TGCT of the shoulder – a case series and literature review
Josefa Stadelmeier, Filip Bijeljac, Alexander Klein, Felix Winden, Paul Reidler, Hans Roland Dürr

TL;DR
This case series and literature review explores the diagnosis and treatment of rare tenosynovial giant cell tumors in the shoulder, emphasizing the need for individualized treatment and follow-up.
Contribution
The study provides insights into the management of shoulder TGCT through a case series and comprehensive literature review, highlighting treatment outcomes and recurrence risks.
Findings
All patients except one were recurrence-free after treatment, with a mean follow-up of 39–233 months.
Diffuse TGCT was more common than nodular TGCT in the literature review, with a reported recurrence rate of 10.6%.
Arthroscopic and open resections were the primary treatments, with adjuvant therapies used in a minority of cases.
Abstract
Tenosynovial giant cell tumor (TGCT), also known as pigmented villonodular synovitis (PVNS), involving the shoulder is extremely rare and can present with a challenging clinical course. Due to the complex anatomy of the shoulder, both diagnosis and treatment are demanding. This study aims to evaluate the diagnostic and therapeutic management of shoulder TGCT based on a case series and a review of the literature. Between 2005 and 2021, four patients (2 females, 2 males) with shoulder TGCT (1 localized, 3 diffuse) underwent surgical treatment at our institution. The minimum follow-up was 39 months (range: 39–233 months). Functional outcomes were assessed using the Disabilities of the Arm, Shoulder and Hand Questionnaire (DASH), the Oxford Shoulder Score (OSS), and the Short Form 36 Health Survey (SF-36). Additionally, a literature review of 65 studies comprising 108 patients was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
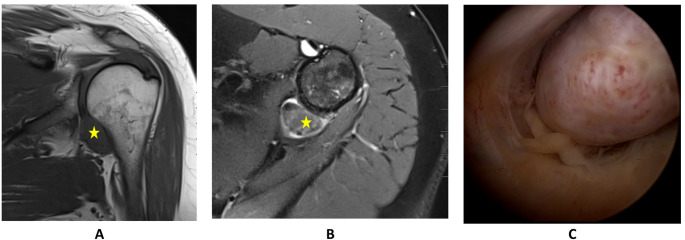 Figure 1
Figure 1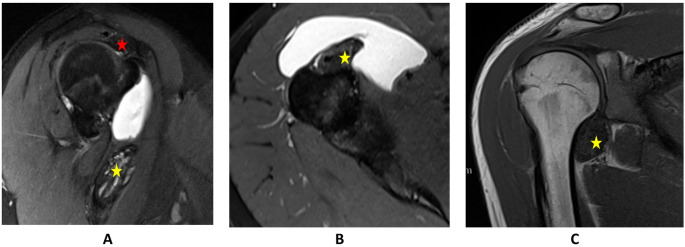 Figure 2
Figure 2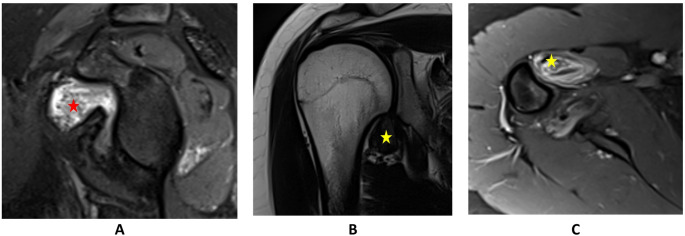 Figure 3
Figure 3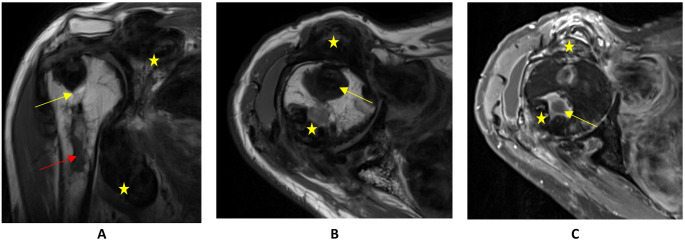 Figure 4
Figure 4- —Klinikum der Universität München (6933)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMusculoskeletal synovial abnormalities and treatments · Tendon Structure and Treatment · Elbow and Forearm Trauma Treatment
Introduction
Background
Tenosynovial giant cell tumor (TGCT), formerly known as Pigmented Villonodular Synovitis (PVNS), is a rare, benign proliferative disorder of the synovium, the tendon sheath and the bursa [1]. Typically, TGCT presents as a monoarticular process and predominantly affects the knee joint, hip, ankle, shoulder, elbow as hands and feet. Two types of TGCT are recognized: the nodular-type TGCT (N-TGCT) and the diffuse-type TGCT (D-TGCT) [2].
Epidemiology
Epidemiological data on TGCT are limited and varied, making comparisons challenging. In nationwide studies, the incidence rates of N-TGCT ranged around 11 to 34 per million. For D-TGCT, incidence rates were reported between 5 and 8.4 per million [3–5].
There is inconsistency in the data concerning the gender distribution of pigmented villonodular synovitis. While some studies indicate that males and females are affected at similar rates, others suggest a slight predisposition in females, specifically in cases of N-TGCT [3, 6]. TGCT predominantly presents between 35 and 50 years of age [5, 6].
