Postoperative Adjuvant Therapy in Resectable Advanced Oral Squamous Cell Carcinoma With Intermediate Risk Factors
Koichi Koizumi, Fumitaka Obayashi, Mirai Higaki, Kota Morishita, Atsuko Hamada, Sachiko Yamasaki, Nanako Ito, Souichi Yanamoto

TL;DR
This study examines how post-surgery treatments affect survival in oral cancer patients with certain risk factors, finding that specific tumor features strongly influence outcomes.
Contribution
Identifies perineural and lymphatic invasion as critical factors for determining postoperative adjuvant therapy in intermediate-risk oral cancer patients.
Findings
Perineural invasion significantly increases recurrence and metastasis rates in oral cancer patients.
Lymphatic invasion is associated with poorer survival outcomes in patients with advanced oral cancer.
Postoperative adjuvant therapy improves survival for patients with perineural or lymphatic invasion.
Abstract
Postoperative adjuvant therapy strategies are generally determined based on pathological risk stratification in oral cancer. However, the efficacy of postoperative adjuvant therapy in patients with intermediate‐risk factors for recurrence of oral cancer such as close surgical margins, pT3–T4 classification, pN2–N3 nodal status, perineural invasion, vascular invasion, lymphatic invasion and pattern of invasion remains unclear, and no standardized treatment guidelines or consensus have been established to date. Therefore, this study retrospectively analyzed the clinical significance of risk factors for pathological recurrence in patients with advanced oral cancer and evaluated the impact of postoperative adjuvant therapy on patient prognosis. This retrospective clinical study included 130 patients who underwent initial radical surgical resection for advanced oral squamous cell carcinoma…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
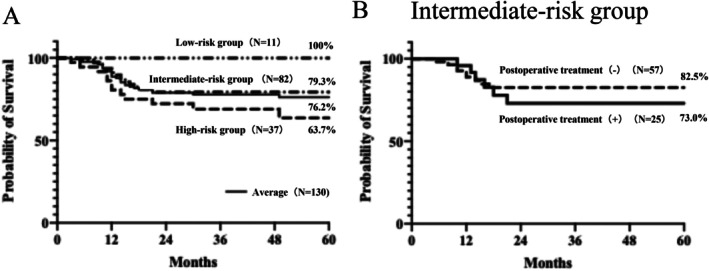 FIGURE 1
FIGURE 1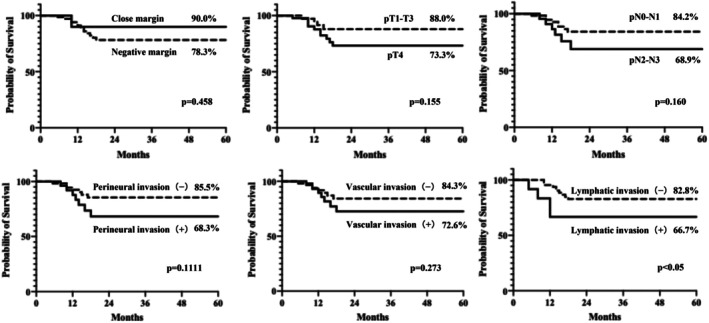 FIGURE 2
FIGURE 2| Characteristics | No. of cases (%) | ||
|---|---|---|---|
| Surgical margin | |||
| Positive | 17 | (13.1) | |
| Close | 11 | (8.4) | |
| Negative | 102 | (78.5) | |
| Perineural invasion | |||
| Positive | 46 | (35.4) | |
| Negative | 84 | (64.6) | |
| Vascular invasion | |||
| Positive | 33 | (25.4) | |
| Negative | 97 | (74.6) | |
| Lymphatic invasion | |||
| Positive | 20 | (15.4) | |
| Negative | 110 | (84.6) | |
| Preoperative treatment | |||
| Yes | 32 | (24.6) | |
| No | 98 | (75.4) | |
| Postoperative treatment | |||
| Yes | 58 | (44.6) | |
| No | 72 | (55.4) | |
| Follow‐up observation | Re‐resection | Re‐resection + CRT (or RT) | CRT (or RT) | Subtotal | Total | |
|---|---|---|---|---|---|---|
| High risk group | ||||||
| Extranodal extension ± positive margin | 1/5 | 0/1 | 10/19 | 11/25 | 18/37 (48.6%) | |
| Positive margin | 2/4 | 1/2 | 4/6 | 7/12 | ||
| Intermediate‐risk group | ||||||
| Close margin | 1/4 | 0/2 | 1/2 | 1/3 | 3/11 | 28/82 (34.1%) |
