Addition of Multi‐Level Technologies to Evaluate Eggs and Embryos and Improve Endometrial Quality Applied for In Vitro Fertilization to Achieve Pregnancy: A Case Study
Tania G. Rojas‐Pérez, Yúvika Reyes‐Albarracín, Ginna Ortiz, Juan José Suárez, Diego Vilchis Reyes, Jacqueline Cordero Oropeza, Dinorah Hernández‐Melchor, Esther López‐Bayghen

TL;DR
This case study shows how combining advanced embryo selection and endometrial improvement techniques can lead to a successful pregnancy in a couple with infertility.
Contribution
The study demonstrates a novel integrated clinical approach combining molecular diagnosis and regenerative strategies for IVF success.
Findings
Combining PGTA, cumulus cell analysis, PRP, and dietary intervention led to a successful pregnancy.
A low-carb diet improved insulin resistance and endometrial receptivity within two weeks.
PRP application enhanced endometrial quality and supported embryo implantation.
Abstract
Preimplantation genetic testing for aneuploidies (PGTA) diagnoses chromosomal abnormalities and can be complemented by cumulus cell transcriptional analysis to assess egg and ovarian quality and development during embryo culture. In addition to selecting the best available embryo, intrauterine administration of platelet‐rich plasma (PRP) and correction of insulin resistance (IR) through nutritional intervention can improve endometrial quality. This case report examines the potential feasibility of combining in vitro fertilization (IVF) with four techniques to achieve a viable pregnancy. A couple with a prior successful IVF pregnancy was seeking a second pregnancy. The patient was diagnosed with polycystic ovary syndrome (BMI = 24.5 kg/m2), whereas her partner had teratozoospermia. For the first IVF cycle, using PGTA, we confirmed that only euploid embryos were transferred. A…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
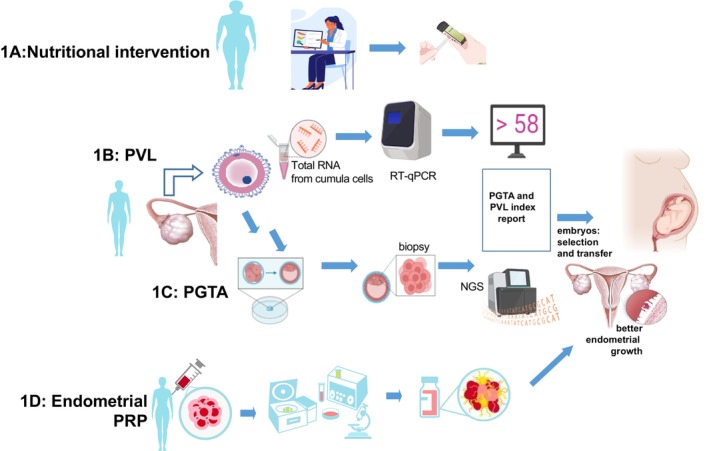 FIGURE 1
FIGURE 1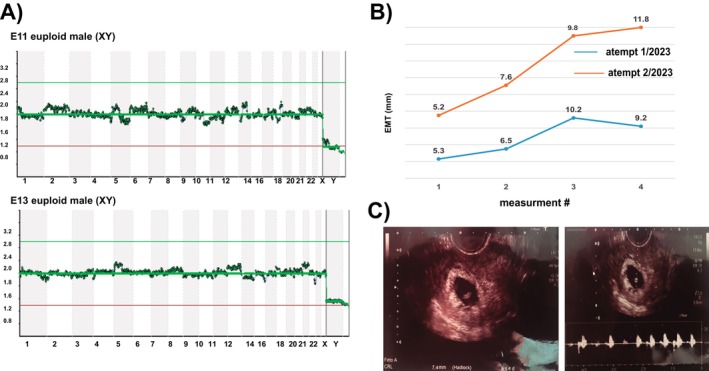 FIGURE 2
FIGURE 2| Category | Failed IVF treatment 2023 | Successful IVF treatment to achieve a second pregnancy in 2023 | |
|---|---|---|---|
| Nutritional intervention | No | Ketogenic diet | |
| Anthropometric/nutritional parameters | |||
| Nutritional intervention | |||
| Before | After | ||
| Age (years) | 36 | 36 | |
| Weight (kg) | 53 | 52 | 50 |
| Waist circumference (cm) | NA | 72 | 69 |
| BMI (kg/m2) | 25.4 | 20.3 | 19.5 |
| Blood pressure (mmHg) | N/A | 100/60 | 90/60 |
| Carbohydrates (g/day) | NA | 176 | 49 |
| Biochemical parameters | |||
| Fasting glucose (mg/dL) | NA | 77 | 75 |
| Ketones in urine (mg/dL) | NA | Negative | 80 |
| Insulin (mIU/mL) | NA | 15.9 | 8.57 |
| HOMA‐IR | NA | 3.02 | 1.59 |
| QUICKI (insulin sensitivity) | NA | 0.324 | 0.356 |
| Triglycerides (mg/dL) | NA | 123 | 94 |
| Triglycerides‐glucose‐BMI | NA | 171.8 | 159.27 |
| IVF parameters | |||
| Oocyte source | Patient | Patient | |
| Oocytes collected ( | 26 | 27 | |
| Oocytes fertilized (%) | 76% | 59% | |
| Embryos ( | 4 | 5 | |
| Molecular analysis | |||
| PGTA |
