Deep brain stimulation and magnetic resonance–guided focused ultrasound for essential tremor: a meta-analysis of effectiveness and safety
Haneen Sabet, Abdallah Abbas, Esraa Y. Salama, Abrar AbuHamdia, Mohamed El-Moslemani, Majed Aldehri, Ibrahim Alnaami

TL;DR
This study compares deep brain stimulation and focused ultrasound for treating essential tremor, finding that deep brain stimulation may be more effective but both have different safety profiles.
Contribution
The study provides a meta-analysis comparing the effectiveness and safety of DBS and MRgFUS for essential tremor, highlighting differences in outcomes and adverse events.
Findings
DBS showed greater improvement in total Clinical Rating Scale for Tremor scores compared to MRgFUS.
MRgFUS was associated with more frequent sensory and motor adverse events like paresthesia and gait instability.
Both treatments had similar response rates, but DBS had more serious but rare complications like infection and hemorrhage.
Abstract
We compared the effectiveness and safety of deep brain stimulation (DBS) and magnetic resonance-guided focused ultrasound (MRgFUS) in patients with essential tremor (ET). A comprehensive search was conducted across four databases (Web of Science, Scopus, PubMed, and Cochrane CENTRAL) till June 2025. Clinical trials and observational studies comparing DBS and MRgFUS in patients with ET were included. Meta-analysis was performed using RevMan version 5.4 and OpenMetaAnalyst, applying a random-effect