Midlife aging and performance study (MAPS): evaluating biological aging through a physical capacity battery
Roy Tzemah-Shahar, Ilona Shapiro, Einat Kodesh, Merav Asher, Yechiel Friedlander, Hagit Hochner, Maayan Agmon

TL;DR
This study shows that physical performance in midlife is linked to biological aging, offering a practical way to assess and promote healthier aging.
Contribution
The study introduces a physical capacity battery as a behavioral marker for biological aging assessment.
Findings
Better performance in strength, endurance, balance, and flexibility correlates with younger biological age.
Lower composite physical capacity scores are associated with accelerated aging states.
Each increase in physical capacity score reduces the odds of accelerated aging by 60%.
Abstract
Aging is a risk factor for the development of chronic diseases; however, it is heterogeneous. Measuring aging in midlife, commonly done using laboratory markers and statistical methods for estimation of biological age (BA), cannot directly inform behavioral intervention goals aiming to promote healthier aging. The Midlife Aging and Performance Study (MAPS) examined the association between an extended, inclusive assessment of physical capacity (PC), as a behavioral marker of aging, and BA, estimated using the Klemera-Doubal method from 11 laboratory and physiological biomarkers, in 112 individuals aged 42–46 (47% women). PC was comprehensively measured by a battery covering five domains: muscle strength, endurance, balance, agility and flexibility. Better performance in strength, endurance, balance, and flexibility domains was correlated with younger BA (Pearson’s r 0.33–0.49, p <…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
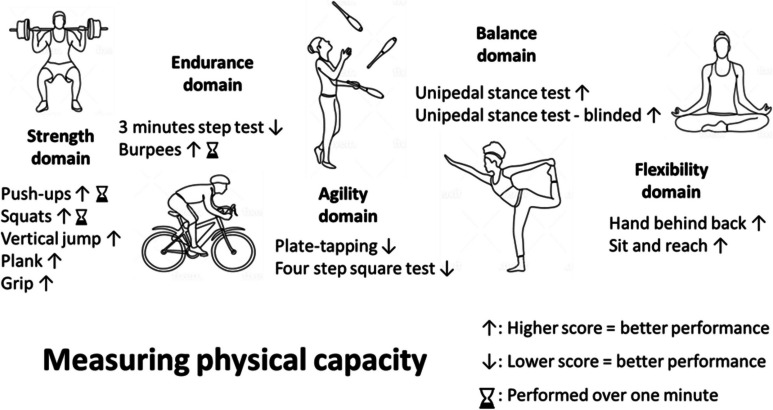 Figure 1
Figure 1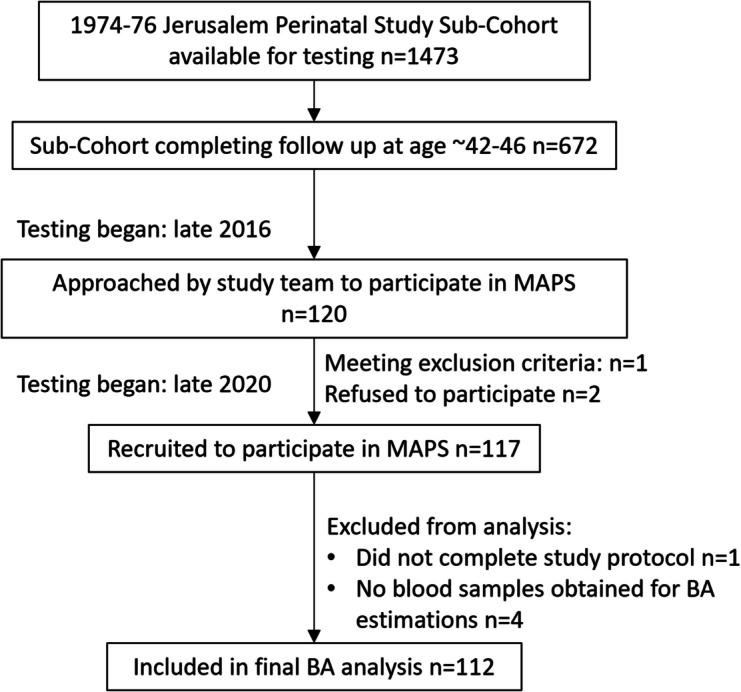 Figure 2
Figure 2- —NIH
- —Israeli Science Foundation
- —http://dx.doi.org/10.13039/501100003976Israel National Institute for Health Policy Research
- —The Rina Brick Memorial Foundation
- —University of Haifa
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBody Composition Measurement Techniques · Nutrition and Health in Aging · Children's Physical and Motor Development
Introduction
Aging is a risk factor for the development of chronic diseases and functional decline, yet the aging process is highly diverse [1]. Biological age (BA) captures both between and within individual heterogeneity of aging by representing the overall body state [2], thus better estimating health-related status than chronological age (CA) alone [3]. Given the rising prevalence of age-related diseases [4], quantifying aging has become a frequent focus in research [5], and may assist in identifying individuals at risk for accelerated aging (where BA > CA), promoting personalized preventive interventions [6, 7]. Although there is no single gold standard for estimating BA, many studies use laboratory-based methodologies, such as molecular ageing clocks [8] that offer an acceptable quantification for different aspect of aging [9–11], while other studies quantify BA using a composition of laboratory and physiological markers [12–14]. Methods based on laboratory markers are costly, making them primarily suitable for research [15]. Furthermore, laboratory methods are less practical as a means to informing behavioral changes [16], such as promoting a more active lifestyle, leading to a better physical state and healthier aging process [17, 18].