E3 Abnormal (−22) XX E4 Abnormal (−8) XX E11 Abnormal (−16, +22) XX |
| |
| PVL (transcriptional analysis of cumulus cells) | NA |
E15 = PVL 51.19 E21 = PVL 52.28
| |
| Embryo quality (morphology grade at inner cells mass/trophectoderm) |
E3 B/B, E4 B/B, E11 A/B |
| |
| Embryos transferred | 1 (E1) | 2 (E11, E13) | |
| Endometrial interventions | |||
| Endometrial corrections | Hysteroscopy (normal cavity) and platelet‐rich plasma (two applications) | ||
| Endometrial thickness (mm; at the transfer day) | 9.2 | 11.8 | |
| Obstetric outcomes | |||
| Implantation | Negative | Positive | |
| β‐hCG day 14 | NA | 362.0 mUI/mL | |
| Clinical pregnancy (US result) | NA | Yes (one sack with heartbeat) | |
| Nutritional control during pregnancy | NA | 54.2 g average CH/day | |
| Pregnancy result | NA | 39 weeks, healthy male, 53 cm, 3465 g, Apgar 8/9 | |
|
|
| Pregnancy week | |||||
|---|---|---|---|---|---|---|---|
| 6 | 8 | 13 | 17 | 28 | |||
| Carbohydrates (g/day) | 49 | 93 | 59 | 48 | 55 | 57 | 52 |
| Weight (kg) | 50.2 | 50 | 49 | 48.7 | 48 | 55.5 | 57 |
| BMI (kg/m2) | 21.1 | 23.1 | 22.7 | 22.5 | 22.2 | 25.7 | 26.4 |
| Fasting glucose (mg/dL) | 75 | 81 | 84 | 81 | 74 | 81 | 76 |
| Ketones in urine (mg/dL) | 80 | NA | NA | NA | NA | NA | NA |
| Insulin (mIU/mL) | 8.57 | NA | 9.1 | NA | NA | 11 | NA |
| HOMA‐IR | 1.59 | NA | 1.88 | NA | NA | 2.2 | NA |
| QUICKI | 0.356 | NA | 0.347 | NA | NA | 0.339 | NA |
| Triglycerides (mg/dL) | 94 | 96 | 100 | 84 | 61 | 96 | 109 |
| Triglycerides‐glucose‐BMI | 159.2 | 161.1 | 159.7 | 155.4 | 147.2 | 153.4 | 185.4 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsReproductive System and Pregnancy · Reproductive Biology and Fertility · Prenatal Screening and Diagnostics
Introduction
1
Reproductive medicine faces the challenge of diagnosing and resolving problems at multiple levels within a single case. From oocyte collection, embryo fertilization, and selection to improving patient health for implant preparation and development, this work still needs to be done individually or, ideally, collectively. Preimplantation genetic testing for aneuploidies (PGTA) screens for chromosomal abnormalities and enables the selection of euploid embryos, thereby increasing the likelihood of obtaining normal embryos, potentially limiting diseases such as Turner and Laron Syndromes, propionic acidemia, and Carnitine‐acylcarnitine Translocase Deficiency [1, 2, 3, 4]. In addition to genomic testing, noninvasive alternatives are still needed to assess embryonic parameters and enhance the potential for successful implantation. For example, analyzing cumulus cells (CC) as a non‐invasive way to assess individual egg quality through transcriptional analysis of Prostaglandin‐Endoperoxide Synthase 2 (PTGS2) and Versican (VCAN) gene expression, normalized to the L19 ribosomal gene as a control (PVL index). A PVL index score ≥ 58.2 has been associated with oocytes that produce better embryos for transfer [5]. These two techniques could more accurately select metabolically competent oocytes and euploid embryos.