model. Five cohort studies (463 patients) were included. In the total Clinical Rating Scale for Tremor (CRST) score, there was a significant difference between the two groups favoring DBS (mean difference (MD): 5.12, 95% confidence interval (CI): [1.08, 9.16], P = 0.01), while in part A of the CRST, there was no significant difference (P = 0.15). No significant difference was found between the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
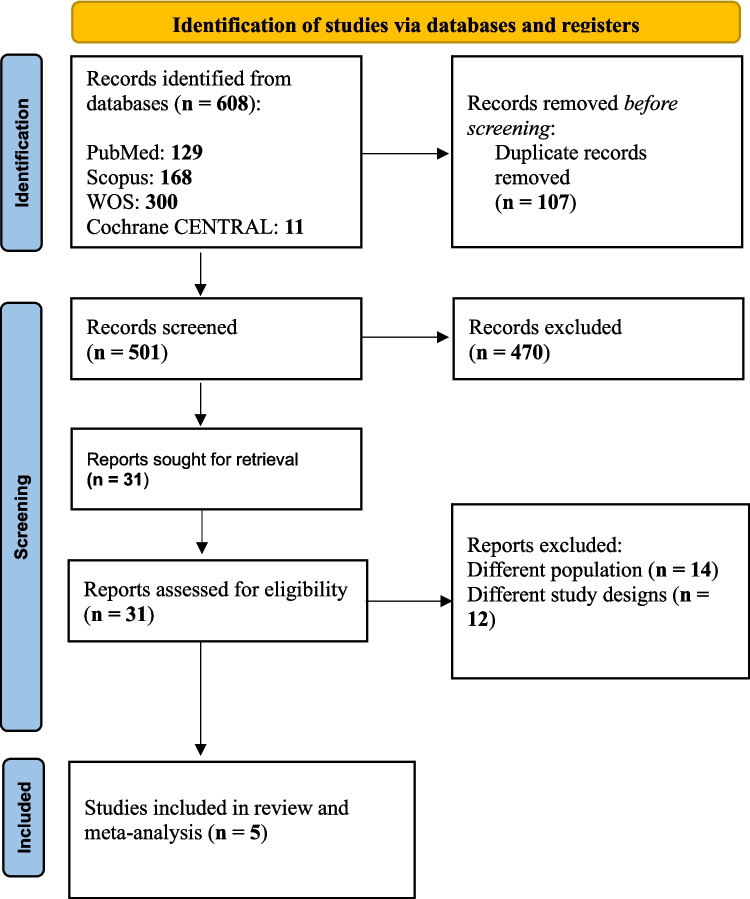 Figure 1
Figure 1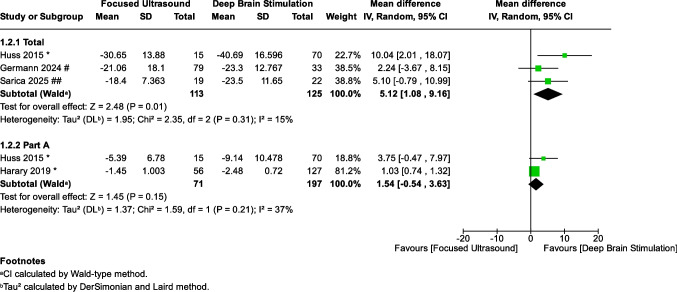 Figure 2
Figure 2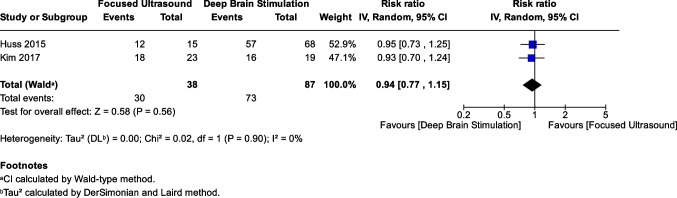 Figure 3
Figure 3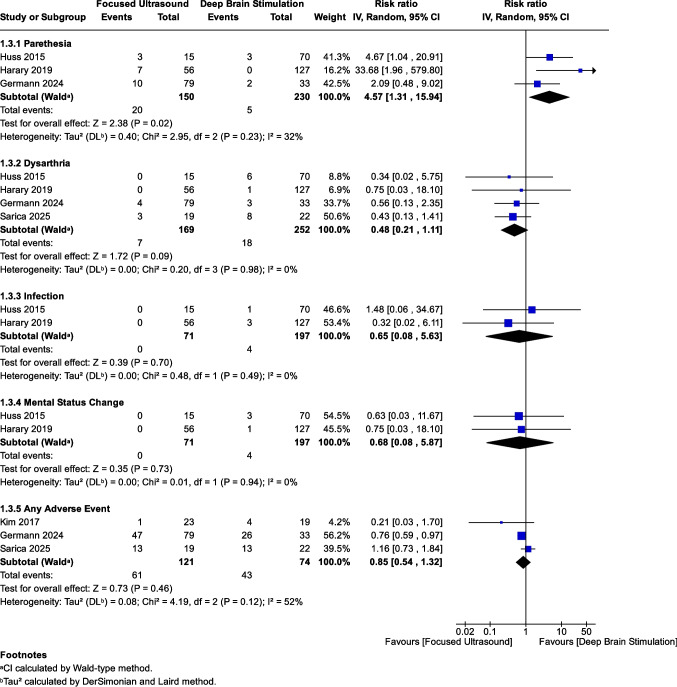 Figure 4
Figure 4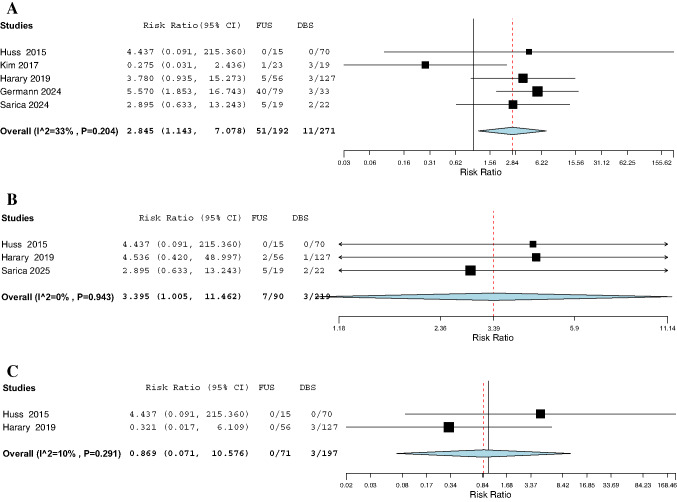 Figure 5
Figure 5- —Al-Azhar University
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeurological disorders and treatments · Vagus Nerve Stimulation Research · Botulinum Toxin and Related Neurological Disorders
Introduction
Essential tremor (ET) is the most prevalent movement disorder, affecting approximately 3.2 individuals per 1,000 globally. Characterized primarily by an isolated upper limb action tremor persisting for at least three years, ET may also present with tremors in other regions [1]. Management strategies for ET primarily involve pharmacological and surgical interventions. Propranolol is the only U.S. Food and Drug Administration (FDA)-approved medication for ET. For patients resistant to medical management, surgical options are often required [1].