Physical capacity (PC) [19], defined as a collection of functional markers associated with health and aging [20, 21], can serve as an alternative to the laboratory-based BA measurement, capturing individual’s health status by using behavioral markers of function [22, 23]. Although PC has been previously proposed as a means to quantify aging [24, 25], majority of available studies focus on muscular strength, or use a narrow testing battery [23], thus limiting our ability to effectively use PC markers in aging research. Published tests tend to ignore personal ability and sex-specific differences in performance [26, 27]. Moreover, the majority of available literature on function focuses on older adults, overshadowing the midlife period, a critical window of opportunity to facilitate a positive lifestyle change to improve the aging process [28]. Lastly, limitations of previous studies arise from the methods used in estimating BA, such as telomere length or specific laboratory markers that do not examine aging status comprehensively [23].
Filling these gaps is important for several reasons. First, PC is a broad concept, covering many distinct domains—muscular strength, endurance, flexibility, agility, and balance—corresponding with different ability requirements. Using a composite and inclusive measure of PC can provide an extensive representation of the body’s functional state [23] and available physical intrinsic capacity [29]. Second, to accommodate varying performance levels or possible sex-related differences [30], multiple tests with graded difficulty should be used when assessing PC. Moreover, midlife adults typically demonstrate relatively high physical ability yet remain understudied in aging research; using a graded approach in this age group can support enhanced detection of subtle inter-individual differences in PC that may relate to accelerated aging processes [2]. Lastly, by estimating BA using a composite measure based on laboratory and physiological markers [31] and comparing it with PC, the link between PC and aging state can be better understood. Developing PC measures for BA estimation that address these limitations can offer a practical and feasible alternative to the laboratory-based methodologies that is both community-accessible and informative for promoting positive health behavioral changes [32].
The Midlife Aging and Performance Study (MAPS) aims to examine the association between an extended, inclusive measure of PC—covering five functional domains—and BA in midlife, considering sex differences and leveraging graded levels of performance.
Methods
This study comprises a subset of the Jerusalem Perinatal Study [33]; participants from the most recent follow-up point, at ages 42–45 (conducted between 2016 and 2021) [34], that were willing to take part in an extension study were included in MAPS. The inclusion criterion was a subjective ability to engage in leisure time exercise. Exclusion criteria were (a) acute illness (in the week prior to the testing day); (b) acute musculoskeletal complaint (e.g., acute low back pain) or known chronic condition (e.g., cardiovascular disease) subjectively limiting participation in physical exercise; and (c) use of medications that might influence physical performance or pose a risk when performing exercises (e.g., non-steroid anti-inflammatory drugs) on testing day. Each participant received general information on the study aims and provided signed informed consent prior to testing. The Ethics Committee of the Faculty of Social Welfare and Health Sciences at the University of Haifa (#407/20) and the Hadassah Hospital Institutional Review Board (#10–01.04.05) provided ethical approval for this study.