Concerning the maternal side, an excellent endometrial lining is not always achievable. It is challenging to diagnose as fit—ideally, 7 mm thick at embryo implantation with a trilaminar structure [6]. Endometrial regeneration with endogenous growth factors involves applying platelet‐rich plasma (PRP) during endometrial preparation to improve endometrial quality in infertile patients [7]. Alternatively, improving the patient's health through nutritional interventions that correct their metabolic profile and insulin resistance (IR) could improve in vitro fertilization (IVF). In patients with polycystic ovarian syndrome (PCOS), a low‐carb dietary intervention (limited carbohydrate intake) improved waist circumference, serum triglycerides, and fasting plasma glucose (FPG), leading to reduced IR and favoring implantation and clinical pregnancy [8]. Here, we present the case of a patient who underwent four combined techniques and achieved 39 weeks of pregnancy, resulting in the delivery of a male baby.
Case Presentation
2
Case History, Physical, and Laboratory Examinations
2.1
A couple with secondary infertility associated with PCOS and teratozoospermia attended the Instituto de Infertilidad y Genética México SC, INGENES, México City, in 2023. The couple opted to undergo IVF due to a successful IVF in 2019, where three euploid embryos were transferred. This earlier IVF (2020) resulted in a healthy male baby.
For the 35‐year‐old male partner, sperm quality was obtained from the Andrology Laboratory of the Ingenes Institute. Semen samples were collected by masturbation (after 3–5 days of abstinence) on the day of the IVF procedure. After liquefaction, samples were analyzed according to the WHO criteria for volume, time of liquefaction, pH, leukocyte concentration, sperm concentration, progressive motility, morphology (by the Kruger criteria), and viability according to the WHO (2010) parameters [9, 10]. Sperm morphological diagnosis indicated abnormal shapes (teratozoospermia).
The 36‐year‐old female was slightly overweight (BMI = 25.4 kg/m^2^). Her overall medical history was unremarkable, with no reproductive health conditions. The patient's anthropometric measurements were within standards for Latina women. The patient had a history of PCOS. Imaging examination showed more than 30 follicles on each ovary, as detected by ultrasound. PCOS was confirmed using the Rotterdam criteria: at least two of three conditions: (a) clinical signs of hyperandrogenism, (b) oligo/amenorrhea or amenorrhea, and (c) polycystic ovaries confirmed by ultrasound [11]. Laboratory tests were performed to evaluate metabolic status. In the initial evaluation, the patient was in a state of hyperinsulinemia. HOMA‐IR index was calculated, indicating she was IR.
For this case study, four methods were employed: (1) nutritional intervention to improve critical metabolic factors, such as FPG, triglycerides (TG), and insulin (FPI); (2) intrauterine PRP application to improve endometrium quality and promote embryo implantation; (3) assessing oocyte quality with the PVL index; and (4) PGTA to ensure only euploid embryos were transferred (Figure 1).
Representative and schematic overview of all technologies applied together in the case. (A) Nutritional intervention based on carbohydrate restriction and ketosis induction. (B) Granulosa cells qRT‐PCR analysis to analyze PVL index. (C) PGT‐A analysis to determine genomic normality in chromosomal number. (D) Plasma‐rich platelet applied to the endometrium before endometrial preparation to improve endometrial growth.
IVF
2.1.1
The patient underwent controlled ovarian stimulation with a gonadotropin‐releasing hormone antagonist (Gonal 150 UI and Merapur 150 UI). The stimulus was prolonged until the diameter of the leading follicles was > 18 mm. Afterward, recombinant human chorionic gonadotropin was administered. After 36 h, the oocytes were retrieved with ultrasound guidance. All 14–18 mm follicles were aspirated, and ova were collected and fertilized by intracytoplasmic sperm injection (ICSI) with the partner's sperm and then cultured. Embryos were cryopreserved using vitrification.
