss of functional hearing bilaterally, with inability to communicate by spoken voice. A cranial MRI scan revealed hypointensity in brain tissue on T2-weighted imaging, linear low signal on the brain surface, ventricular enlargement, white matter lesions, and brain atrophy (see Figures 1A–D). A neck and head computed tomography angiography (CTA) showed no evidence of vascular narrowing, malformations, or aneurysms. Suspected iron deposition was noted on susceptibility-weighted imaging (SWI), showing diffuse low signals on the surface of the pia mater, spinal meninges, and ventricular surfaces. Based on the SWI findings, a diagnosis of SSCNS was established (see Figures 2A–D).
Non-contrast MRI (A–D). T2-weighted imaging (T2WI) shows linear hypointensity along the pial and periventricular surfaces, predominantly infratentorial. (A) Linear hypointensity around the medulla oblongata (black arrow) and over the cerebellar surface (white arrow(s)). (B) Linear hypointensity around the pons and along the medial temporal lobe (white arrow(s)), with bilateral temporal lobe white-matter hyperintensities. (C) Linear hypointensity around the midbrain (white arrow(s)). (D) Linear hypointensity around the Sylvian fissure (white arrow(s)), with enlargement of the lateral ventricles and cerebral atrophy.
SWI (A–D) shows iron deposition along the cortical and periventricular surfaces. (A) Linear hypointensity around the medulla oblongata and over the cerebellar surface (white arrow(s)). (B) Linear hypointensity around the pons and the fourth ventricle (white arrow(s)). (C) Linear hypointensity along the temporal lobe surface, around the midbrain, and within the cerebral aqueduct (white arrow(s)). (D) Linear hypointensity around the lateral ventricles and the Sylvian fissures (white arrow(s)).
The patient was treated with therapies aimed at improving cerebral circulation and nourishing the nervous system, which resulted in slight symptomatic improvement. But 2 years later, follow-up assessments indicated that the patient had experienced almost complete loss of hearing and significant cognitive decline, rendering him unable to care for himself.
Discussion
In our patient, the florid infratentorial pattern of superficial siderosis on blood-sensitive MRI strongly supports a chronic or recurrent subarachnoid bleeding process rather than an isolated hemorrhagic event, consistent with established clinicopathological descriptions of SSCNS (Fearnley et al., 1995). From a mechanistic and practical perspective, current frameworks stress that ongoing iron-mediated injury drives clinical progression, making a source-directed workup essential to identify and eliminate the bleeding source whenever feasible (Wilson et al., 2017). This consideration is particularly relevant in the postoperative setting, where dural defects or occult spinal cerebrospinal fluid (CSF) leaks may serve as persistent bleeding foci; emerging evidence suggests that targeted detection and dural repair can reduce ongoing subarachnoid bleeding and may modify the disease trajectory (Lobo et al., 2022). Accordingly, beyond describing a rare association with a pituitary tumor history, this case underscores the need for systematic evaluation for a treatable bleeding source to potentially prevent further neurological decline.
A focused literature review was conducted in PubMed and regional sources using the keywords “superficial siderosis,” “pituitary adenoma,” “craniopharyngioma,” “dural defect,” “postoperative,” and “apoplexy,” restricting to human reports relevant to sellar or postoperative etiologies (Table 1). Cases due to non-surgical vascular lesions (aneurysm, arteriovenous malformation), major trauma, or systemic coagulopathies were excluded. Eight eligible cases were synthesized, including the present case (1998–2023). The cohort had a mean age of 56.5 years and was predominantly male. Two mechanisms predominated: tumor-associated hemorrhage (5/8; pituitary adenoma or craniopharyngioma) and postoperative dural defect/leak permitting chronic low-grade bleeding (3/8; one spinal dural tear and two postoperative sellar contexts). Progressive sensorineural hearing loss and gait ataxia were the leading manifestations; T2*-weighted GRE or SWI consistently revealed superficial siderosis along cerebellar and cortical surfaces. Management clustered into definitive tumor hemostasis/resection, targeted dural repair or CSF pathway reconstruction, and adjunct medical therapy (e.g., dopamine agonists for prolactinoma), with outcomes markedly better when the bleeding source was identified and controlled; in contrast, non-definitive care was associated with progression, including one postoperative death and persistent disability.