BA estimation
Eleven biomarkers were used to estimate BA: six fasting blood measures (glucose, insulin, high-density lipoproteins, low-density lipoproteins, triglycerides, total cholesterol) and five physiological markers (body mass index, diastolic resting blood pressure, systolic resting blood pressure, resting heart rate, and waist circumference) were added to the Klemera-Doubal method (KDM) [12] algorithm using the BioAge R package [31] to calculate BA. KDM estimates BA by weighing each marker according to its correlation with chronological age in training cohort data [12]. BioAge uses the third United States Health and Nutrition Examination Surveys (NHANES) [35] dataset as the training cohort. Thus, participants’ BA was estimated by determining the corresponding CA at which an individual’s biomarkers would be considered normal in the training dataset. See Supplementary Table S1 for additional information.
Physical capacity measurements
Measuring PC requires testing individuals’ abilities to perform tasks that capture different aspects of physical function; there are a range of fitness tests suitable for measuring PC, accounting for age and sex differences and PC domains of interest [36–38]. Five main PC domains were identified and previously studied in the context of BA (strength, endurance, agility, balance, flexibility); here, we measured these domains using 13 different tests (Fig. 1). Specific test selection was based on suitability to a home environment and, where possible, previous validation in a similar population. A detailed list of performed tests and testing procedure is provided in Supplementary Table S1. Calculations of domain specific and composite PC (ΣPC) scores were based on standardized ranking and percentile calculation, performed separately for each sex, like a previously used method for calculating ΣPC [39]. First, each test’s results were categorized based on percentiles on a scale of 0 to 1 (1 corresponding with best performance); domain scores were derived by averaging the standardized results of included tests (Fig. 1). We calculated ΣPC scores by summing the five domains, for a total score ranging from 0 to 5. See Supplementary Table S2 for additional information on standardization processes. Subjective perceived exertion in the entire testing session was also recorded, by asking each participant to rate his or her exertion once the session was over, on a visual analogue scale (VAS) ranging from 0 to 10 (10 corresponding with maximal exertion) [40]. Fig. 1. Physical capacity tests by domain
Data analysis
Analysis of results was conducted using IBM SPSS v.27.0.0.0. We compared MAPS cohort and Jerusalem Perinatal Study sub-cohort to identify significant differences. The associations between the different standardized tests or PC domain scores and BA were examined using Pearson’s partial correlation, controlling for chronological age. Significantly correlated domains were then included in a linear regression model to identify the independent contribution of each domain to BA, while controlling for chronological age. Lastly, we estimated the contribution of ΣPC to being in an accelerate aging state: The differences between BA and CA were dichotomized (∆Age > 0 representing accelerated aging state, ∆Age ≤ 0, normal to slower aging), and a logistic regression was used to assess the effect (odds ratio) of ΣPC on accelerated aging state, controlling for CA. Investigation of sex-specific differences in PC performance was done by comparing tests results scores prior to the ranking procedure, tests completion rates, and reported exertion levels of the entire testing procedure (examined using t-tests or Mann–Whitney tests, as appropriate).