Deep brain stimulation (DBS) is a well-established, reversible method to alleviate ET through targeted electrical stimulation of the ventral intermediate nucleus (Vim) of the thalamus. While DBS offered substantial benefits, including adjustable stimulation, it requires invasive procedures and the implantation of hardware [2–5]. Conversely, magnetic resonance-guided focused ultrasound (MRgFUS) has emerged as a non-invasive alternative. It leverages focused ultrasound (FUS) energy to create precise lesions in the brain without incisions [6]. This technique combines the accuracy of real-time magnetic resonance imaging (MRI) with the therapeutic effects of ultrasound and has been recently approved for the treatment of ET [5, 7–9].
Despite the distinct mechanisms of these two modalities, current literature suggests comparable effectiveness and safety, yet a systematic review and meta-analysis that thoroughly examines and directly compares these studies is lacking. This creates a critical knowledge gap regarding the optimal surgical choice for medication-refractory patients. This systematic review and meta-analysis aim to fill this gap by rigorously comparing the effectiveness and safety of DBS and MRgFUS in treating patients with ET.
Methods
This study followed the guidelines outlined in the Cochrane Handbook for Systematic Reviews of Interventions, the PRISMA statement [10, 11], and the MOOSE guidelines for meta-analyses of observational studies [12]. The protocol was registered in the PROSPERO (CRD420251158889).
Search & eligibility criteria
We searched four databases—Web of Science, Scopus, PubMed, and Cochrane CENTRAL—from their inception until June 2025. The search query used was:
(("Deep brain stimulation" OR DBS) AND ("Focused ultrasound" OR FUS)) AND ("Essential tremor" OR "Essential tremors" OR "Kinetic tremor" OR "Kinetic tremors" OR "Familial tremor" OR "Familial tremors"). For the detailed search strategy across each database, refer to Supplementary Table 1.
We included all clinical trials and observational studies (both retrospective and prospective) that compared two groups—one receiving DBS and the other FUS—in patients with ET. The studies had to aim at evaluating the efficacy and safety of these two treatment modalities. There was no language restriction.
We excluded studies with different designs (case series, abstracts, animal studies, reviews, and case reports), as well as studies involving different populations (e.g., patients with PD), single-arm studies, or studies with outcomes unrelated to effectiveness or safety.
Screening & data extraction
The screening process was conducted in two steps: first by reviewing titles and abstracts, followed by full-text screening. Two independent and blinded authors carried out the process using the Rayyan tool [13].
We applied the same approach for data extraction. A spreadsheet was used to collect the following information: summary data, baseline data, and outcomes. The summary data included study design, recruitment duration, follow-up period, country, details of FUS and DBS (whether unilateral or bilateral, target, and imaging modality), inclusion criteria, and a general summary of the study. Baseline data included the sample size (number of patients), age (in years, mean and standard deviation [SD]), sex (number of males and females), disease duration (in years, mean and SD), baseline Clinical Rating Scale for Tremor [CRST] score (mean and SD), and baseline quality of life in essential tremor questionnaire [QUEST] score (mean and SD).
Outcome data included the response rate, CRST scores, and adverse events (AEs). The response rate was defined differently in two studies. In Kim et al. (2017), it was defined as complete tremor remission after surgery or a reduction in tremor greater than 90% [14]. In Huss et al. (2015), it was defined as a reduction in dominant hand action or intention tremor on the CRST score from a rating of 2 to 4 to a rating of 0 to 1 [15].
The CRST included Part A and the total score. The CRST is a tool used to assess the severity of tremor symptoms and their impact on daily life [16]. It consists of three parts. Part A assesses tremor severity at rest, in posture, and during movement (intention tremor). Part B evaluates how tremor affects motor tasks such as writing, drawing, and pouring water. Part C assesses the functional impact of tremor on daily activities such as eating, dressing, and using utensils. Each item on the scale is typically scored from 0 to 4, with 0 indicating no tremor and higher scores reflecting more severe symptoms. The total CRST score is the sum of all three parts, with higher scores indicating greater severity and functional impairment.