Pathogenesis
The pathogenesis of TGCT remains unclear, with theories ranging from chronic inflammatory processes to neoplastic etiology [7, 8]. Last is at present the commonly accepted pathogenesis, hence the name was changed from PVNS to TGCT [9, 10].
The most frequently suggested associations include chronic recurring trauma, intra-articular hemorrhage, and persistent inflammation [11, 12]. West et al. hypothesized that a chromosomal translocation involving the 1p13 locus may contribute to the underlying pathogenesis [13]. Colony-stimulating factor-1 (CSF-1) overexpression promotes the formation of aberrant cellular aggregates, contributing to synovial soft tissue hyperplasia and thus defining the clinical and radiological disease [14].
Imaging and clinical presentation
TGCT is one of the few soft-tissue conditions with a nearly pathognomonic magnetic resonance imaging (MRI) appearance, characterized by synovial hypertrophy, low signal intensity and a “blooming artifact” [15–17]. This artifact, caused by iron in hemosiderin deposits, appears as notable signal loss on both T1- and T2-weighted MRI [18]. While N-TGCT presents most commonly with a painless swollen joint and MRI shows a well-circumscribed soft tissue mass [19], D-TGCT presents with a painful swollen joint, often with reduced mobility. On MRI an ill-defined soft-tissue mass is visualized [15]. In some cases impingement is the leading symptom [20].
Clinical, histological and molecular profile
Clinically, N-TGCT typically presents as a well-circumscribed, nodular mass causing painless swelling or mechanical symptoms (e.g., locking, impingement), with slow growth and low risk of local invasion. In contrast, D-TGCT manifests as an infiltrative synovial process with painful swelling, effusions, stiffness, and progressive joint destruction over time, often requiring repeated interventions if untreated. N-TGCT rarely progresses to diffuse form, while D-TGCT may extend intra- and extra-articularly [5].
N-TGCT typically shows mononuclear histiocyte-like cells, multinucleate giant cells, lymphocytes, and hemosiderin deposits, with moderate mitotic activity [15, 21]. D-TGCT displays a more infiltrative pattern with higher mitotic rates, a variable presence of giant cells, and occasional sarcoma-like features [22].
Molecularly, both forms are clonal neoplasms driven by CSF1 overexpression, often due to genomic rearrangements such as COL6A3::CSF1. This overexpression promotes tumor growth via paracrine recruitment of inflammatory cells and forms the basis for targeted therapy with CSF1R inhibitors [23–26].
Treatment strategies
In both N-TGCT and D-TGCT, the decision to pursue active treatment should carefully weigh the potential for cure against the typically benign nature of TGCT, its sometimes slow progression, the risk of local recurrence (LR) after complete resection, and the possibility of surgery-related complications [5]. Active surveillance should be considered as approach for asymptomatic patients [5].
The standard of care for symptomatic TGCT is surgical intervention, provided it can be performed with acceptable morbidity [5]. For N-TGCT, marginal excision is sufficient, whereas D-TGCT requires extensive synovectomy to achieve local disease control and optimize functional outcomes. Surgical access may be achieved via an open anterior approach or arthroscopically, depending on tumor extent and anatomical considerations [27]. In cases of extensive rotator cuff pathology or advanced joint destruction, rotator cuff repair or shoulder arthroplasty in combination with complete synovectomy may provide effective symptom relief and functional restoration.
Adjuvant therapies
Current evidence is insufficient to support radiotherapy as a standard treatment for TGCT in neoadjuvant, adjuvant, or recurrent settings. Radiation therapy can be in very selected cases an effective supplementary treatment, particularly where complete synovectomy is not feasible. It helps to prevent recurrences and preserves joint function with minimal toxicity [28, 29]. Other adjuvant therapies may include radiosynoviorthesis (RSO) and cryotherapy [30]. Both are at the moment considered as not beneficial.
Systemic treatment
In current trials, CSF1R pathway inhibitors such as Pexidartinib, Imatinib, Nilotinib, Vimseltinib, and monoclonal antibodies such as Emactuzumab have demonstrated effectiveness in TGCT, leading to significant tumor reduction, symptom relief, improved function, and sustained disease control [31–35]. Systemic treatment with CSF1R inhibitors may be considered when symptomatic TGCT cannot be surgically removed with acceptable morbidity and symptoms remain difficult to manage, particularly if disease progression is likely to impair quality of life (QoL) [5].
Study
In 1999, only 25 cases had been described in the English literature, managed by open synovectomy in all cases [36]. In 2017, Noailles et al. provided a literature review including 6 studies with 46 patients [36–42]. In this study, we present a series of four patients with TGCT of the shoulder, illustrating the heterogeneous clinical presentations, diagnostic challenges, and therapeutic outcomes associated with this rare entity. Additionally, we conducted a comprehensive review of the existing literature on shoulder TGCT, including 65 studies comprising 108 patients. Through the analysis of our cases and the available evidence, we aim to expand the limited knowledge on shoulder TGCT by providing insights into its clinical and radiological features, while underscoring the importance of timely diagnosis and appropriate management to optimize patient outcomes.