| pT3 or pT4 | 17/50 | 0/2 | 1/1 | 5/15 | 23/66 | |
| pN2 or pN3 | 7/9 | 4/15 | 11/24 | |||
| Perineural invasion | 9/18 | 0/1 | 1/2 | 4/6 | 14/27 | |
| Vascular invasion | 7/12 | 0/1 | 1/1 | 1/5 | 9/19 | |
| Lymphatic invasion | 7/11 | 0/1 | 7/12 | |||
| Low‐risk group | ||||||
| No risk factors | 3/11 | 3/11 (27.3%) | ||||
| 48/130 (36.9%) | ||||||
| HR | 95% Cl |
| |
|---|---|---|---|
| Close margin/Negative margin | 0.47 | 0.10–2.14 | 0.458 |
| pT3‐T4/pT1‐T2 | 0.86 | 0.23–3.27 | 0.817 |
| pT4/pT1‐T3 | 2.25 | 0.79–6.44 | 0.155 |
| pN2‐N3/pN0‐N1 | 2.09 | 0.64–6.85 | 0.160 |
| Perineural invasion (+)/(−) | 2.28 | 0.73–7.10 | 0.111 |
| Vascular invasion (+)/(−) | 1.78 | 0.60–5.29 | 0.273 |
| Lymphatic invasion (+)/(−) | 3.08 | 0.60–15.91 | < 0.05 |
| Recurrence/Metastasis | HR | 95% Cl |
| |||
|---|---|---|---|---|---|---|
| (+) | (−) | |||||
| Close margin | ||||||
| (+) | 3 | 8 | 0.719 | 0.128–3.246 | 0.678 | |
| (−) | 24 | 47 | ||||
| pT4 | ||||||
| (+) | 17 | 27 | 1.763 | 0.695–4.655 | 0.234 | |
| (−) | 10 | 28 | ||||
| pN2‐N3 | ||||||
| (+) | 10 | 14 | 2.937 | 0.812–11.296 | 0.101 | |
| (−) | 17 | 41 | ||||
| Perineural invasion | ||||||
| (+) | 14 | 13 | 4.496 | 1.276–17.786 | 0.019 | |
| (−) | 13 | 42 | ||||
| Vascular invasion | ||||||
| (+) | 9 | 10 | 0.665 | 0.148–2.643 | 0.571 | |
| (−) | 18 | 45 | ||||
| Lymphatic invasion | ||||||
| (+) | 7 | 5 | 3.139 | 0.749–14.064 | 0.117 | |
| (−) | 20 | 50 | ||||
| Postoperative treatment | Recurrence/Metastasis | |||||
|---|---|---|---|---|---|---|
| (+) | (−) | HR | 95% Cl |
| ||
| Close margin (11) | ||||||
| (+) | 2 | 5 | 1.200 | 0.076–32.783 | 0.898 | |
| (−) | 1 | 3 | ||||
| pT4 (44) | ||||||
| (+) | 5 | 5 | 1.833 | 0.431–7.882 | 0.431 | |
| (−) | 12 | 22 | ||||
| pN2‐N3 (24) | ||||||
| (+) | 4 | 11 | 0.181 | 0.026–1.021 | 0.053 | |
| (−) | 6 | 3 | ||||
| Perineural invasion (27) | ||||||
| (+) | 5 | 4 | 1.250 | 0.249–6.574 | 0.785 | |
| (−) | 9 | 9 | ||||
| Vascular invasion (19) | ||||||
| (+) | 2 | 5 | 0.286 | 0.031–1.942 | 0.204 | |
| (−) | 7 | 5 | ||||
| Lymphatic invasion (12) | ||||||
| (+) | 0 | 3 | 0.009 | |||
| (−) | 7 | 2 | ||||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHead and Neck Cancer Studies · Oral Health Pathology and Treatment · Oral and Maxillofacial Pathology
Introduction
1
Oral cancer is characterized by its significant local invasiveness and a high postoperative recurrence rate. Postoperative adjuvant therapy (radiotherapy (RT) and/or chemoradiotherapy (CRT)) aimed at preventing recurrence after curative resection plays a critical role in improving patient prognosis [1, 2]. Surgical resection remains the cornerstone of treatment for resectable advanced oral cancers classified as stage III or IV unless contraindicated by the patient's general condition or personal preferences. Following surgery, the intraoperative and postoperative resected specimens are evaluated to assess the risk of recurrence, which in turn determines the indication for postoperative adjuvant therapy.