Frozen–thawed embryos were implanted during an estrogen‐primed cycle. The uterine transfer occurred during a controlled endometrial development cycle free of gonadotropins. Endometrial preparation with 6 mg of estrogen valerate (Primogyn, UPC: 00770333115702) was started on menstrual cycle day (MCD) 2 with a 10‐day increasing‐dose scheme, beginning with 2 mg/day and increasing to a maximum of 8 mg/day, and assessing endometrial mean thickness (EMT) every other day via ultrasound. Blastocysts were transferred. Embryo implantation was confirmed on Day 14 by serum β‐hCG concentrations > 10 mUI/mL and clinical pregnancy by the presence of a fetal heartbeat using ultrasound at 6 weeks.
Preimplantation Genetic Test for Aneuploidies (PGTA)
2.1.2
Aneuploidy analysis was performed according to the Ingenes Institute's standardized protocol, using trophectoderm biopsies from morphologically good‐quality embryos before vitrification [12].
Intrauterine PRP
2.1.3
Autologous PRP administration was performed according to Hernandez‐Melchor et al. [7] into the uterus during an estrogen‐primed cycle. Briefly, venous blood (3 mL) was drawn from the patient and centrifuged at 1200 rpm for 12 min. The plasma was obtained and centrifuged again at 3300 rpm for 7 min. PRP was collected and infused into the uterus within 10 min. On MCD 10, EMT was measured using ultrasonography, and 1 mL of autologous PRP was collected and infused into the uterine cavity within 10 min of isolation to avoid protein degradation, using a Wallace Embryo Transfer Catheter (SureView Soft 2 CE123). The procedure was repeated on MCD 12 as the EMT was < 7 mm.
Dietary Assessment and Nutritional Intervention
2.1.4
Using a direct food intake questionnaire, the patient's carbohydrate, fat, and protein intake was calculated in the MyFitnessPal app (before and during the nutritional intervention). The nutritionist confirmed the daily and weekly macronutrient intake and corrected the diet's macronutrient distribution when needed. A low‐carb dietary intervention, averaging approximately 1800 cal with a maximum daily carbohydrate intake of 50 g, was advised, with macronutrients adjusted to 20% carbohydrates, 35% protein, and 40% fat. Ketosis was monitored using Medicon Ketone Test Strips (China), and urinary ketones > 40 mg/dL were considered positive for ketosis. The patient received individualized counseling focused on achieving adequate intake of essential nutrients while limiting carbohydrates to levels that support stable glycemia and control of hyperinsulinemia. The dietary structure emphasized three main meals per day. Meal composition included a high‐quality protein source (such as fish, poultry, eggs, lean meats, or unsweetened dairy), non‐starchy vegetables, and healthy fats (such as olive oil, avocado, nuts, and seeds), as needed to support satiety and reduce postprandial glycemic excursions. At the same time, intake of ultra‐processed foods, refined carbohydrates, added sugars, grains, and foods high in sugar was reduced to a minimum.
Analysis for FPG, TG, and FPI was performed at an outside facility. Insulin sensitivity was calculated according to the QUICKI index: 1/(log FPG + log FPI), in which a value < 0.357 is considered low insulin sensitivity. IR was calculated according to the HOMA‐IR index: (FPG*FPI)/405, in which a score of > 2.0 is IR. The triglyceride‐glucose‐BMI (TyG‐BMI) index was calculated as ln(TG × FPG/2) × BMI.
PVL Index
2.1.5
The PVL index was determined using the method described by Ocampo et al. [5]. Briefly, the CCs were mechanically separated and collected for each cumulus‐oocyte complex. Afterward, the CCs' total RNA was isolated using TRIzol reagent according to the manufacturer's protocol. The expression, as a function of the cycle threshold, for the PTGS2 and VCAN genes, normalized to the L19 ribosomal gene, was measured by quantitative reverse transcription‐polymerase chain reaction to obtain the PVL index: [(PTGS2 + VCAN)*L19] [5]. The Step One Plus apparatus (Applied Biosystems) with the One Step Kappa Syberfast system (KAPA Biosystems, Woburn, MA, USA) was used in this study. A score ≥ 58.2 is a probable embryo of adequate quality for transfer.
Results
3
Initial evaluation determined that the patient suffered from PCOS with IR. Chronologically, the patient and her partner attended Ingenes for their second IVF. They underwent a standard protocol. Lack of endometrial competence was suspected and confirmed by hysteroscopy, but no abnormalities were found. The EMT was suboptimal, and a thin endometrium was diagnosed (before hysteroscopy, EMT = 3.6 mm). PRP was infused to improve endometrial quality before the embryo transfer (ET) attempt. Endometrial preparation was delayed by 1 cycle to achieve adequate endometrial growth (Figure 2B). The PRP treatment improved EMT thickness, and one euploid embryo was transferred (PGTA‐confirmed) but did not implant (β‐hCG < 10 mUI/mL). The patient opted to postpone another IVF cycle to lose weight.