Materials and methods
Patient selection
Between March 2005 and May 2021, 4 patients (2 female, 2 male; mean age 38.8 ± 21.4 years) were diagnosed with TGCT of the shoulder—three with diffuse-type and one with localized-type (localized-type will be called nodular-type throughout the text). The right (dominant) shoulder was affected in three cases, the left in one. All patients underwent preoperative MRI and intraoperative histopathological confirmation by our Department of Pathology. Symptoms had been present for an average of 32.5 months (range: 12–60 months) before diagnosis. Surgical treatment was performed in all cases, including one rotator cuff repair. Two patients received adjuvant RSO. The mean follow-up period was 90 ± 95 months, with a minimum of 39 months. Patient characteristics are summarized in Table 1.
Table 1. Patient characteristics Patient No.Age/SexDuration of preoperative Symptoms (mo)TGCT typeTorn Rotator Cuff TendonAdjuvant therapyRecur-renceFollow-Up (mo) 1 54/f31nodularSSPnono40 2 24/f27diffuse-nono39 3 17/m12diffuse-RSOyes48 4 60/m60diffuse-RTstable disease233(abbreviations: f = female; m = male; mo = months; TGCT = Tenosynovial Giant Cell Tumor; SSP = Supraspinatus Tendon; RSO = radiosynoviorthesis; RT = Radiotherapy)
Surgical technique
Patients 1, 2, and 4 were positioned in a 30° beach-chair setup, while patient 3 was placed supine with the upper body elevated 30°; all underwent general anesthesia. The arm was positioned freely in all cases. Patient 1 initially underwent diagnostic shoulder arthroscopy with supraspinatus tendon repair and bony decompression, followed by open N-TGCT resection via the deltopectoral approach. Patients 2, 3, and 4 underwent primary open resections of D-TGCT using the deltopectoral approach. Patient 4 required a planned two-stage procedure; the second stage involved repositioning in left lateral decubitus and dual access via a medial scapular and subspinal incision.
Pathology
Tissue samples from synovial tissue were stained with hematoxylin and eosin, Elastica-van-Gieson (EvG) and iron stain and reviewed under a light microscope by a pathologist who specialized in musculoskeletal pathology.
Postoperative rehabilitation
Drains were removed within 1–3 days postoperatively. Patients 1–3 received interscalene plexus blocks for 4–5 days, after which all patients maintained adequate pain control according to WHO classification levels 1–2. Shoulders were immobilized in an arm sling for 4–6 weeks, with passive glenohumeral mobilization up to 60° in abduction and flexion. From week 4, assisted active movements up to 90° were introduced, excluding external rotation. Beginning in week 7, exercises were progressively intensified beyond 90°, with rotation as tolerated. The goal was full shoulder mobility by 12 weeks, with return to sports permitted no earlier than week 12.
In the 1st year, MRI follow-up checks were carried out every 3 months, every 6 months in the 2nd year, then annually for 5 years.
Outcome instruments
The patient related outcome measures (PROMs) of this study included the Disabilities of Arm, Shoulder and Hand Questionnaire (DASH), the Oxford-Shoulder-Score (OSS) and the Short Form 36 Health Survey (SF-36). The total DASH score ranges from 0 to 100, where a score of 0 indicates an excellent functional outcome. The OSS ranges from 0 to 48, with a score of 48 representing the optimal functional outcome. The SF-36 health survey scores range from 0 to 100, where a score of 100 reflects excellent health and the highest quality of life. These PROMs were collected postoperatively at the time of the last follow-up. The rest of the data were retrieved from the patients’ medical records.
Literature search strategy and selection criteria
A comprehensive literature search was conducted to identify all published studies reporting on TGCT of the shoulder. The search was performed using PubMed, google scholar, Web of Science from their inception to 15.02.2025. The following search terms were used in combination with Boolean operators: “tenosynovial giant cell tumor” OR “TGCT” OR “pigmented villonodular synovitis” OR “PVNS” OR ″giant cell tumor of the tendon sheath″ AND “shoulder”.
Inclusion criteria were: (1) studies reporting on TGCT of the shoulder; (2) clinical studies, case series, or case reports; (3) abstracts published in English. Exclusion criteria included: (1) studies focusing on TGCT of other joints without specific mention of the shoulder; (2) review articles without original patient data.
Titles and abstracts were screened by 2 independent reviewers, followed by a full-text assessment for eligibility. Any disagreements were resolved by consensus or consultation with a third reviewer. References of included articles were manually screened to identify additional relevant studies.
Statistical analytic tools
Analysis was performed with Microsoft Excel 2016. No statistical hypothesis tests were performed due to the small sample size (n = 4). Results are presented descriptively using means ± standard deviations, ranges, and confidence intervals where appropriate to characterize the patient cohort and outcomes.
Results
Case 1
A 54-year-old female presented with a 2-year and 7-month history of progressive, movement-dependent left shoulder pain and restricted mobility without prior trauma. The pain was exacerbated by activity and present at rest and during the night. Conservative treatment, including physiotherapy and a corticosteroid injection, was ineffective.