Local recurrence and distant metastasis are the most significant factors influencing treatment outcomes in oral cancer. Therefore, identifying predictive factors for these outcomes is essential for optimizing therapeutic strategies [3, 4, 5, 6, 7]. The 2024 edition of the NCCN guidelines classifies recurrence risk factors into high‐ and intermediate‐risk categories. High‐risk factors include extranodal extension (ENE) of the cervical lymph nodes and positive surgical margins (R1), whereas intermediate‐risk factors comprise close surgical margins, pT3–T4 classification, pN2–N3 nodal involvement, metastasis to level IV or V lymph nodes, perineural invasion, vascular invasion, and lymphatic invasion. Among these, perineural invasion is particularly notable for its close association with tumor aggressiveness and local recurrence risk and is recognized as a poor prognostic factor. Recent studies have reported that patients with perineural invasion‐positive tumors experience higher recurrence rates and reduced disease‐free survival (DFS) and overall survival (OS) [8, 9, 10, 11, 12, 13]. However, the efficacy of postoperative adjuvant therapy in patients with perineural invasion‐positive oral cancer remains unclear, and no standardized treatment guidelines or consensus have been established to date.
Therefore, this study aimed to retrospectively analyze the clinical significance of risk factors for pathological recurrence in patients with advanced oral cancer, focusing on the presence or absence of perineural invasion. Specifically, we evaluated the impact of postoperative adjuvant therapy (RT and CRT) on patient prognosis. In doing so, we hope to contribute to the optimization of postoperative treatment strategies based on recurrence risk and provide new insights into the management of patients with perineural invasion‐positive oral cancer.
Materials and Methods
2
This retrospective clinical study included 130 patients who underwent initial radical surgical resection for advanced oral squamous cell carcinoma (OSCC) at our institution between January 2010 and December 2023. Advanced cases were defined as those classified as stage III or IV, according to the 8th edition of the Union for International Cancer Control Staging System. The primary tumor sites of the 130 cases were as follows: mandibular gingiva, tongue, maxillary gingiva, floor of the mouth, and buccal mucosa in 52 (40%), 33 (25%), 23 (18%), 13 (10%), and 9 (7%), respectively (Table 1A). Detailed clinicopathological characteristics of the patients are presented in Table 1B.
The postoperative recurrence risk factors included ENE of the cervical lymph nodes, positive surgical margins, close surgical margins, pathological T classification (pT3 or pT4), pathological N classification (pN2 or pN3), metastasis to level IV or V lymph nodes, perineural invasion, vascular invasion, and lymphatic invasion. We analyzed the relationships among the presence of these risk factors, administration of postoperative adjuvant therapy (RT or CRT), occurrence of recurrence or metastasis, and patient prognosis (DFS). The decision to initiate postoperative adjuvant therapy was based on the final pathological findings and discussion with a multidisciplinary tumor board. All enrolled patients received either RT alone or CRT, mainly with cisplatin. Recurrence or metastasis and final survival status were determined by reviewing the medical records. The primary endpoint was DFS.
Ethics Statement
2.1
This study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the Ethics Committee of Hiroshima University (approval number: e2023‐0056).
Statistical Analysis
2.2
Survival curves were generated using the Kaplan–Meier method, and between‐group differences were assessed using the log‐rank test. Multivariate analysis was performed using the Cox proportional hazards model to identify factors affecting DFS. Associations between the risk factors for recurrence, the presence or absence of postoperative adjuvant therapy, and the rates of recurrence or metastasis were evaluated using logistic regression analysis. Statistical significance was set at p < 0.05. All statistical analyses were conducted using JMP Pro version 16 (SAS Institute).
Results
3
The rates of local recurrence, cervical lymph node metastasis, and distant metastasis were 16.2%, 15.4%, and 9.2%, respectively, with an overall recurrence/metastasis rate of 36.9%. When analyzed according to the risk factors for recurrence, the high‐risk group, defined by the presence of ENE of the cervical lymph nodes and/or positive surgical margins, showed a recurrence/metastasis rate of 48.6%. The intermediate‐risk group, which included patients with close surgical margins, pT3–T4, pN2–N3 metastasis to level IV or V lymph nodes, perineural invasion, vascular invasion, or lymphatic invasion, had a recurrence/metastasis rate of 34.1%. However, the low‐risk group, with none of these pathological risk factors, had a recurrence/metastasis rate of 27.3% (Table 2).