Bias risk assessment
We used the Newcastle–Ottawa Scale (NOS) tool to assess the bias risk in retrospective observational studies. For details about the domain and scoring system, refer to Supplementary Table 2.
Meta-analysis
The meta-analysis was performed using Review Manager (RevMan) version 5.4 or OpenMetaAnalyst [17, 18]. We used OpenMetaAnalyst in cases where the event count was zero in both the DBS and FUS groups, applying a correction factor of 0.5, as recommended by the Cochrane Handbook when both arms include zero events [19], since this function is not available in RevMan. For continuous outcomes, we analyzed the pooled mean difference (MD) with a 95% confidence interval (CI). We opted for the MD over the Standardized Mean Difference (SMD) because all included studies utilized the same assessment tool (CRST) and reported scores in the same units (points). This allowed for a direct, clinically meaningful comparison of the absolute treatment effect between DBS and MRgFUS. For dichotomous outcomes, such as the incidence of AEs and response rate, we calculated the Risk Ratio (RR) and its 95% CI.
We applied a random-effects model because it better accounts for heterogeneity or variability between groups or individuals [20]. In random-effects models, smaller studies are given relatively more weight compared to fixed-effect models. This model also allows for greater variability in the pooled estimate, which is more suitable for data that may contain inconsistencies or variations. As a result, the effect sizes derived from our meta-analysis are conservative estimates that take possible heterogeneity into consideration.
Heterogeneity was considered significant if the p-value was less than 0.1 or the I^2^ statistic was greater than 50% [21]. When significant heterogeneity was present, we performed a leave-one-out analysis to address it [22]. Since fewer than ten studies were included, assessment of publication bias was not applicable, in accordance with Cochrane guidelines [23].
Results
Search and screening
Our initial database search retrieved 608 studies, then we removed the duplicates to have 501 articles ready for title and abstract screening. We excluded 470 articles for not meeting the eligibility criteria, resulting in the inclusion of 31 articles for the full-text screening. Ultimately, five studies [14, 15, 24–26] remained for data extraction and analysis as thoroughly described in Fig. 1.Fig. 1PRISMA flow diagram of study selection. Flow chart illustrating the process of study identification, screening, eligibility assessment, and final inclusion. A total of 608 records were identified, with 5 studies meeting the inclusion criteria for the meta-analysis
Summary and baseline characteristics
Table 1 shows five retrospective cohort studies (2 in the USA, 2 in Canada, and 1 in South Korea), with a mean follow-up period of 15 months. All studies in the FUS reported unilateral treatment targeting the Vim using MRI guidance, whereas the DBS reported bilateral and unilateral procedures targeting the Vim. All the studies in the DBS group used MRI guidance except the Huss et al. [15] study, which was the only study to report computed tomography (CT) and 1.5- or 3-Tesla (T) MRI in the imaging modality.Table 1. Summary of included studiesStudy IDStudy designRecruitment durationFollow-upCountryFUS detailsDBS detailsInclusion criteria Summary of the study Unilateral/BilateralTargetImagingUnilateral/BilateralTargetImaging Huss 2015Retrospective cohort2004–201313 monthsUSAUnilateralVIMMRIBothVIMCT and 1.5 or 3-T MRIPatients with ET