Results
Participant characteristics
The latest Jerusalem Perinatal Study follow-up at age ~ 42–46 years included a total of n = 672 individuals from the complete original cohort. Data collection began in late 2016, while collection for MAPS began in November 2020 and was completed by November 2021, when the pool of volunteers was exhausted. A total of 120 individuals were approached, and 117 consented to participate in MAPS (see Fig. 2). One man was excluded due to subjective complaints of acute lower back pain limiting his ability to participate in physical exercise, and two women refused participation. Of the remaining 117 participants, five were omitted from the final analysis: one man was unable to complete the testing battery due to an adverse response to the physical effort, resulting in termination of testing (the participant had complaints of nausea and chest pain and was referred to an emergency room, resulting in coronary artery catheterizations for previously undiagnosed coronary arteries disease), and four participants did not provide the blood samples needed for BA estimation. Demographics, anthropometric data, and BA estimation of the 112 participants (53 women, 47%) included in the analysis, and comparisons with the remaining Jerusalem Perinatal Study sub-cohort tested are presented in Table 1. This comparison revealed that individuals consenting to participate in MAPS were slightly older (the age differences were associated with majority of Jerusalem Perinatal Study participants being examined before COVID-19 pandemic, while MAPS participants were examined later, following the first pandemic waves), with participating men having a lower BMI and smoking less than the men in the overall sub-cohort. Fig. 2. Study procedures flow chartTable 1MAPS cohort characteristics and selection bias analysisMAPS (mean ± SD) N = 112Jerusalem Perinatal Study sub-cohort (mean ± SD)^1^, N = 560Women (n = 53)Men (n = 59)Women (n = 285)Men (n = 275)CA (years)^2^44.5 ± 1.444.5 ± 1.442.9 ± 1.143.0 ± 1.2BMI26.8 ± 4.627.0 ± 3.927.6 ± 6.028.5 ± 4.6Waist circumference (cm)^3^85.3 ± 11.896.5 ± 11.185.9 ± 12.698.3 ± 12.0Education (years)15.9 ± 1.916.6 ± 3.415.3 ± 2.615.9 ± 4.2Smoking (pack years)1.3 ± 3.31.9 ± 3.11.2 ± 3.54.5 ± 6.6CA chronological age, MAPS Midlife Aging and Performance Study, BMI body mass index, SD standard deviation^1^Comparisons between male and female participants included in MAPS and the remaining sub-cohort revealed significant differences in age for both sexes, and differences in BMI and smoking for men only (included men had lower BMI and lower smoking pack years). The observed age difference was associated with the time difference between Jerusalem Perinatal Study follow-up and MAPS initiation.^2^Age at time of blood sample collection.^3^Women/men statistically different in MAPS and the complete sub-cohort, T-test, p < 0.05.
BA estimation and PC testing battery
In the MAPS cohort, BA ranged from 31.3 to 51.3 years with accelerated aging in just under 40% of individuals. We did not find significant differences in these measures (Table 2). Raw PC test results are also presented in Table 2, as well as the attrition rates of each test performed. Average completion rates were over 95% for both women and men; note that almost half of the women (N = 23, 43%) were unable to complete the three-minutes step test (3MST), leading to its early termination (later imputed to the lowest category, see Supplementary Table S2). This could originate from the 30-cm step height, posing a greater challenge to women. The push-up test was also more difficult for women: 28% of women completed two repetitions or less. Note that regardless of any significant differences in performance, reported exertion levels of women and men were comparable. Table 2. Biological age (BA) and physical capacity (PC) measuresWomenMenSex differences^1^BA (mean ± SD; range)43.1 ± 5.8; 31.3,54.943.8 ± 6.2; 32.8,57.3p = 0.72∆Age (mean ± SD; range) (% accelerate aging) − 1.4 ± 5.5; − 12.3,10.3 (36%) − 0.7 ± 6.4; − 12.2,14.8 (39%)p = 0.77Physical CapacityMean ± SD; rangeN (completed test %)Mean ± SD; rangeN (completed test %)StrengthSquats (reps)36.2 ± 10.4;15,60.553(100%)41.3 ± 10.7; 20,7059(100%)p = 0.01Push-ups (reps)7.4 ± 6.1;0,2050(94%)20.4 ± 10.4;3,4459(100%)p** < 0.01Grip (kg)21.7 ± 6.5;10.2,36.853(100%)35.8 ± 8.6;15.67,50.1559(100%)p < 0.01Vertical Jump (cm)14.3 ± 4.6;4.4,26.049(93%)26.5 ± 6.3;14.7,40.056(95%)p < 0.01Plank (s)64.7 ± 45.3;2.8,20053(100%)100.9 ± 43.7;17,20057(97%)p < 0.01FlexibilityHBB (cm) − 4.0 ± 6.3; − 23.5,10.853(100%) − 8.9 ± 9.1; − 29.5,9.559(100%)p < 0.01Sit and reach (cm)0.8 ± 9.9; − 20,2353(100%) − 8.8 ± 11.9; − 33,1159(100%)p < 0.01Endurance3MST (heart rate)^2^124.3 ± 15.8;94.0,153.630^4^(57%)121.3 ± 18.4;79.0,170.854(92%)p = 0.43Burpees4.9 ± 4.7;0,1851(96%)10.4 ± 4.8;1,2159(100%)p < 0.01AgilityPTT (s)16.5 ± 3.7;11.2,27.153(100%)14.0 ± 3.5;9.5,2359(100%)p < 0.01FSST (s)5.8 ± 1.0;3.6,7.8453(100%)5.7 ± 1.3;3.4,9.159(100%)p = 0.64BalanceUPST (s)27.7 ± 4.6;12.1–3053(100%)28.1 ± 4.6;8.4,3059(100%)p = 0.51UPST blinded (s)11.5 ± 6.2;3.1,27.553(100%)16.2 ± 9.3;3.2,3059(100%)p = 0.02**Perceived exertion (VAS)5.0 ± 2.4; 0,953(100%)5.5 ± 2.4; 0,859(100%)p = 0.23∆Age the difference between BA and CA (∆Age = BA-CA), HBB hand behind back, 3MST 3 min step test, PTT plate tapping test, FSST four step square test, UPST unipedal stance test, VAS visual analogue scale^1^Differences examined using t-test/Mann–Whitney test.^2^Out of the 23 women that did not complete this test, 21 terminated the test before it ended.
Correlation between BA and PC measures
In the MAPS cohort, strength, flexibility, endurance, and balance domains were significantly negatively correlated with BA, controlling for CA (Table 3). Since standardization of PC scores accounted for any sex-specific differences, correlations were assessed across the full sample rather than stratifying by sex. We examined the independent contribution of significantly correlated domains (i.e., strength, flexibility, endurance, and balance) to BA using a linear regression model, demonstrating that better performance in endurance, agility, and balance domains was significantly associated with younger BA (Table 4). The logistic regression model used to assess the relationship between ΣPC and a dichotomized ∆Age explained 22% of the variance in participants’ accelerated aging status (Nagelkerke R^2^ = 0.22) with an area under the curve of 0.73 (95% CI 0.64–0.83; p < 0.001); ΣPC was the only significant variable in the model, with an odds ratio of 0.40 (95% CI 0.25–0.64), showing that each incremental increase in ΣPC corresponded with a 60% reduction of the odds being in an accelerated aging state. Table 3. Pearson’s partial correlation between physical capacity measures (individual tests domain averages, and ΣPC, respectively) and BA, controlling for CAPerson’s correlation rSignificanceStrength domainSquats − 0.16p = 0.10Push-ups − 0.30p** < 0.01Grip0.02p = 0.86Vertical jump − 0.15p = 0.12Plank − 0.47p***** < 0.01Strength domain − 0.33p***** < 0.01Flexibility domainHBB − 0.29p***** < 0.01Sit and reach − 0.37p***** < 0.01Flexibility domain − 0.44p***** < 0.01Endurance domain3MST − 0.45p***** < 0.01Burpees − 0.33p***** < 0.01Endurance domain − 0.49p***** < 0.01Agility domainPTT0.04p = 0.69FSST − 0.15p = 0.12Agility domain − 0.07p = 0.50Balance domainUPST − 0.34p***** < 0.01UPST blinded − 0.31p***** < 0.01Balance domain − 0.38p***** < 0.01** − 0.49p*** < 0.01**Abbreviations: PC physical capacity, BA biological age, CA chronological age, HBB hand behind back, 3MST 3 min step test, PTT plate tapping test, FSST four step square test, UPST unipedal stance test, ΣPC composite physical capacity Table 4A linear regression model examining PC domain association with BA while controlling for CAVariableCoefficients BSignificance (95% CI)Adjusted R^2^ = 0.33, p < 0.01Strength domain0.08p = 0.47 (− 3.28, 7.12)Flexibility domain − 0.29p < 0.01 (− 9.78, − 2.46)Endurance domain − 0.38p < 0.01 (− 11.17, − 3.45)Balance domain − 0.19p = 0.03 (− 7.71, − 2.46)CA0.03p = 0.73 (− 1.15, 1.63)PC physical capacity, BA biological age, CA chronological age.*Agility domain was omitted from this analysis, as it was not significantly correlated with BA.
