Persistent Anemia in an HIV Patient: The Role of Parvovirus B19
Priscila M Fiallo, Larry M Bush, Maria T Vazquez-Pertejo

TL;DR
This paper discusses how parvovirus B19 can cause chronic anemia in HIV patients and highlights the importance of early diagnosis and treatment.
Contribution
The paper emphasizes the under-recognized role of parvovirus B19 in causing persistent anemia in HIV patients and advocates for early diagnosis.
Findings
Parvovirus B19 can cause chronic anemia in immunocompromised individuals like those with HIV.
Intravenous immunoglobulin can effectively treat B19V-induced anemia in HIV patients.
B19V infection is often overlooked in HIV patients due to lack of routine monitoring.
Abstract
Parvovirus B19 (B19V) is a common single-stranded DNA virus that infects humans and is its only host. Although infection is often asymptomatic, B19V can cause significant hematologic disease due to its tropism for erythroid progenitor cells. Immunocompromised individuals, including those with human immunodeficiency virus (HIV), are susceptible to persistent infection and may develop pure red cell aplasia (PRCA) and chronic anemia. Since B19V infection is not routinely monitored in the United States, and its symptoms can overlap with other causes of anemia in HIV, diagnosis may be overlooked. Early identification is critical, as intravenous immunoglobulin (IVIG) can rapidly restore erythropoiesis and reverse transfusion dependence.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
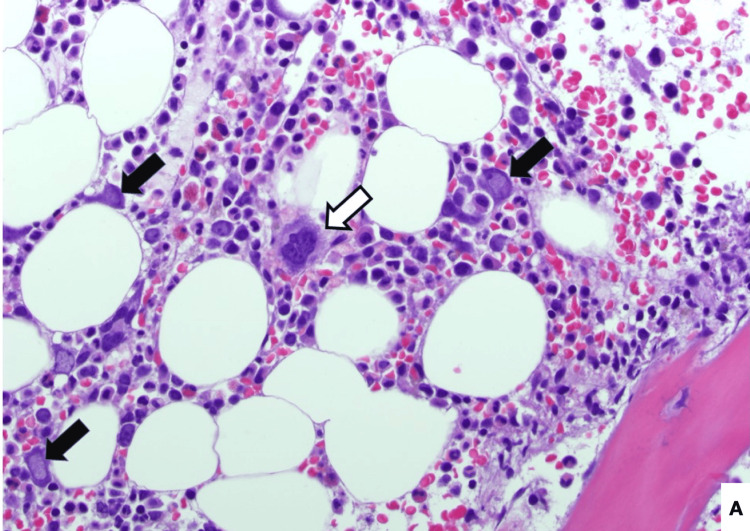 Figure 1
Figure 1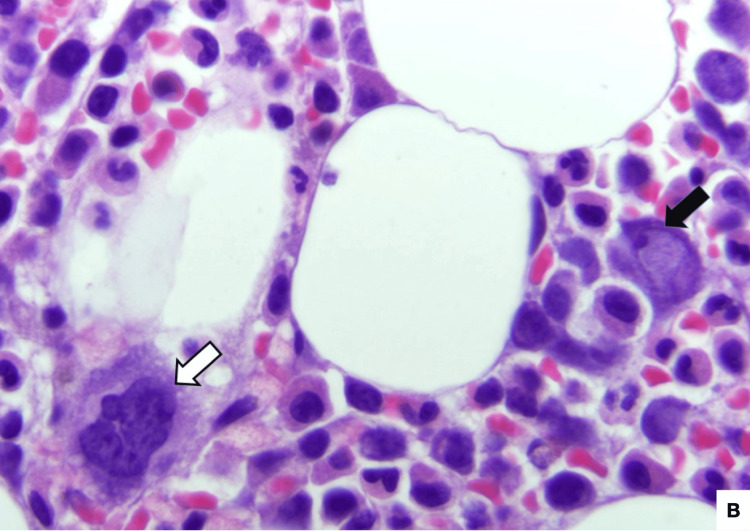 Figure 2
Figure 2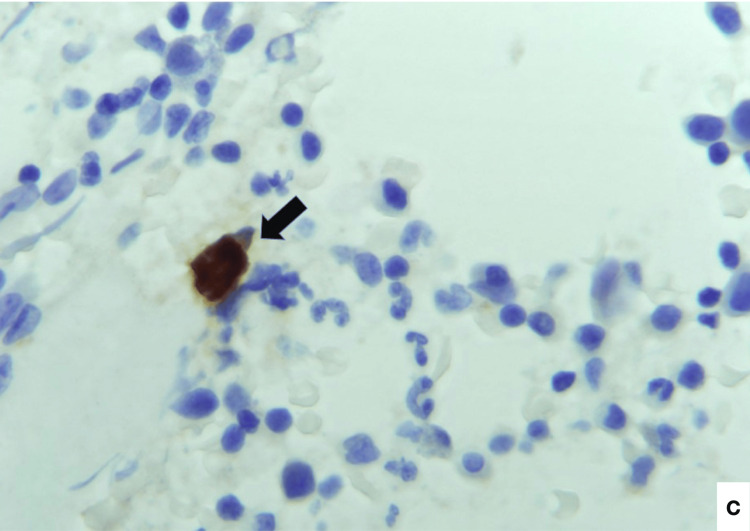 Figure 3
Figure 3| Laboratory (units) | Normal Ranges | Day 1 of admission | Day 2 of admission | Day 3 of admission | Day 4 of admission | Day of discharge |
| Hematology | ||||||
| WBC (x103/µL) | 4.5-10.5 | 4.01 | 4.98 | 5.19 | 6.21 | 5.28 |
| RBC (x106/µL) | 4.4-6.15 | 1.72 | 2.11 | 2.73 | 2.44 | 2.73 |
| Hgb (g/dL) | 14-18 | 4.7 | 6.1 | 7.6 | 6.9 | 7.9 |
| Hct (%) | 40-54 | 13.8 | 16.6 | 21.6 | 19.6 | 21.9 |
| MCV (fL) | 81-96 | 80.2 | 78.7 | 79.1 | 80.3 | 80.2 |
| MCH (pg) | 27-34 | 27.3 | 28.9 | 27.8 | 28.3 | 28.9 |
| MCHC (g/dL) | 32-36 | 34.1 | 36.7 | 35.2 | 35.2 | 36.1 |
| RDW-SD (fL) | 36-50 | 50.5 | 47.5 | 48.8 | 50.3 | 49 |