underwent both preoperative and postoperative CRST evaluations by the same neurologic specialist and physical therapistThe study showed that bilateral DBS is more effective than unilateral DBS or FUS in improving tremors Kim 2017Retrospective cohort1995–201412 monthsSouth KoreaUnilateralVIM3-T MRIBothVIM1.5-T MRIPatients with drug-resistant ETBilateral thalamic DBS reduces overall tremor more than unilateral DBS or FUS; however, both unilateral and bilateral treatments are equally effective for contralateral hand tremor and show no significant differences in disability or quality of life outcomes Harary 2019Retrospective cohortNA12 monthsUSAUnilateralVIMMRIBothVIMMRIPatients with ETPatients with drug-resistant ET experienced similar outcomes from RF thalamotomy, DBS, and MRgFUS, with fewer treatment-related complications observed in DBS and MRgFUS Germann 2024Retrospective cohortNA13.8 monthsCanadaUnilateralVIM1.5–3 T MRIUnilateralVIM1.5–3 T MRIPatients with ET who have hand tremor that is medically refractory to two full doses of therapeutic medication and who have substantial disability in performing at least two daily activitiesComparison of DBS and MRgFUS efficacy maps suggests a potentially more antero-superior lesion target that may reduce complications while preserving efficacy Sarica 2025Retrospective cohort2000–202424.5 monthsCanadaBilateralVIMMRIBilateralVIMMRIPatients with ET who underwent successful first-side surgery and exhibited residual tremors on the contralateral sideBilateral MRgFUS and DBS seem equally effectiveCRST clinical rating scale for tremor, CT computed tomography, DBS deep brain stimulation, ET essential tremor, FUS focused ultrasound, MRI magnetic resonance imaging, MRgFUS magnetic resonance-guided focused ultrasound, RF radiofrequency, T Tesla, VIM ventral intermediate nucleus
Table 2 summarizes the baseline characteristics of 192 patients (133 males, 59 females) in the FUS group and 271 patients (173 males, 98 females) in the DBS group. The pooled mean age and the SD in the FUS group and DBS group were 66.8 ± 14.8 and 62.3 ± 13.9 years, respectively. Moreover, the pooled mean of the disease duration is 30.7 years with an SD of 17.7 in the FUS group, compared to a pooled mean of 27.5 years with an SD of 17.3 in the DBS group. The baseline CRST in the FUS group has a pooled mean of 57.4 with an SD of 10.4, compared to a pooled mean of 58.7 with an SD of 11.2 in the DBS group.Table 2. Baseline characteristics of patients in FUS and DBS groupsStudy IDSample size (no.)Age, years, mean (SD)Sex, Males No: Females NoDisease duration (y), mean (SD)Baseline total CRST, mean (SD)Baseline QUEST, mean (SD)FUSDBSFUSDBSFUSDBSFUSDBSFUSDBSFUSDBS Huss 2015157067.265.02 (11.9)10:558:12NRNR54.961.937.552.1 Kim 2017231964.7 (8.04)62.8 (13.5)20:313:620.5 (13.13)14.1 (7.317)NRNRNRNR Harary 20195612770.8 (8.7)64.6 (9.6)37:1969:5828.3 (16.4)29.1 (17.4)NRNR42.649.1 Germann 2024793371.1 (9)65.6 (9.4)53:2622:1135.4 (18.4)28.8 (18.1)57.7 (15.8)58.7 (11.03)NRNR Sarica 2025192235.5 (17.9)34.9 (18.2)13:611:11NRNR56.3 (7.6)58.8 (11.7)NRNRCRST clinical rating scale for tremor, DBS deep brain stimulation, FUS focused ultrasound, M males, F females, NR not reported, QUEST quality of life in essential tremor questionnaire, SD standard deviation, y years
Risk of bias assessment
The NOS tool evaluated the five included retrospective cohorts. Four studies [14, 15, 24, 25] showed good quality and scored 8 out of 9. However, one study [26] showed poor quality and scored 6 out of 9 due to the lack of comparability (see Supplementary Table 2).