Analysis of the association between the risk factors for recurrence and 5‐year OS showed that the high‐, intermediate‐, and low‐risk groups had a 5‐year OS rate of 63.7%, 79.3%, and 100%, respectively, with an overall average of 76.2% (Figure 1A). No significant difference in the 5‐year OS was observed between patients in the intermediate‐risk group who received postoperative therapy and those who did not (Figure 1B). When the 5‐year OS was compared according to individual intermediate risk factors, patients with lymphatic invasion had a significantly lower survival rate than those without lymphatic invasion (66.7% vs. 82.8%, p < 0.05). Multivariate analysis using the Cox proportional hazards model also demonstrated that the presence of lymphatic invasion was an independent prognostic factor (Hazard ratio (HR) = 3.08, p = 0.043), confirming its clinical relevance. Although other intermediate‐risk factors did not reach statistical significance, a trend toward reduced survival was observed in each case: pT4 versus pT1–T3 (73.3% vs. 88.0%, p = 0.155), pN2–N3 versus pN0–N1 (68.9% vs. 84.2%, p = 0.160), perineural invasion‐positive versus perineural invasion‐negative (68.3% vs. 85.5%, p = 0.111), and vascular invasion‐positive versus vascular invasion‐negative (72.6% vs. 84.3%, p = 0.273) (Figure 2, Table 3).
5‐year OS by risk factor for recurrence (A), 5‐year OS by intermediate risk factors for recurrence with or without postoperative treatment (B).
5‐year OS in the presence or absence of intermediate risk factors for recurrence.
When the recurrence and metastasis rates were compared according to individual intermediate risk factors, the perineural invasion‐positive group had a significantly higher rate than the perineural invasion‐negative group (51.9% vs. 23.6%, p < 0.05). Multivariate analysis using logistic regression also confirmed that the presence of perineural invasion was an independent prognostic factor (HR = 4.496, p = 0.019) (Table 4). Among patients with two or more intermediate risk factors, a significant difference was observed only in cases involving perineural invasion (data not shown).
Logistic regression analysis was used to evaluate the relationship between postoperative adjuvant therapy and recurrence/metastasis in patients with intermediate‐risk factors. The results showed a significant association only in cases with lymphatic invasion (p = 0.009), suggesting a potential benefit of postoperative adjuvant therapy for these patients. No significant differences in recurrence or metastasis rates were observed with or without postoperative adjuvant therapy for the other intermediate‐risk factors (Table 5).
Discussion
4
Postoperative adjuvant therapy strategies are generally determined based on pathological risk stratification in oral cancer [1, 14]. The intermediate‐risk group comprises patients without high‐risk features—such as positive surgical margins or ENE of the cervical lymph nodes—who remain at risk of recurrence if treated with surgery alone. In such patients, the indication for postoperative adjuvant therapy (RT or CTR) is usually considered [15, 16, 17]. Pathological risk factors that classify a case into the intermediate‐risk category include close surgical margins, pT3–T4 classification, pN2–N3 nodal status, metastasis to level IV or V cervical lymph nodes, perineural invasion, vascular invasion, lymphatic invasion, depth of invasion (DOI) of the primary lesion, histological grade of tumor differentiation, and pattern of invasion. Determining whether adjuvant therapy should be administered to patients with these risk factors remains a significant clinical challenge, as clear and standardized criteria for such decisions have not yet been established.
Among the 37 patients with high‐risk recurrence factors, 32 (86.5%) received postoperative adjuvant therapy. Recurrence was observed in 18 (48.6%) of the patients. In contrast, within the intermediate‐risk group, defined by factors such as close surgical margins, pT3–T4 classification, pN2–N3 nodal involvement, perineural invasion, vascular invasion, and lymphatic invasion, recurrence or metastasis was observed in 28 of the 82 patients (34.1%). Notably, the recurrence rates were markedly high in patients who did not receive postoperative adjuvant therapy: 77.8% (7 of 9 cases), 50.0% (9 of 18 cases), 58.3% (7 of 12 cases), and 63.6% (7 of 11 cases) in the pN2–N3‐positive, perineural invasion‐positive, vascular invasion‐positive, and lymphatic invasion‐positive groups, respectively. These findings suggest that patients with pathological risk factors, such as pN2–N3 nodal status perineural invasion, vascular invasion, or lymphatic invasion, can benefit from a more proactive application of postoperative adjuvant therapy.