Discussion
The aims of this study were to examine the association between an extended, inclusive measure of PC and BA in midlife, as a feasible alternative to the widely reported laboratory biomarkers. This work adds to previous literature by showing that different behavioral marker of physical capacity can be used for assessing health-related body state at midlife [23], transcending previous work estimating BA using limited PC measures in conjunction with laboratory biomarkers [41, 42]. This study addressed the limitations of previously published work by using a comprehensive testing battery, investigating midlife individuals, and quantifying BA using a composite measure. These findings show the link between PC measures, as a possible community-based alternative to laboratory-based methodologies for BA estimation, thus supporting screening of midlife individuals at greater risk for accelerated aging status [43], enabling personalized lifestyle interventions focusing on healthy and active aging [44].
We demonstrate that a PC testing battery could be used for estimating biological aging in midlife healthy individuals: (1) As a composite score, increased PC was associated with younger BA and reduced risk of being in an accelerated aging state; (2) better performance in strength, endurance, balance, and flexibility domains was significantly associated with younger BA, while agility performance was not; (3) subjectively reported exertion levels of women and men were comparable, and total attrition rates were low, suggesting the testing battery, as a whole, was suitable for both sexes and wide ability level.
Considerations for PC battery
The battery presented here covered a wide range of physical functions, aiming to provide a comprehensive measurement of the physical state of the human body. Observed sex differences in most tests (see Table 2) [45, 46] can be explained by sex-specific muscle mass [30], cardiovascular regulation [47], or even respiratory capacity [48]. These differences support using multiple tests in each domain, to account for personal variation in performance. Some modifications in the battery should be made, adapting the tests for female performance level (i.e., modifying the 3MST and push-up test). Note that the agility tests we used, and the agility domain in general, were not correlated with BA. One possible explanation for this finding is the complexity of agility performance—an interaction of both PC and cognition [49], requiring a different approach when studied in the context of midlife individuals, perhaps calling for the use of tests that are considerably more difficult. Nonetheless, as agility offers insight into certain dimensions of PC, we recommend keeping this domain in future investigations, including more vigorous agility tests, ensuring every aspect of PC is accounted for.
Midlife as a window of opportunity for healthy-aging promotion interventions
Unveiling the role function plays during midlife is a key to increasing health and lifespan [50, 51]. However, the need for population-wide early detection methods, similar to functional testing batteries designed for older adults (e.g., BESTest[52]), remains largely unanswered. Promotion of healthier aging in midlife is an easier task than curing diseases that have already developed [53], and the suggested testing battery, performed in midlife, can be used both for successfully communicating an easily conveyed functional goal [54] and for monitoring intervention outcomes that may induce a positive change of cardiometabolic state [55]. As such, it could support our efforts to ameliorate the global burden of aging. Additional studies focusing on midlife are required to further establish the contribution of using these markers to inform the public of recommended behavior changes.
PC as a substitute for BA estimation methods
Many methodologies are currently available for BA estimations [53, 56, 57]. We used a single BA estimation based on a set of blood and physiological biomarkers that were readily available for calculation. KDM-estimated BA is a well-established, effective predictor when it comes to health-function and mortality [41], even when compared with other established methods [53]. The precision of biological clocks depends on sex, as there are differences in life span and health metrics of aging women and men [58, 59]. By showing PC is associated with KDM BA, we place PC as a robust measure for body state, bridging the male–female health-survival paradox [59, 60]. These results suggest that function and performance as health metrics may go beyond the role any specific marker plays in aging mechanism, and reflect on available physical intrinsic capacity [61]. Moreover, identifying the contribution of specific PC domains in this health-related assessment echoes health organizations’ recommendations for adopting active lifestyle, framing PC assessment as a preventive health screening test. Considering that better performance equals younger BA, it enables personalized intervention strategies and allows for easy-to-follow changes in health status that can be monitored even by the patient themselves.