(A) PGT‐A screening via genomic analysis for the selection of euploid embryos. (B) The endometrial mean thickness, along with the two major interventions. Endometrial thickness after regeneration using PRP to improve endometrial quality, achieving good endometrial growth in the two attempts; measurements after PRP application and endometrial preparation for frozen–thawed embryo transfer cycles are shown. On the first attempt in 2023, blue, one embryo diagnosed as euploid, was negative for pregnancy. In the second embryo transfer, after correcting the insulin resistance characteristic of the PCOS patient, endometrial thickness is shown by the orange line: 11.8 mm at the time of transfer. (C) Confirmation of clinical pregnancy by ultrasound showing a single embryonic sac with a fetal heartbeat. The sonogram is 6 weeks after embryo transfer.
By the patient's efforts, she lost weight and reduced her BMI to 20.3 kg/m^2^. Nevertheless, IR was assessed (HOMA‐IR), and even with the decrease in BMI, metabolic abnormalities persisted. The patient typically consumed an unbalanced standard American 2000‐cal diet with 55% carbohydrates, 25% fat, and 20% protein content. The patient was advised to follow a ketogenic diet to correct IR. Within 2 weeks, a 2‐kg weight loss and a reduction in BMI were observed (Table 1). Decreases were also observed in FPG and TG, lowering HOMA‐IR below the 2.0 threshold while increasing insulin sensitivity (Table 1).
The patient underwent a second round of controlled ovarian stimulation. However, this time, using the CCs, the PVL index was generated. Three oocytes were identified as potentially high‐quality (11, 13, and 27). After ISCI fertilization, embryos 11 and 13 were confirmed as euploid. PRP was infused to improve endometrial quality before ET. USG of the endometrium confirmed the ideal trilaminar structure (EMT = 11.8 mm), and the two embryos were transferred. Table 1 depicts the yields and quality of the embryos, whereas Figure 2A shows the euploidy of the two male‐transferred embryos. For the second ET, IR was corrected (Table 1). Ultrasound confirmed a clinical pregnancy with an embryo sac, fetal heartbeat of 131 beats per minute at Week 6 with normal amnio, and absence of markers for chromosomal defects (Figure 2C). The pregnancy was monitored through a structured prenatal care program under maternal–fetal medicine, with follow‐up visits scheduled once a month. The care protocol includes a first‐trimester screening between 11 and 14 weeks of gestation, during which maternal serum markers and an early ultrasound assessment were performed to evaluate the risk of chromosomal abnormalities and to assess early fetal development, yielding results within the normal range. A comprehensive second‐trimester anatomical (structural) scan was performed at 23 weeks to evaluate fetal anatomy in detail, screen for congenital anomalies, assess placental and uterine conditions, and confirm the male fetus. These follow‐ups monitor maternal well‐being, fetal growth, amniotic fluid volume, and other parameters essential to ensuring a healthy pregnancy. This schedule was continued until delivery, resulting in a healthy boy at Week 39 (length: 53 cm; weight: 3465 g; Apgar 8/9).
Discussions
4
In this case, multi‐level technologies were combined at the maternal and embryo levels, evaluating oocytes and embryos and improving endometrial quality to achieve a successful pregnancy.