Several studies have reported differences in survival and recurrence rates based on whether postoperative adjuvant therapy was administered in patients classified as intermediate‐risk for recurrence [17, 18, 19, 20, 21]. For instance, in cases with a large DOI that resulted in disease upstaging, the OS was significantly lower in patients who did not receive postoperative RT, highlighting the importance of such therapy [22, 23, 24, 25]. Similarly, among patients with perineural invasion, those treated with surgery alone experience poorer local control and reduced DFS, whereas the addition of postoperative RT significantly improved DFS in some studies [11, 26, 27, 28]. In the present study, among patients with intermediate‐risk factors, those with lymphatic invasion showed a significantly lower 5‐year DFS than those without lymphatic invasion, suggesting the need for postoperative adjuvant therapy. Although not statistically significant, a trend toward decreased 5‐year DFS was observed in patients with pT4 tumors, pN2–N3 nodal involvement, perineural invasion positivity, or vascular invasion positivity, indicating that postoperative adjuvant therapy is also applicable in these subgroups. Conversely, the 5‐year DFS was improved in patients with close surgical margins despite the absence of postoperative adjuvant therapy, suggesting that this factor alone does not warrant such additional treatment. Multivariate analysis of factors associated with recurrence and metastasis in the intermediate‐risk group revealed that only patients with perineural invasion positivity had a significantly higher rate of recurrence and metastasis, demonstrating the presence of perineural invasion as an independent prognostic factor (HR = 4.496, p = 0.019). Among patients with multiple intermediate‐risk factors (i.e., having two or more of such factors), a significant difference in recurrence/metastasis was observed only in those who were perineural invasion positive (data not shown).
Analysis of the association between postoperative adjuvant therapy and recurrence/metastasis in patients with intermediate‐risk factors revealed a significant difference only in the lymphatic invasion‐positive group. These findings strongly support the recommendation to administer postoperative adjuvant therapy to patients with lymphatic invasion. RT alone or concurrent CRT is typically considered a postoperative adjuvant therapy option for patients in the intermediate‐risk groups. In patients with these pathological risk factors, postoperative RT is expected to reduce local recurrence rates and improve survival outcomes. Indeed, many retrospective studies have demonstrated a tendency for better survival outcomes in patients who received adjuvant RT compared to those who did not [17, 18, 19, 20, 21, 25]. However, the additive benefit of CRT in this risk group remains inconclusive, with different results reported across studies [2]. Therefore, the decision to administer postoperative adjuvant therapy and the specific type of treatment should be made on an individual basis, guided by the specific recurrence risk factors. Particularly, the introduction of postoperative adjuvant therapy should be strongly considered for patients with independent adverse prognostic indicators, such as lymphatic or perineural invasion. We fully acknowledge the limitation of our study's statistical power due to the relatively small sample size. In response, our findings should be interpreted with caution and that larger, multicenter, and prospective studies are warranted to validate our observations.
Each pathological risk factor classified in the intermediate‐risk group for recurrence also serves as a poor prognostic indicator, directly influencing recurrence rates and patient survival. Representative adverse prognostic factors include bone, perineural, and vascular invasion; multiple metastatic lymph nodes; close surgical margins; and poor tumor differentiation. Among them, bone invasion is a notable predictor of decreased OS [29], and perineural invasion positivity has been independently linked to poor local control and reduced DSS [26, 28]. Although the rate of distant metastasis is lower than that of local recurrence, it still has significant clinical relevance. Notably, patients with a large number of metastatic lymph nodes or extensive cervical lymph node involvement have a markedly increased risk of developing distant metastases [30, 31, 32, 33]. In the present study, 12 of the 48 patients with intermediate‐risk factors (25%) had distant metastases, and half of them had multiple lymph node metastases. These findings strongly suggest the importance and potential benefits of adjuvant therapy in patients with pN2–N3 nodal status. Therefore, evaluating recurrence and metastasis risk using a multifactorial approach, incorporating quantitative indicators, such as the extent and volume of lymph node metastasis, is essential to make informed and individualized decisions regarding the necessity and intensity of postoperative adjuvant therapy.