| RDW-CV (%) | 11-14.5 | 17.5 | 16.8 | 16.8 | 17.2 | 16.6 |
| Platelets (x103/µL) | 150-450 | 312 | 283 | 316 | 325 | 282 |
| MPV (fL) | 6.9-10.5 | 10.3 | 10.3 | 9.9 | 10.8 | 9.9 |
| Received transfusion | Received transfusion | Received transfusion | ||||
| Chemistry | ||||||
| Iron (µg/dL) | 65-175 | 197 | ||||
| TIBC calculated (µg/dL) | 250-450 | 191 | ||||
| Transferrin (mg/dL) | 202-364 | 153 | ||||
| Ferritin (mg/dL) | 8-388 | 925 | ||||
| Glucose (mg/dL) | 74-106 | 96 | 94 | 98 | 88 | 108 |
| Sodium (mmol/L) | 134-148 | 141 | 140 | 141 | 141 | 139 |
| Potassium (mmol/L) | 3.6-5.2 | 3.3 | 3.8 | 3.8 | 3.6 | 3.7 |
| Chloride (mmol/L) | 95-110 | 110 | 113 | 11 | 112 | 109 |
| CO2 (mEq/L) | 21-32 | 28 | 25 | 25 | 23 | 28 |
| AGAP (mmol/L) | 5-15 | 6.3 | 6.8 | 8.8 | 9.6 | 5.7 |
| BUN (mg/dL) | 7-18 | 11 | 13 | 10 | 10 | 8 |
| Creatinine (mg/dL) | 0.7-1.3 | 1.07 | 0.86 | 0.95 | 0.81 | 0.9 |
| BUN/Creat Ratio | N/A | 10 | 15 | 11 | 12 | 9 |
| Calcium (mg/dL) | 8.5-10.1 | 8.7 | 8.6 | 8.4 | 8.1 | 8.8 |
| eGFR Cr (mL/min/1.732) | N/A | 92 | 106 | 116 | 112 | |
| Others | ||||||
| HIV-1 RNA by PCR (copy/mL) | N/A | 13500 | ||||
| log10 HIV-1 RNA (copy/mL) | N/A | 4.13 | ||||
| % CD-4 (%) | 30.8-58.5 | 14.5 | ||||
| Absolute CD-4 (cells/µL) | 359-1519 | 232 | ||||
| Parvovirus IgM Index | 0.0-0.8 | 2.1 | ||||
| Parvovirus IgG Index | 0.0-0.8 | 0.5 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsParvovirus B19 Infection Studies · Blood groups and transfusion · Autoimmune and Inflammatory Disorders
Introduction
Parvovirus B19 is a single-stranded DNA virus member of the Parvoviridae family, having humans as the only known host [1]. Transmission of infection is primarily via the respiratory route, but may also occur through blood or blood products, as well as through organ transplantation. While approximately 50% of children have serologic evidence of infection, this figure reaches 80% in the elderly population, as the acquisition of infection continues throughout adolescence into adulthood [2]. Infection with B19V is not a notifiable disease in the United States and is not routinely surveilled; however, a rise in reported cases has been observed in 2024. A large portion of those infected remain asymptomatic or subclinical. Nevertheless, dependent on the immunologic and hematologic status of the host, infected individuals may present with a wide variety of disease manifestations [3].