Clinical rating scale for tremor (CRST)
Four studies [15, 24–26], including 421 patients (169 in FUS and 252 in DBS), reported CRST outcomes. Analysis of the change from baseline in total CRST score favored DBS over FUS, showing a statistically significant greater improvement for DBS (MD: 5.12, 95% CI: [1.08, 9.16], P = 0.01) (Fig. 2). Heterogeneity was insignificant across the studies (I^2^ = 15%, P = 0.31). In contrast, there was no statistically significant difference between the FUS and DBS groups regarding the change in CRST Part A score (MD: 1.54, 95% CI: [−0.54, 3.63], P = 0.15), with insignificant heterogeneity (I^2^ = 37%, P = 0.21) (Fig. 2).Fig. 2. Forest plot of the effect of DBS vs. FUS on total and part A CRST scores. Meta-analysis comparing the change from baseline in total CRST and CRST Part A scores between patients undergoing DBS and those receiving FUS. DBS showed significantly greater improvement in total CRST (MD: 5.12, 95% CI: [1.08, 9.16], P = 0.01), with insignificant heterogeneity (I^2^ = 15%, P = 0.31). No significant difference was found in CRST Part A (MD: 1.54, 95% CI: [−0.54, 3.63], P = 0.15), with insignificant heterogeneity (I^2^ = 37%, P = 0.21). (*: 12 months, #: 41 months, ##: 16 months)
Response rate
The 12-month response rate was reported in two studies with 125 patients (38 in FUS and 87 in DBS) [14, 15]. There was no statistically significant difference in the response rate between the two groups (RR: 0.94, 95% CI: [0.77, 1.15], P = 0.56) (Fig. 3). The pooled results were homogenous (I^2^ = 0%, P = 0.90).Fig. 3. Forest plot of the response rate between DBS and FUS groups. Pooled analysis of the response rate at 12 months among patients undergoing DBS and FUS. No statistically significant difference was observed between the two groups (RR: 0.94, 95% CI: [0.77, 1.15], P = 0.56), with no heterogeneity (I^2^ = 0%, P = 0.90)
Adverse events (AEs)
We analyzed AEs reported in at least two studies; all AEs are reported in Supplementary Table 3. The overall incidence of any AE did not differ significantly between FUS (50.4%) and DBS (58.1%) (RR: 0.85, P = 0.46), as shown in Fig. 4. Paresthesia (RR: 4.57, P = 0.02), gait instability (RR: 2.85, P = 0.025), and dysphagia (RR: 3.40, P = 0.049) were all significantly more frequent in the FUS group. Specifically, gait instability is shown in Fig. 5A and dysphagia in Fig. 5B. Rates of dysarthria (RR: 0.48, P = 0.09), infection (RR: 0.65, P = 0.70), and mental status changes (RR: 0.68, P = 0.73) did not differ significantly between FUS and DBS (Fig. 4). Similarly, there was no significant difference in the risk of hemorrhage (RR: 0.87, P = 0.913), as shown in Fig. 5C.Fig. 4. Forest plot of adverse events in DBS vs. FUS. Meta-analysis comparing the incidence of multiple adverse events between patients treated with DBS and FUS. Paresthesia was significantly more common in the FUS group (RR: 4.57, 95% CI: [1.31, 15.94], P = 0.02), with insignificant heterogeneity (I^2^ = 32%, P = 0.23). There was no significant difference between the groups in the risk of dysarthria (RR: 0.48, 95% CI: [0.21, 1.11], P = 0.09; I^2^ = 0%, P = 0.98), infection (RR: 0.65, 95% CI: [0.08, 5.63], P = 0.70; I^2^ = 0%, P = 0.49), or mental status changes (RR: 0.68, 95% CI: [0.08, 5.87], P = 0.73; I^2^ = 0%, P = 0.94). The pooled analysis of any adverse event showed no statistically significant difference between FUS and DBS (RR: 0.85, 95% CI: [0.54, 1.32], P = 0.46), with moderate heterogeneity (I^2^ = 52%, P = 0.12)Fig. 5A Forest plot of gait instability in DBS vs. FUS. Patients undergoing FUS had a significantly higher risk of gait instability compared to those treated with DBS (RR: 2.85, 95% CI: [1.14, 7.08], P = 0.025), with insignificant heterogeneity (I^2^ = 33%, P = 0.204). B Forest plot of dysphagia in DBS vs. FUS. Pooled analysis revealed a higher incidence of dysphagia in the FUS group compared to DBS (RR: 3.40, 95% CI: [1.01, 11.46], P = 0.049), with no heterogeneity (I^2^ = 0%, P = 0.943). C Forest plot of hemorrhage in DBS vs. FUS. No statistically significant difference in the risk of hemorrhage was found between FUS and DBS (RR: 0.87, 95% CI: [0.07, 10.58], P = 0.91), with insignificant heterogeneity (I^2^ = 10%, P = 0.291)
Discussion
Our meta-analysis demonstrated that DBS provides significantly greater improvement in total CRST scores compared with MRgFUS, whereas no significant differences were observed for CRST Part A or the 12-month response rate. FUS was associated with higher rates of paresthesia, gait instability, and dysphagia, while other AEs, including dysarthria, infection, hemorrhage, and mental status changes, were comparable between groups. Overall, these findings reflect a trade-off in which DBS offers stronger total tremor suppression, whereas MRgFUS carries a higher likelihood of certain sensory and gait-related AEs.