Strengths and limitations
A major strength of this study is the comprehensive PC testing battery, covering all PC domains that were previously separately associated with aging, while offering a robust measurement across ability levels of normal, healthy, midlife individuals. Although limiting the tests to home-based assessment contributed to the usability of the testing battery, it might ignore biases associated with testing environment, potentially impacting physical performance. Furthermore, we did not account for any selection bias, cognitive, psychological, or sensory capacities that may contribute to BA differences and should be considered in future investigation. Using a single method to estimate BA provides a somewhat narrow perspective on BA, as different methods focus on different aging mechanisms. Larger, population-based studies are needed to further establish the use of PC at a means to estimate BA. Lastly, as this study is limited to cross-sectional data, it does not provide additional information on the role PC plays in predicting BA and accelerated-aging state or offer insights on causal links between the two.
Conclusions
The suggested PC battery, composed of five PC domains, may offer additional insight on aging state, supporting the identification of midlife individuals at risk for accelerated aging state, while being sensitive enough to reflect different performance ability levels. Specific PC domains and a composite PC score were correlated with BA, emphasizing that behavioral markers could be used to estimate aging state in midlife. Although many studies focus on aging mechanisms to find a cure for “aging disease,” this study emphasizes the importance of identifying individuals at risk for accelerated aging trajectories, supported by the consensus that a lifestyle change can be used to improve health. Clinicians of all professions should assess aging risk and offer personalized behavioral interventions addressing age-related diseases. Physical capacity assessment outcomes can be communicated to the individual tested, not only as an estimate of potential risks, but also as a means of providing a feasible, attainable goal that could be longitudinally monitored.
Supplementary Information
Below is the link to the electronic supplementary material.ESM 1(DOCX 31.9 KB)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lohman T, Bains G, Berk L, Lohman E. Predictors of biological age: the implications for wellness and aging research. Gerontol Geriatr Med. 2021; 7. 10.1177/2333721421104641910.1177/23337214211046419 PMC 847768134595331 · doi ↗ · pubmed ↗
- 2Erema VV, Yakovchik AY, Kashtanova DA, Bochkaeva ZV, Ivanov MV, Sosin DV, et al. Biological age predictors: the status Quo and future Trends. Int J Mol Sci. 2022; 23(23):15103.10.3390/ijms 232315103 PMC 973954036499430 · doi ↗ · pubmed ↗
- 3Patrizio E, Calvani R, Marzetti E, Cesari M. Physical functional assessment in older adults. J Frailty Aging. 2020; p. 1–9. 10.14283/jfa.2020.61.10.14283/jfa.2020.6133575703 · doi ↗ · pubmed ↗
- 4Bautmans I, Knoop V, Amuthavalli Thiyagarajan J, Maier AB, Beard JR, et al. WHO working definition of vitalitycapacity for healthy longevity monitoring. Lancet Healthy Longev. 2022; 3(11), e 789–e 796. 10.1016/s 2666-7568(22)00200-810.1016/S 2666-7568(22)00200-8PMC 964093536356628 · doi ↗ · pubmed ↗
- 5Cooper R, Strand BH, Hardy R, Patel KV, Kuh D. Physical capability in mid-life and survival over 13 years offollow-up: British birth cohort study. BMJ. 2014; g 2219–g 2219. 10.1136/bmj.g 221910.1136/bmj.g 2219 PMC 400478724787359 · doi ↗ · pubmed ↗
- 6Sierra F. The emergence of geroscience as an interdisciplinary approach to the enhancement of health span and life span. Cold Spring Harbor perspectives in medicine. 2016;6(4).10.1101/cshperspect.a 025163 PMC 481773826931460 · doi ↗ · pubmed ↗
- 7Sierra, F. The emergence of geroscience as an interdisciplinary approach to the enhancement of health span and life span. Cold Spring Harb Perspect Med. 2016; 6(4). 10.1101/cshperspect.a 02516310.1101/cshperspect.a 025163 PMC 481773826931460 · doi ↗ · pubmed ↗