Erythema infectiosum, more commonly referred to as the fifth disease or “slapped cheek” disease, is the most common childhood presentation. Infection during pregnancy may lead to fetal death in utero, hydrops fetalis, or, rarely, the development of congenital anemia. In the immunocompromised host, B19V can cause transient aplastic anemia. Persistent viremia can result in pure red cell aplasia (PRCA) and chronic anemia [3,4]. The prevalence of B19V-induced anemia in HIV-seropositive patients is probably higher than that generally recognized [5]. We report a case of severe, transfusion-dependent anemia in an HIV-infected adult ultimately diagnosed with B19V-associated PRCA, highlighting the importance of maintaining clinical suspicion for this treatable condition.
Case presentation
An asymptomatic 37-year-old HIV-infected man was referred to the hospital due to severe anemia. Physical examination was unremarkable except for pale conjunctivae. On admission, the hematogram revealed hemoglobin (Hgb) of 4.7 g/dl, hematocrit (HCT) of 13%, mean corpuscular volume (MCV) of 80 fl, white blood cell count (WBC) of 4.01x10³/μl, and platelets (PLTS) of 312x10³/μl (Table 1). He had a history of chronic anemia requiring transfusions, the etiology of which had not been previously determined. His CD4 T-cell lymphocyte count was 232 cells/ml (14.5%) with an HIV RNA load of 13,500 copies while being treated with bictegravir/emtricitabine/tenofovir-alfenamide. He tested positive for immunoglobulin M (IgM) but negative for IgG anti-B19V antibodies (Table 1). Quantitative, real-time polymerase chain reaction (PCR) testing for parvovirus B19 DNA was not performed due to a lack of availability. A bone marrow biopsy revealed marked erythroid hypoplasia with scattered large, atypical cells displaying abnormal erythroblast morphology (Figures 1, 2). These cells contained prominent ground-glass intranuclear viral inclusions, which stained positive for B19V by immunohistochemistry (Figure 3), supporting the diagnosis of B19V-associated PRCA.
Bone marrow bone core biopsy, 200x, Hematoxylin and eosin (H&E) stain. B19V-infected erythroid precursor cells (black arrows indicate intranuclear viral inclusions; white arrows indicate megakariocytes for comparison).