MRI revealed a solid intra-articular mass with hemosiderin deposits in the shoulder recess, suggestive of TGCT (Fig. 1), along with AC joint osteoarthritis, a supraspinatus tendon tear with footprint cyst formation, and early degenerative changes of the glenohumeral joint. Clinically, TGCT appeared asymptomatic, with the symptoms attributed primarily to the rotator cuff pathology. Examination showed tenderness over the AC joint, subacromial space, and bicipital groove. Active range of motion included 160° flexion, 100° abduction, internal rotation to L2, and 30° external rotation. Impingement signs and supraspinatus and AC joint tests were positive.
Arthroscopy revealed articular-sided partial rupture of the SSP (Ellman III), SLAP I lesion, subacromial bursitis, acromioclavicular joint arthrosis, bony subacromial impingement, and a cherry-sized nodular lesion in the lower recess (Fig. 1). Arthroscopic synovectomy, SLAP debridement, subacromial bursectomy, lateral clavicle resection, supraspinatus tendon repair using a SpeedScrew anchor (Smith & Nephew GmbH, Hamburg, Germany) and bony subacromial decompression were performed. In open surgery, the pedunculated, dorsally luxated N-TGCT was removed in total. Histopathology confirmed TGCT. Three years and four months postoperatively, the patient remained free of recurrence with excellent functional outcome and full range of motion (PROMs in Tables 2 and 3).
Fig. 1MRI scans and arthroscopic images of TGCT of the shoulder in patient 1. A: T1w coronal view of the left shoulder, depicting a mass in the lower recess. B: T2w axial view of the left shoulder, depicting a mass in the dorsal lower recess. C: Arthroscopic view of a mass in the dorsal lower recess of the left shoulder
Case 2
A 24-year-old female patient reported right shoulder pain for two years and three months, treated conservatively. The pain was intermittent and worsened with specific movements. For two months, she noticed a lump in the upper arm accompanied by increased pain, which later subsided. Further diagnostic workup, including MRI was initiated. A diagnosis of diffuse TGCT involving the long biceps tendon and anterior shoulder joint was confirmed (Fig. 2).
She underwent marginal resection of the TGCT lesion. The patient was positioned in a beach chair position with a deltopectoral surgical approach. Intraoperative findings included extensive TGCT masses along the long head of the biceps tendon, requiring transection and refixation of the subscapularis tendon. A solid TGCT lesion caudally was also noted, pedunculated and attached to the capsule. Histopathology confirmed TGCT.
Three years and three months postoperatively, the patient remained free of recurrence with excellent functional outcome (PROMs in Tables 2 and 3).
Fig. 2MRI scans of TGCT of the shoulder in patient 2. A: sagittal PD tse fs TE 47 of the right shoulder; B: axial PD tse fs TE 47 of the right shoulder; C: coronal T1 TSE of the right shoulder; The star marks the masses of TGCT around the bicpes tendon (yellow) and subacromial (red)
Case 3
An 18-year-old male presented with progressive, atraumatic right shoulder pain over one year, localized intra-articularly and radiating to the proximal humerus. The discomfort was described as intra-articular, radiating to the proximal humerus, and unrelated to mechanical load. MRI revealed a suspected TGCT in the inferior recess and below the coracoid process (Fig. 3). Open synovectomy via a deltopectoral approach confirmed TGCT histologically. Postoperative recovery was initially uneventful.
Seven months postoperatively, MRI revealed a LR, necessitating a repeat open synovectomy and subsequent RSO. Despite initially unremarkable follow-up imaging, progressive lesion growth was noted 1.5 years later. The patient was clinically symptom-free. A third surgical intervention—arthroscopic total synovectomy—was performed three years after the initial recurrence, revealing extensive brownish synovitis and mild cartilage damage (grades I–II). The arthroscope was also repositioned ventrally in order to achieve a dorsal synovectomy of the lower recess. Histopathology again confirmed TGCT.
Postoperative care included free mobilization and a second RSO. The patient remained symptom-free with no radiological evidence of recurrence at one-year follow-up. One year later, there was no evidence of recurrence (PROMs in Tables 2 and 3).
Fig. 3MRI scans of TGCT of the shoulder in patient 3. A: PDFS sagittal of the right shoulder: red star marks the mass below the coracoid. B: T2 coronal of the right shoulder: yellow star marks the mass in the lower recess. C: T1FS axial view of the right shoulder: yellow star marks the mass in the lower recess
Case 4
A 61-year-old male patient experienced right shoulder pain for at least six years, progressively worsening over the past six months. Imaging, including X-rays and MRI, revealed extensive TGCT extending into the thoracic wall, involving the humeral shaft with intraosseous components, and encasing neurovascular structures without infiltration (Fig. 4).
The patient underwent open anterior synovectomy, tumor resection, and intraosseous curettage. This patient showed very pronounced TGCT findings: a large tumor extending subscapularly, a broad infiltration of the dorsal joint space extending far distally along the humerus. In addition, there was an extensive infiltration of the long head of the biceps tendon on the ventral side, destroyed to such an extent that it tore when pulled with a finger. Besides, the TGCT infiltrated the proximal medullary cavity in the bicipital sulcus. Here, the window was opened with the Luer and extensively curetted. Ultimately, the lesions could be completely removed ventrally, but there were still tumor parts in the area of the subscapularis muscle and the dorsal humerus, which were then removed in a planned second surgery six weeks later. Histopathology confirmed TGCT.