Our patient fits a postoperative pathway: prior pituitary adenoma treatment (Gamma Knife radiosurgery in 2016 followed by craniotomy and tumor resection in 2018), craniospinal SWI evidence of diffuse siderosis, negative vascular imaging, and a chronic, low-grade course culminating in near-total functional deafness and cognitive decline. In this context, prior Gamma Knife radiosurgery and subsequent open surgery could be considered potential contributing background factors, as postoperative changes at the sellar region (including tissue remodeling and dural scarring) may, in principle, facilitate occult CSF-space bleeding or dural vulnerability, although a direct causal relationship cannot be established from the available data. Furthermore, the absence of interval MRI surveillance between 2016 and 2018 (mainly due to suboptimal follow-up compliance) may have limited early detection of progressive hemosiderin deposition and delayed etiologic evaluation. Taken together, these features are compatible with an occult dural or tumor-bed source that was not definitively localized or repaired. For similar cases, a source-first strategy is indicated—craniospinal SWI with targeted (dynamic) CT myelography/cisternography to localize small dural defects or CSF leaks, followed by watertight dural repair—before considering hearing rehabilitation.
In contrast to other studies, our case highlights a unique presentation following pituitary tumor Surgery, demonstrating the role of primary CNS tumors as potential bleeding sources—an aspect less frequently documented in the literature.
Imaging techniques, particularly susceptibility-weighted imaging (SWI), have revolutionized the diagnostic approach, allowing for more accurate identification of iron deposition patterns in SSCNS. While the existing literature outlines symptoms common to SSCNS patients, the variability in clinical presentation underscores the need for heightened awareness among clinicians. This case not only contributes to the understanding of SSCNS but also emphasizes the criticality of etiological exploration for effective management and highlights a significant gap in current literature regarding the long-term outcomes and treatment efficacy in similar cases. To frame the differential diagnosis, Table 2 summarizes MRI discriminators by distribution, T2/SWI morphology, ancillary sequences, and clinical context.
The diagnosis of SSCNS presents significant challenges, primarily due to its rarity and the nonspecific nature of its clinical manifestations. The presence of progressive neurological symptoms following a history of subarachnoid hemorrhage should prompt clinicians to consider SSCNS in their differential diagnosis. Misdiagnosis remains a notable concern, as common symptoms such as ataxia and hearing loss can often be attributed to other neurological disorders, leading to delays in appropriate management. The utilization of advanced imaging modalities, particularly susceptibility-weighted imaging (SWI), has proven essential in identifying the characteristic iron deposits associated with SSCNS, thereby facilitating earlier and more accurate diagnoses. This case underscores the necessity for an interdisciplinary approach, involving collaboration among neurologists and radiologists, to enhance recognition and treatment strategies for SSCNS (Liao and Deng, 2024).
Moreover, understanding the underlying pathophysiological mechanisms of SSCNS is crucial for developing effective therapeutic interventions. Chronic exposure to blood breakdown products in the subarachnoid space, particularly following recurrent hemorrhages, leads to hemosiderin deposition, which is implicated in oxidative stress and neurodegeneration (Raveendran and Rajini, 2024). As evidenced by this case, the association between SSCNS and prior surgical interventions, such as the resection of tumors, highlights a previously underappreciated etiological factor that warrants further investigation. Future research should aim to elucidate the long-term outcomes and efficacy of treatment approaches targeting the oxidative pathways involved in SSCNS, as existing management remains largely symptomatic (Mariajoseph et al., 2023).
The unique presentation following pituitary tumor surgery exemplifies the complexities associated with identifying SSCNS, particularly in patients with prior neurological interventions. Clinicians must maintain a high index of suspicion for SSCNS when faced with progressive neurological deficits, especially in the context of subarachnoid hemorrhage. The utilization of advanced imaging techniques, such as susceptibility-weighted imaging (SWI), is paramount in enhancing diagnostic accuracy and expediting appropriate management. Furthermore, the interdisciplinary collaboration among neurologists and radiologists is essential for improving recognition and treatment strategies for SSCNS, ultimately leading to better patient outcomes.