Both DBS and MRgFUS modulate tremor circuitry at the level of the Vim, a major relay within the cerebello–thalamo–cortical network implicated in ET. DBS achieves tremor reduction by applying adjustable electrical stimulation that modulates pathological oscillations within this circuit, allowing postoperative titration and management of stimulation-related side effects. In contrast, MRgFUS produces a precise, MRI-guided thermal lesion that permanently disrupts the aberrant tremor pathway [27–29]. The irreversibility of MRgFUS underscores the importance of accurate targeting, whereas DBS offers ongoing flexibility that may contribute to its overall efficacy profile.
Regarding study quality, most included cohorts were of good methodological quality, although one study had limited comparability [26]. Sensitivity analyses excluding this study showed that the direction of effect for most outcomes remained unchanged, supporting the robustness of the primary findings.
Interpretation of laterality is essential when comparing modalities. DBS was frequently performed bilaterally in the included studies, whereas MRgFUS was predominantly unilateral [14, 15, 25, 26]. This likely contributed to the superior total CRST improvement observed with DBS. Patients undergoing staged bilateral DBS often demonstrate strong first-side outcomes and fewer AEs before receiving the second implant, introducing a degree of selection bias. Conversely, evidence for bilateral MRgFUS remains extremely limited; only one short-term study has reported outcomes, and its highly selective design limits broader applicability [24].
The knowledge gap surrounding bilateral MRgFUS represents one of the most critical limitations in the current literature. Although long-term data for bilateral DBS demonstrate a gradual attenuation of benefit, such as the decline from 57 to 43% improvement over four years reported by Sarica et al. [24], no comparable long-term data exist for bilateral MRgFUS. Furthermore, the long-term safety of bilateral thermal lesions, particularly with respect to gait, speech, and sensory function, remains unknown. This lack of data prevents definitive comparisons between bilateral MRgFUS and its DBS counterpart and should be highlighted as a central limitation.
Differences in AE profiles between procedures also warrant clinical consideration. MRgFUS carries a higher incidence of sensory and gait-related complications, likely due to perilesional edema or lesion extension into adjacent fiber tracts [26]. Neurological AEs may decline as operator experience increases, yet current data remain heterogeneous. DBS, on the other hand, presents a distinct set of risks, such as infection, hemorrhage, or hardware-related complications, that were infrequent but exclusive to the DBS cohorts. The adjustability of DBS allows many stimulation-related AEs to be mitigated postoperatively [24], which may contribute to its overall safety profile in long-term use.
Targeting considerations further differentiate both approaches. The irreversibility of MRgFUS makes optimal lesion placement crucial, whereas DBS enables postoperative refinement through contact selection and stimulation adjustments. Evidence from recent connectomic and probabilistic mapping studies suggests that networks involving the primary motor cortex (M1), primary somatosensory cortex (S1), cerebellum, and supplementary motor area play key roles in tremor suppression [30, 31]. How these findings translate to optimizing MRgFUS targeting remains an area requiring further investigation.
Clinically, bilateral approaches appear most appropriate for patients with significant axial tremor and functional impairment, given the substantial improvements observed after second-side DBS. Unilateral procedures may suffice for patients with predominantly asymmetric tremor. Treatment selection should therefore integrate tremor laterality, patient comorbidities, willingness to manage implanted hardware, and tolerance for sensory or gait-related risks.
Overall, the current evidence indicates that DBS may provide greater total tremor reduction, whereas MRgFUS offers a non-invasive alternative with a distinct AE profile. However, the absence of long-term and bilateral MRgFUS data remains a substantial limitation that restricts definitive comparisons. Future prospective studies with balanced bilateral designs, longer follow-up intervals, and standardized reporting will be essential to refining patient selection and optimizing therapeutic outcomes.