Postoperative care included immobilization in a Gilchrist brace for four weeks, and limited shoulder movement. Postoperative radiation therapy followed due to remaining tumor tissue.
MRI surveillance continued at regular intervals, revealed stable disease without significant progression over subsequent years. 19 years and 5 months after the initial diagnosis, the patient maintained functional mobility with mild restrictions (PROMs in Tables 2 and 3).
Fig. 4MRI scans of TGCT of the shoulder in patient 4. A: T1 TSE coronal: cystic components (marked by a yellow arrow). Destruction of the humeral head and erosions in the subcapital humeral shaft (marked by a red arrow). The lesions extend subacromial and to the medial thoracic wall (exemplified by yellow stars). B: T1 TSE axial: hypointense nodular structures (exemplified by yellow stars) with individual cystic components (marked by a yellow arrow). C: T1 TSE axial with contrast fluid: hypointense nodular structures (exemplified by yellow stars) with individual cystic components (marked by a yellow arrow) with increased absorption of contrast medium
Outcome of DASH, OSS and SF-36
All scores for each patient and means are shown in Tables 2 and 3.
Table 2. Individual Oxford-Shoulder-Score (OSS) and Score of the Disabilities of Arm, Shoulder and Hand Questionnaire (DASH), including mean and standard deviation (SD) for the patient collective at a median follow-up of 44 months (range 39–233 months)Patient no.OSSDASHDASH Sport/InstrumentSport / InstrumentDASH WorkWork 1 470,830Volleyball/ piano0Art teacher 2 4800Running, biking0Desk activity 3 470,8325Strength training0Computer scientist 4 4121,6712,5Senior gymnastics-Pensioner Mean 45,755,839,380,00 SD 3,2010,5711,970,00
Table 3. Individual scores of the Short Form 36 Health Survey (SF-36), including mean and standard deviation (SD) for the patient collective at a median follow-up of 44 months (range 39–233 months)Patient no.Physical FunctioningRole limitations due to physical healthRole limitations due to emotional problemsEnergy/fatigueEmotional well-beingSocial functioningPainGeneral health 1 8000304088035 2 1001001008096100100100 3 9510010080881009040 4 551001005088757860 Mean 82,5075,0075,0060,0078,0090,7567,0058,75 SD 20,2150,0050,0024,4925,6111,9345,5629,55
Pathologic findings
Macroscopically, the excised tissues were variably orange-brown and gray-glassy.
Patient 1 (N-TGCT) showed a nodular lesion with oval nuclei, scattered disorganized giant cells, and hemosiderin-loaded macrophages, without atypia or necrosis.
Patients 2–4 (D-TGCT) demonstrated cell-rich synovial tissue with irregular giant cells, foam cells, hemosiderin deposits, and signs of old hemorrhage. Focal necrosis and marked bleeding were present, but no cellular atypia was observed.
Literature review
Shoulder TGCT is an exceptionally rare condition, with a total of 107 cases identified in the literature, including the four patients presented in this study. The sex distribution was nearly balanced, with a slight predominance of female patients (46.7%) over male patients (36.4%). The mean age at diagnosis was 50.3 ± 19.7 years, ranging from 5 to 84 years. The average duration of symptoms prior to diagnosis was 23.6 ± 28.1 months. TGCT subtype was specified in only 65 cases, of which 33.8% were classified as N-TGCT and 66.1% as D-TGCT. The affected side was reported in 58 cases and the left shoulder was affected in 34.5% of cases, the right shoulder in 58.6%, and bilateral involvement was reported in 6.9%. A concomitant rotator cuff tear was documented in 32.4% of patients, while bone involvement was reported in 30.6% of cases.
Surgical details were available for 77 cases: 42.9% underwent open surgery, 53.2% arthroscopic surgery, and 3.9% a combined approach. Rotator cuff repair was performed in 20.8% of cases, and rotator cuff debridement in 2.7%. Shoulder arthroplasty was performed in 12 cases (15.6% of surgical cases), including four hemiarthroplasties (HA), six reverse total shoulder arthroplasties (rTSA) (one of the rTSAs in a case of recurrence), one anatomic total shoulder arthroplasty (aTSA), and two cases where the type of prosthesis was not specified.
Adjuvant therapy was administered in 9.3% of cases (n = 10), including RSO in one patient (0.9%), radiotherapy in eight patients (7.5%), and osmium acid therapy in one patient (0.9%). The mean follow-up duration was 37.6 ± 36.2 months (range 6–233 months) in 67 cases. In those 44.8% were D-TGCT, 19.4% were N-TGCT and in 35.8% type of TGCT was not mentioned. In those 67 cases LR was reported in 10.6% (n = 7) and residual disease in 4.5% (n = 3). All reported recurrences and residual diseases were classifed as D-TGCT. Details of the literature review are depicted in Table 4.