Conclusion
SSCNS results from hemosiderin deposition and iron-mediated neurotoxicity secondary to chronic or intermittent subarachnoid hemorrhage. The typical phenotype comprises progressive cerebellar ataxia, sensorineural hearing loss, and pyramidal signs; in at-risk populations, SSCNS should be prioritized in the differential diagnosis and evaluated promptly. Susceptibility-weighted imaging (SWI) is highly sensitive for superficial iron deposition and should serve as the first-line modality, complemented by whole-brain and whole-spine imaging with systematic assessment of dural integrity to localize low-grade, intermittent bleeding sources, including postoperative dural defects, tumor-related leakage, and vascular malformations. Management centers on etiologic control: early identification and definitive repair or resection of the bleeding source can attenuate disease progression and improve functional outcomes, whereas pharmacologic approaches—including iron chelation—have limited evidentiary support and are unlikely to reverse established neurodegeneration. Multidisciplinary care and structured long-term follow-up are recommended to enable early recognition, timely intervention, and optimization of long-term prognosis.
In summary, the rarity of SSCNS, coupled with its complex clinical presentation and diagnostic challenges, necessitates a thorough understanding and consideration in clinical practice. Documenting such cases is vital for enhancing awareness and improving diagnostic accuracy, ultimately leading to better patient outcomes and informing future research efforts to elucidate the underlying mechanisms and potential therapeutic approaches for this debilitating condition.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Fearnley J. M. Stevens J. M. Rudge P. (1995). Review article: superficial siderosis of the central nervous system. Brain 118, 1051–1066. doi: 10.1093/brain/118.4.1051, 7655881 · doi ↗ · pubmed ↗
- 2Hashikata H. Takebe N. Yoshizaki W. Maki Y. (2023). Postoperative vasospasm and cerebral infarction in a patient with large pituitary adenoma and cerebral superficial siderosis. Surg. Neurol. Int. 14:256. doi: 10.25259/sni_397_2023, 37560577 PMC 10408626 · doi ↗ · pubmed ↗
- 3Katoh H. Watanabe M. (2023). “Superficial Siderosis” in Essentials of Cerebellum and Cerebellar Disorders: A Primer for Graduate Students. eds. Gruol D. L. Koibuchi N. Manto M. Molinari M. Schmahmann J. D. Shen Y. (Cham (Switzerland): Springer International Publishing).
- 4Kharytaniuk N. Cowley P. Sayal P. Eleftheriou P. Farmer S. F. Chan E. . (2022). Classical infratentorial superficial siderosis of the central nervous system: pathophysiology, clinical features and management. Pract. Neurol. 22, 274–284. doi: 10.1136/practneurol-2021-003324, 35817559 PMC 7614629 · doi ↗ · pubmed ↗
- 5Liao H. Deng Y. (2024). Cerebral superficial siderosis. Neurol. India 72, 205–206. doi: 10.4103/neurol-india.Neurol-India-D-24-00018, 38443043 · doi ↗ · pubmed ↗
- 6Lobo R. Batbayar B. Kharytaniuk N. Cowley P. Sayal P. Farmer S. . (2022). Targeted detection and repair of a spinal dural defect associated with successful biochemical resolution of subarachnoid bleeding in classical infratentorial superficial siderosis. Neurol. Sci. 43, 5643–5646. doi: 10.1007/s 10072-022-06181-x, 35691973 PMC 9385782 · doi ↗ · pubmed ↗
- 7Mapaga J. N. Martinez M. (2020). Hemosiderosis of the central nervous system and its association with a pituitary macroadenoma: a case report. Pan Afr. Med. J. 37:288. doi: 10.11604/pamj.2020.37.288.17507, 33623627 PMC 7881924 · doi ↗ · pubmed ↗
- 8Mariajoseph F. P. Castle-Kirszbaum M. Chandra R. V. Lai L. T. Gonzalvo A. Williamson T. . (2023). Safety and effectiveness of spinal dural defect repair in the management of superficial siderosis: a systematic review and patient-level analysis. J. Clin. Neurosci. 109, 44–49. doi: 10.1016/j.jocn.2023.01.011, 36731382 · doi ↗ · pubmed ↗