Based on the findings of the present study and previous reports, treatment strategies for advanced oral cancer can be summarized as follows. Surgical resection is the first‐line treatment in resectable cases. Re‐resection may be considered in some cases if postoperative pathological evaluation reveals high‐risk factors for recurrence, such as positive surgical margins or ENE of the cervical lymph nodes. However, as a general principle, postoperative CRT using RT in combination with high‐dose cisplatin is recommended. Selecting an appropriate postoperative adjuvant therapy based on specific risk factors is critical in cases with intermediate risk factors for recurrence. In particular, perineural invasion has been shown to be strongly correlated with local recurrence, and lymphatic invasion has been suggested to be associated with poorer prognoses. Therefore, postoperative RT (with the optional addition of cisplatin) should be administered in such cases. Postoperative RT should be actively considered for patients with pT4 tumors, pN2–N3 nodal involvement, or vascular invasion. Conversely, the recurrence rate is relatively low for patients who do not exhibit any of these risk factors, and the prognosis is generally favorable. In such cases, withholding postoperative adjuvant therapy and conducting careful clinical follow‐up is reasonable. Consequently, establishing personalized treatment strategies based on these risk factors is essential. Further prospective studies are necessary to optimize the treatment intensity and ensure that therapeutic interventions are tailored to each patient's profile.
In conclusion, this study demonstrated that perineural invasion is a significant risk factor for recurrence and that lymphatic invasion is a poor prognostic factor in oral cancer. Postoperative adjuvant therapy in patients with perineural or lymphatic invasion‐positive disease contributed to reduced recurrence rates and prolonged survival. These findings suggest that the pathological evaluation of perineural and lymphatic invasions is an important indicator in determining the appropriateness of postoperative adjuvant therapy. Ultimately, this study's findings could support the development of personalized treatment strategies and contribute to the optimization of therapeutic outcomes in oral cancer management.
Funding
The authors have nothing to report.
Ethics Statement
The authors have nothing to report.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1J. S. Cooper , T. F. Pajak , A. A. Forastiere , et al., “Postoperative Concurrent Radiotherapy and Chemotherapy for High‐Risk Squamous‐Cell Carcinoma of the Head and Neck,” New England Journal of Medicine 350 (2004): 1937–1944.15128893 10.1056/NEJ Moa 032646 · doi ↗ · pubmed ↗
- 2J. P. Pignon , A. le Maitre , E. Maillard , J. Bourhis , and MACH‐NC Collaborative Group , “Meta‐Analysis of Chemotherapy in Head and Neck Cancer (MACH‐NC): An Update on 93 Randomised Trials and 17,346 Patients,” Radiotherapy and Oncology 92 (2009): 4–14.19446902 10.1016/j.radonc.2009.04.014 · doi ↗ · pubmed ↗
- 3C. T. Liao , S. F. Huang , I. H. Chen , et al., “Risk Stratification of Patients With Oral Cavity Squamous Cell Carcinoma and Contralateral Neck Recurrence Following Radical Surgery,” Annals of Surgical Oncology 16 (2009): 159–170.19011944 10.1245/s 10434-008-0196-4 · doi ↗ · pubmed ↗
- 4S. Yanamoto , S. Yamada , H. Takahashi , et al., “Clinicopathological Risk Factors for Local Recurrence in Oral Squamous Cell Carcinoma,” International Journal of Oral and Maxillofacial Surgery 41 (2012): 1195–1200.22901502 10.1016/j.ijom.2012.07.011 · doi ↗ · pubmed ↗
- 5S. Yanamoto , S. Yamada , H. Takahashi , et al., “Predictors of Locoregional Recurrence in T 1‐2N 0 Tongue Cancer Patients,” Pathology Oncology Research 19 (2013): 795–803.23677778 10.1007/s 12253-013-9646-9 · doi ↗ · pubmed ↗
- 6S. B. Chinn and J. N. Myers , “Oral Cavity Carcinoma: Current Management, Controversies, and Future Directions,” Journal of Clinical Oncology 33 (2015): 3269–3276.26351335 10.1200/JCO.2015.61.2929 PMC 5320919 · doi ↗ · pubmed ↗
- 7M. Higaki , K. Koizumi , T. Ando , et al., “Extranodal Extension in Oral Squamous Cell Carcinoma: Clinical and Histopathological Analysis,” Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology 137 (2024): 632–639.38679502 10.1016/j.oooo.2024.03.008 · doi ↗ · pubmed ↗
- 8A. Tarsitano , M. L. Tardio , and C. Marchetti , “Impact of Perineural Invasion as Independent Prognostic Factor for Local and Regional Failure in Oral Squamous Cell Carcinoma,” Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology 119 (2015): 221–228.25487983 10.1016/j.oooo.2014.10.004 · doi ↗ · pubmed ↗