Table 4. Results of the literature review of TGCT of the shouldersourcenumber of patientssexageduration of symptoms in monthsnodular /diffuseaffected siderotator cuff tearbony involvementtype of surgerycuff-repairtype of APadjuvant therapyfollow-up time (months)recurrencetreatment of recurrenceresidual lesionAgrawal et al. [59]1m384dryesopen8yesRSOyes Broski et al. [60]1f46lByers et al. [55]1dopenCheng et al. [52]1m2036nopenChiang et al. [41]]5fyesAS22,4nofyesAS22,4nomyesAS22,4nomyesAS22,4nomyesAS22,4noCho et al. [61]1m213rAS + open18noColak et al. [62]1f49Costallat et al. [63]1f1512rAS9noCotten et al. [64]1m528dopenDias et al. [65]1f591nlopen24noDkhissi et al. [66]1m6836dyesopen6yesDorwart et al. [43]2f6548dyesyesyes114yesrTSAm569dyesopenrTSA Du et al. [67]1f12dlopenElumogo et al. [68]1m65chroniclFlandry and Norwood [69]1m28dopen24noGanel et al. [70]2f749dyesyesopen36nom798dyesyesopen24noGiannatos et al. [44]1f5024lAS12noGolge et al. [54]1m75chronicyesyesopenrTSAGraf et al. [71]1f80dbyesASyesGumina et al. [40]9f65,812ryesASyes27f65,812ryesASyes27f65,812ryesASyes27f65,812ryesASyes27f65,812ryesASyes27f65,812ryesASyes27m65,812ryesASyes27m65,812lyesASyes27m65,812lyesASyes27Ji et al. [51]2f6636dryesyesASyesRT24nof71120dryesyesASyes36noJohansson et al. [42]43572dyesrTSA24no3572dyesrTSA24no3524n3512dyes180noKho et al. [39]1644byesASKonrath et al. [72]1m4136dyesopen48noKwon et al. [73]1f716dryesopenHSA7no Lee, K. et al. [74]1f270nlAS12noLee, S.-J. et al. [75]1m64dbyesyesASLee, M. et al. [76]1f40dlyesopen43noLevin and Gannon [77]2f792dopenf216dyesopenLewis et al. [78]1m580nrLi et al. [27]6f45n/dryesAS92yes2 x AS (progress from N-TGCT to D-TGCT)f30nlASRT62nof65nryesAS44nof62nryesAS40nof38nrAS28nom64nryesAS46no Liang et al. [79]1rLoh et al. [80]1m466nrAS + open9noMahieu et al. [38]2f3096nlyesAS96nof5336dryesyesASosmium acid24noMankin et al. [81]]4Mazabraud et al. [82]4yesyes Mazabraud et al. [82]1f17dr (mf)conservativeRT14residualyesMulier et al. [84]1m6412dyesyesyes6noMuller et al. [36]1m164nlyesopenPalmerini et al. [85]2openAPopenAPPantazopoulos et al. [53]1m36dyesopenPark et al. [49]129dyesyesopenHSA24noPereira et al. [20]1f1524nrAS12noPetsatodis et al. [48]2f6012dropenHSA48nom636dlopenHSA60noPopov et al. [86]1f63120dlyesopenRT12noRajakulasingam et al. [87]1f60nRezaee, A. et al. [88]1m59nSawmiller et al. [89]1f5712yesyes21noSayegh et al. [90]1f3420dlASSchwartz et al. [56]2m5536nopenm5890dyesopenrTSASeiler et al. [91]1m5560Selby et al. [92]1m58nropen60noSerra et al. [29]1m748dyesyesASRTSher et al. [93]1f18nyesSimmer et al.[94]1f582nlAS53noSipahioğlu et al. [95]1m2324dAS36noSnook [96]2f8212dyesopenRT18yesyesf841dyesconservativeRT24residualyesSotje et al. [97]1m5nStadelmeier et al. 4f5431nlyesAS + openyes40nof2427dropen39nom1712dropenRSO48yesopen, AS, RSOm6060dryesopenRT233residualyesTang et al. [98]1f74dr36yesTong et al. [99]1m516dyesToro et al. [50]1m396dlyesopenaTSA48noVj et al. [46]6f42lAS36nof38rAS36nom74rAS36nof63lAS36nof60rAS36nom27rAS36noZhao et al. [100]1f76db (mf)yesconservativeyes(Abbreviations: m = male; f = female; n = nodular; d = diffuse; l = left; r = right; b = both shoulders; mf = multifocal; AS = arthroscopy; HSA = hemi shoulder arthroplasty; AP = arthroplasty (not specified); rTSA = reverse total shoulder arthroplasty; aTSA = anatomic total shoulder arthroplasty; RSO = radiosynoviorthesis; RT = radiotherapy)
.
Discussion
Main findings
This case series demonstrates that shoulder TGCT can be effectively managed with arthroscopic and open synovectomy combined with rotator cuff repair, achieving excellent long-term functional outcomes and quality of life. All patients maintained adequate pain control and returned to work or sports. Even the patient with most extensive intraosseous involvement showed disease stability over 10 years without revision surgery, highlighting the feasibility of conservative management after initial resection.
Epidemiology
With a mean age of 38.8 ± 21.4 years (range 17–60 years) at their initial presentation, patients in this study fit well compared to other studies. It is suggested that the incidence peak is between 30 and 50 years of age [43]. Other literature reviews even suggest 50–80 years [44]. So far, only two case reports mentioned TGCT in the shoulders of adolescents [36, 45]. Females and males are equally affected [43].