Limitations and recommendations
Our systematic review and meta-analysis are subject to several limitations. The small number of included studies, with several key outcomes, including response rate, CRST Part A, and numerous individual AEs (e.g., mental status changes, infection, and hemorrhage), reported in only two studies, limits the generalizability and robustness of conclusions that can be drawn from these specific outcomes. Additionally, only one study reported outcomes for bilateral MRgFUS, preventing subgroup analyses based on procedure laterality. While four of five studies displayed a low risk of bias, one study revealed poor quality due to issues with comparability. The overall sample size is relatively small, with a higher percentage of male participants: 192 patients (69.27% male) in the MRgFUS group and 271 patients (63.84% male) in the DBS group. Most studies primarily compared bilateral DBS with unilateral MRgFUS, which may introduce bias given the recognized advantages of bilateral approaches. This focus could lead to an overestimation of DBS's benefits when compared to MRgFUS. Additionally, selection bias may influence findings, as patients with more severe conditions are often referred for DBS, potentially skewing the results. Those undergoing bilateral procedures are likely to demonstrate better first-side outcomes and experience fewer AEs, complicating assessments of efficacy. Although most outcomes revealed no significant heterogeneity, moderate heterogeneity was noted for any AE outcome. Possible differences among the included studies may have contributed to this heterogeneity, including variations in intervention protocols regarding laterality, as well as differences in baseline age and follow-up duration. These factors likely influenced the heterogeneity, and therefore, the results should be interpreted with caution. Lastly, the retrospective nature of the studies contributes to the risk of recall bias and missing data, which may limit the clinical applicability of these findings. Addressing these limitations in future research will be crucial for enhancing the reliability and relevance of comparative effectiveness studies in this area.
Author’s conclusion
DBS and MRgFUS both provide meaningful tremor reduction for patients with ET, but their benefits differ in important clinical ways. DBS may offer greater overall improvement in total CRST scores and remains particularly advantageous for patients with bilateral or disabling axial tremor, given its adjustability and established bilateral efficacy. In contrast, MRgFUS represents an effective noninvasive alternative that may be preferable for patients who wish to avoid implanted hardware or who prioritize a single-session, incisionless procedure, while recognizing its higher rates of certain sensory and gait-related AEs.
A major limitation of the current evidence is the lack of long-term data and the near absence of studies evaluating bilateral MRgFUS, which prevents definitive comparison with bilateral DBS. Additionally, variability in outcome definitions across studies limits consistency in reported effects. Future research should prioritize balanced bilateral comparisons, longer follow-up, and standardized outcome measures to more accurately determine the relative benefits and risks of both procedures.
Supplementary Information
Below is the link to the electronic supplementary material.Supplementary file1 (DOCX 528 KB)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cochrane Handbook for Systematic Reviews of Interventions | Cochrane [Internet] (2024) [cited 2026 Jan 10]. Available from: https://www.cochrane.org/authors/handbooks-and-manuals/handbook
- 2PRISMA statement [Internet]. [cited 2024 Jul 17]. PRISMA 2020 checklist (2020) Available from: https://www.prisma-statement.org/prisma-2020-checklist
- 3Rev Man Knowledge Base - RMW Knowledge Base [Internet] (2020) [cited 2024 Dec 18]. Available from: https://documentation.cochrane.org/revman-kb/revman-knowledge-base-55377928.html
- 4Open Meta-Analyst: open-source, cross-platform software for advanced meta-analysis | Cochrane Colloquium Abstracts [Internet] (2010) [cited 2025 Feb 6]. Available from: https://abstracts.cochrane.org/2010-keystone/openmeta-analyst-open-source-cross-platform-software-advanced-meta-analysis
- 5Chapter 10: Analysing data and undertaking meta-analyses | Cochrane [Internet] (2024) [cited 2025 Nov 14]. Available from: https://www.cochrane.org/authors/handbooks-and-manuals/handbook/current/chapter-10#section-10-4-4-1
- 69.5.2 Identifying and measuring heterogeneity [Internet] (2024) [cited 2024 Nov 6]. Available from: https://handbook-5-1.cochrane.org/chapter_9/9_5_2_identifying_and_measuring_heterogeneity.htm
- 79.5.3 Strategies for addressing heterogeneity [Internet] (2024) [cited 2024 Aug 13]. Available from: https://handbook-5-1.cochrane.org/chapter_9/9_5_3_strategies_for_addressing_heterogeneity.htm
- 810.4.3.1 Recommendations on testing for funnel plot asymmetry [Internet] (2024) [cited 2024 Nov 6]. Available from: https://handbook-5-1.cochrane.org/chapter_10/10_4_3_1_recommendations_on_testing_for_funnel_plot_asymmetry.htm