Bone marrow aspirate, 400x, Hematoxylin and eosin (H&E) stain. B19V-infected erythroid precursor cell (black arrow points to an intranuclear viral inclusion; white arrow indicates a megakaryocyte for comparison).
Bone marrow aspirate biopsy, 400x, B19V immunohistochemical stain - positive stain in an infected erythroid precursor cell (black arrow).
Discussion
Although rare in HIV-infected patients, B19V-related anemia is likely underdiagnosed [5]. Persistent parvovirus infection in such individuals is due to inadequate neutralizing antibody production secondary to a poorly functioning adaptive immune response. Adequate IgM and IgG antibody production is required for the elimination of B19V. The role of the cellular immune response in limiting B19V infection has been studied less intensively [6,7]. Despite antiretroviral therapy, our patient’s elevated HIV viral load and reduced CD4 T-cell percentage suggest non-compliance with his regimen [5]. Diagnosis requires clinical suspicion and is supported by the detection of anti-B19V antibodies along with B19V DNA PCR. Since viral isolation is not reliable, confirmation relies on the use of specific immunohistochemical stains to validate the presence of B19V in erythroid precursor cells. IVIG is the treatment of choice in severe cases. If relapse occurs less than six months after the initial treatment, an empirical maintenance treatment with a single-day infusion of 0.4 g/kg IVIG every four weeks may control the B19V viremia [8,9].
Conclusions
Parvovirus B19 is an underdiagnosed yet treatable cause of severe anemia in immunocompromised patients, including those with HIV. To diagnose this condition, clinical suspicion should be supported by serological testing, and, if available, PCR testing and immunohistochemical staining for confirmation. Prompt recognition and management are key to preventing ongoing transfusion dependence and optimizing patient care. Therefore, increased awareness of Parvovirus B19 in immunocompromised populations is essential for healthcare professionals.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Human parvoviruses Clin Microbiol Rev Qiu J Söderlund-Venermo M Young NS 431133020172780699410.1128/CMR.00040-16PMC 5217800 · doi ↗ · pubmed ↗
- 2Seroprevalence of parvovirus B 19 in the German population Epidemiol Infect Röhrer C Gärtner B Sauerbrei A 1564157513620081819800310.1017/S 0950268807009958 PMC 2870752 · doi ↗ · pubmed ↗
- 3Parvovirus B 19: insights and implication for pathogenesis, prevention and therapy Asp Mol Med Zakrzewska K Arvia R Bua G Margheri F Gallinella G 10000712023 https://www.sciencedirect.com/science/article/pii/S 2949688823000072?via%3Dihub
- 4Human parvovirus B 19: a review Acta Virol Rogo LD Mokhtari-Azad T Kabir MH Rezaei F 1992135820142528385410.4149/av_2014_03_199 · doi ↗ · pubmed ↗
- 5Clinical presentation of parvovirus B 19 infection in adults living with HIV/AIDS: a case series Viruses Mendes-de-Almeida DP Bokel JP Alves AD 11241520233724321010.3390/v 15051124 PMC 10223798 · doi ↗ · pubmed ↗
- 6Tale of two viruses: parvovirus B 19 and HIVBMJ Case Rep Hernstadt H Randell P Fidler S Foster C 014202110.1136/bcr-2020-239153 PMC 806183133879461 · doi ↗ · pubmed ↗
- 7Seroprevalence and associated outcomes of parvovirus B 19 infection in human immunodeficiency virus patients: a systematic review Avicenna J Med Mohamed SO Mohamedelmugadam RA Almardi SA Ahmed TH Ibrahim ME Mohamedali AO 1851931420244008422710.1055/s-0045-1801865 PMC 11896723 · doi ↗ · pubmed ↗
- 8A persistent parvovirus infection causing anemia in an HIV patient requiring intravenous immunoglobulin maintenance therapy Cureus Gor D Singh V Gupta V Levitt M 014202210.7759/cureus.24627 PMC 915118135664410 · doi ↗ · pubmed ↗