Diagnosis
In this case series, the mean duration from symptom onset to diagnosis was 32.5 ± 17.4 months, compared to 23.6 ± 28.4 months in the literature, highlighting a significant diagnostic delay in TGCT. This delay often results in advanced joint involvement, with approximately one-third of patients already exhibiting bone erosions due to synovial inflammation, mechanical stress from the lesion, or massive rotator cuff tears [41]. Despite this, the majority of the patients achieve symptom resolution after arthroscopic or open surgery [41, 43]. TGCT should be considered in young patients with unexplained shoulder pain and MRI findings suggestive of neoplastic disease [36, 37].
Functional outcomes post-surgical intervention
There is limited literature on PROMs after TGCT surgery of the shoulder. VJ et al. reported on six patients undergoing arthroscopic synovectomy, showing significant improvements: Constant score from 64.8 to 94.5, American Shoulder and Elbow Surgeons (ASES) score from 81.2 to 99.7, and University of California, Los Angeles (UCLA) score from 23.2 to 34.8 at ≥ 36 months follow-up [46].
Quality of life post-surgical intervention
According to our literature research this is the first study reporting quality of life results for patients with TGCT of the shoulder. Most patients reported outcomes equal to or exceeding the sex- and age-adjusted normative data for the German population [47]. Patient 1 developed severe rheumatoid arthritis, which likely accounts for the self-reported impairment in quality of life, despite demonstrating excellent functional outcomes for the shoulder. Patient 4 reported diminished physical functioning (Score = 50) compared to the age- and sex-adjusted German normative data (Mean Score = 76.4; 95%-CI = 73.7–79.1). This reduction may be attributable to his limited shoulder mobility. Patient 3 reported significantly worse general health (Score = 40) relative to the German normative population (Mean Score = 75.3; 95%-CI = 73.7–77.0). As the youngest participant in this study, the impact of impaired functionality may be more pronounced, particularly due to the inability to engage in sports and strength training, as reflected by a DASH sport/instrument score of 25. Furthermore, the most recent revision surgery occurred only 10 months prior to the assessment, suggesting potential for further improvement in personal strength and overall functional outcomes.
Treatment – open surgery or arthroscopy?
There are no standardized guidelines for choosing between open and arthroscopic surgery in the management of shoulder TGCT. Both approaches yield good outcomes. Open synovectomy may be necessary for complete resection, especially in D-TGCT [42], while arthroscopic resection can also be effective if total synovectomy is achieved [39].
Arthroscopy offers the advantage of joint-wide visualization and lower morbidity and may be preferable when diagnosis is uncertain [27, 38]. In this series, one patient was successfully treated arthroscopically for re-recurrence. Alternating between open and arthroscopic techniques may help in recurrent cases.
Expert consensus by Stacchiotti et al. recommends macroscopic complete resection for all TGCT types, with arthroscopic or open approaches chosen, based on disease extent. D-TGCT has a high risk of local recurrence and should be discussed in a multidisciplinary tumor board. Extra-articular D-TGCT may require marginal resection through extended incisions due to soft tissue involvement [5].
What to do with rotator cuff tear?
In cases involving the shoulder, a thorough evaluation of the rotator cuff and articular surfaces is essential, as these factors play a critical role in determining clinical outcomes. Rotator cuff tears associated with shoulder TGCT are typically classified as massive, and degenerative changes in the articular surfaces are consistently observed to varying degrees. Consequently, in addition to synovectomy, the following surgical interventions are recommended if needed [40]: arthroscopic debridement and of the cuff tear [39, 41], partial cuff repair [41], HA [48, 49], and TSA [50].
Jong-Hun Ji et al. and Li et al. reported favorable clinical outcomes following arthroscopic or open synovectomy combined with rotator cuff repair, highlighting the therapeutic benefit of early intervention [27, 51]. Notably, Gumina et al. found that patients with D-TGCT who underwent arthroscopic synovectomy and subacromial debridement had significantly worse clinical outcomes compared to a control group without synovitis or osteoarthritis (arthroscopic debridement for irreparable rotator cuff tear alone). These poorer results were attributed to secondary osteoarthritis caused by unrecognized or late-treated TGCT [40]. Importantly, in cases where TGCT was identified early and treated with combined synovectomy and rotator cuff repair, outcomes were satisfactory, and no osteoarthritic changes were observed at follow-up.
Severe joint destruction and arthroplasty
TGCT of the shoulder can lead to severe joint destruction, often presenting with polycystic changes in the humeral head [52]. Elevated intra-articular pressure contributes to localized bone resorption and cyst formation, which may be further invaded by hypertrophic synovium via cortical breaches, the chondro-osseous junction, or vascular foramina [36, 48, 53]. As the villonodular tissue expands, progressive intraosseous infiltration may occur.
In advanced cases with substantial joint degeneration, various forms of shoulder arthroplasty—including HA, aTSA, and rTSA—have shown favorable outcomes [48, 50, 54]. Case reports demonstrate that these procedures effectively relieve pain, restore joint function, and reduce recurrence risk by enabling more complete dorsal synovectomy after osteotomy of the humeral head [5, 50]. The choice of prosthesis should be guided by the extent of osseous destruction and the presence of rotator cuff pathology. Specifically, rTSA may be advantageous in patients with concomitant rotator cuff tears, while aTSA or HA are appropriate in cases with preserved cuff integrity [42, 43]. Current evidence supports arthroplasty as a viable treatment option in patients with TGCT of the shoulder and advanced joint damage, particularly in elderly individuals with degenerative changes [36, 50].
Adjuvant therapies
Percutaneous radiotherapy can offer some relief of the symptoms and it can be beneficial as adjuvant treatment after surgical resection for residual lesions [28, 29]. However, due to the young age of most patients, it is rarely a primary alternative. For inoperable cases, systemic therapy is preferable, while surgical management with complete macroscopic resection remains the treatment of choice for D-TGCT, and early marginal excision is recommended for the nodular form [5].
Given that patients with TGCT are typically young, and the disease is non-life-threatening, long-term complications such as malignant transformation, fibrosis, joint stiffness, and other sequelae are of particular concern. The use of radiotherapy in selected cases lacking viable alternative treatment options remains a subject of ongoing debate [5].
Radiosynoviorthesis has not demonstrated efficacy in the management of D-TGCT and should not be employed as a substitute for incomplete surgical resection. Prospective studies are warranted to better define its potential therapeutic role in the treatment of TGCT [5].
Recurrence
Reported LR rates of TGCT after treatment vary widely between 9% and 55%, influenced by nodular or diffuse disease, joint location and follow-up duration [55–57]. Most of the recurrencies are seen in the first 2 years after surgery. Recurrence in the shoulder is rarely reported, likely due to the overall low incidence of TGCT at this site [50]. In this literature review, the LR rate for shoulder TGCT was 10.6% (n = 7) and the rate for residual disease was 4.5% (n = 3) at a mean follow-up of 37.6 ± 36.2 months (range 6–233 months).
D-TGCT has a higher recurrence risk than the localized form, though data specific to the shoulder are limited [57]. Key risk factors include incomplete surgical resection, particularly with extra-articular or intraosseous involvement, as well as delayed diagnosis and long symptom duration. These factors contribute to more extensive synovial disease and increase the likelihood of residual tumor and recurrence. Moreover, revision surgery in recurrent TGCT cases carries a substantially elevated risk of further recurrence [5]. Careful preoperative MRI evaluation is essential to detect occult or discontinuously growing lesions that may be missed during standard surgical approaches [58].
The main limitation of this study is the small sample size, which is inherent to the rarity of TGCT of the shoulder. Nevertheless, the extended follow-up duration and the inclusion of both functional and quality‑of‑life outcome measures enhance the clinical relevance of the presented findings. Despite these limitations, the present series contributes one of the longest follow-up periods and most comprehensive functional assessments reported to date for this rare entity, thereby expanding the current evidence base. These observations permit cautious but meaningful conclusions regarding the management of shoulder TGCT and underscore the importance of individualized treatment planning and vigilant follow‑up.
Conclusion
TGCT of the shoulder is a rare condition that requires an individualized and multidisciplinary approach. Both arthroscopic and open synovectomy can achieve favorable outcomes when complete resection is accomplished. Given the risk of recurrence, structured long-term follow-up remains essential. To further refine treatment algorithms and identify prognostic factors specific to shoulder TGCT, larger multicenter or registry-based studies with standardized outcome reporting are needed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Stephan SR, Shallop B, Lackman R, Kim TWB, Mulcahey MK (2016) Pigmented Villonodular Synovitis: A Comprehensive Review and Proposed Treatment Algorithm. JBJS Rev 4(7). 10.2106/JBJS.RVW.15.0008610.2106/JBJS.RVW.15.0008627509331 · doi ↗ · pubmed ↗
- 2Falster C, Stockmann Poulsen S, Joergensen U (2017) A rare case of localised pigmented villonodular synovitis in the knee of a 24-year-old female soccer player: diagnosis, management and summary of tenosynovial giant cell tumours. BMJ Case Rep 2017(bcr–2017–219549). 10.1136/bcr-2017-21954910.1136/bcr-2017-219549 PMC 565236128978573 · doi ↗ · pubmed ↗
- 3Schwartz HS, Unni KK, Pritchard DJ (1989) Pigmented villonodular synovitis. A retrospective review of affected large joints. Clin Orthop Relat Res 247:243–2552791393 · pubmed ↗
- 4Cho CH, Sohn SW, Song KS, Kang CH, Min BW, Bae KC et al (2008) Extra-articular pigmented villonodular synovitis of the subacromial space. Orthopedics 31(12). 10.3928/01477447-20081201-0410.3928/01477447-20081201-0419226060 · doi ↗ · pubmed ↗
- 5Sawmiller CJ, Turowski GA, Sterling AP, Dudrick SJ (1997) Extraarticular pigmented villonodular synovitis of the shoulder: a case report. Clin Orthop Relat Res. 335:262–2679020227 · pubmed ↗
- 6Tang K, Zheng X, Lin J, Wang L (2019) Diffuse-type tenosynovial giant cell tumor of the shoulder evaluated by FDG PET/CT. Clin Nucl Med 44(4):310–31210.1097/RLU.000000000000245130624274 · doi ↗ · pubmed ↗