Patients with PCOS exhibit lower pregnancy rates due to the inherent reproductive complications associated with the IR. A low‐carb dietary intervention was implemented to address IR associated with the PCOS condition. Clinical evidence has shown that patients with PCOS and IR exhibit poor oocyte development and maturation, particularly affecting the early stages of IVF cycles [13, 14]. Also, there is a higher proportion of adverse obstetric outcomes despite good oocyte quality and euploid embryos, suggesting that one adverse effect of IR may directly affect endometrial tissue and embryo implantation [15]. IR begins to develop due to excessive carbohydrate consumption, leading to a state of chronic hyperinsulinemia and a progressive loss of insulin sensitivity. In this context, restricting excessive carbohydrate consumption (glucotoxicity) was associated with correction of IR and improved obstetric outcomes [8, 14]. After low‐carb dietary intervention, the final HOMA‐IR, QUICKI, and TyG‐BMI indices indicated that IR resolved, whereas insulin sensitivity increased. The mechanism by which IR affects the endometrium is increasingly well described, and it is associated with the tissue's high energy demand. Any alteration in glucose and insulin homeostasis will disrupt endometrial cell growth and development, decidualization, and blastocyst recognition and adhesion, potentially leading to embryo implantation failure due to IR. Liver concentrations of Insulin‐like Growth Factor Binding Protein 1 and Sex Hormone Binding Globulin lead to decreased GLUT4 transporter‐dependent glucose uptake, contributing to hyperandrogenism [15] and exacerbating inflammation [6, 16, 17]. Endometrial tissue regeneration in patients with PCOS appears necessary to achieve positive obstetric outcomes. Although this patient had previously improved (EMT > 7 mm) with the PRP therapy, pregnancy has not been achieved even when transferring an euploid embryo. Endometrial fitness improved following the intensive nutritional intervention at the time of ET, with a final EMT of 11.8 mm. Regarding the maternal side, endometrial fitness improved following PRP and intensive nutritional intervention. Both may have equally contributed to embryo implantation and pregnancy development.
The PVL index was used to assess oocyte quality by analyzing CC transcriptional profiles. This index can predict the embryo's implantation potential by identifying a higher capacity to implant, leading to a clinical pregnancy [5, 18]. A high PVL index is associated with higher clinical pregnancy rates, as the assessed genes play a crucial role in oocyte maturation and are relevant indicators of oocyte competence [5]. In the previous cycle for this patient, four embryos progressed to day 5 of development (Table 1); however, PGTA analysis revealed that only one was euploid. Five mature embryos were obtained in the subsequent cycle, of which three were euploid and showed the best PVL indices (E11 = 68.89, E13 = 67.31, E27 = 59.64). The patient and clinician decided to transfer the male embryos E11 and E13. The use of the PVL index, coupled with standard morphological evaluation and PGTA, contributed to the success of the second pregnancy. The PVL index provides an alternative method for discriminating embryos from the same patient based on genetic parameters.
PCOS is known for being more difficult to keep a pregnancy, as it is associated with an increased risk of miscarriage, gestational diabetes mellitus, hypertensive disorders of pregnancy, preterm delivery, and gestational growth retardation [19, 20, 21]. Ranging from 200 to 350 g of daily carbohydrates, around 55% of the overall caloric intake from the typical American diet, the significant harms of refined carbohydrates occur from consuming excessive amounts of sugar‐laden foods. Elevated intakes of sugar‐laden foods are associated with an increased prevalence of metabolic syndrome and obesity (44%) and a higher risk of developing diabetes (26%) [22]. Evidence indicates that nutritional status influences endometrial receptivity and implantation. Diets characterized by controlled carbohydrate intake, low glycemic load, and nutrient‐dense food choices stabilize insulin levels and reduce inflammation and may promote a better peri‐implantation environment [23, 24]. In addition, improving metabolic health prior to an in vitro fertilization cycle could optimize the endometrial environment and potentially increase the likelihood of implantation, although additional mechanistic and interventional studies are needed [23, 24, 25].
An additional follow‐up of the patient's nutritional habits, using a monthly questionnaire, revealed that the patient maintained a low‐carbohydrate intake, averaging 75 g/day, and primarily avoided sugary and overprocessed foods, while consuming more vegetables as the primary carbohydrate source (Table 2).
There is a need for further research evaluating the effects of a low‐carb dietary intervention during pregnancy on child development. The low‐carb dietary intervention may have a positive effect on fertility in women with PCOS and blood pressure levels during pregnancy or take part in the prevention and treatment of diseases such as epilepsy, obesity, asthma, depression, anxiety, or autism.
Conclusions
5
The effectiveness of IVF in achieving a viable pregnancy is strengthened by jointly using techniques for embryo selection, IR correction, and endometrial regeneration. The low‐carb dietary intervention and endometrial regeneration increased endometrial thickness, resulting in a healthy birth.
Author Contributions
Tania G. Rojas‐Pérez: conceptualization, data curation, formal analysis, investigation, methodology. Yúvika Reyes‐Albarracín: data curation, investigation, methodology. Ginna Ortiz: investigation, methodology. Juan José Suárez: investigation, methodology. Jacqueline Cordero Oropeza: investigation, methodology. Diego Vilchis Reyes: investigation, methodology. Dinorah Hernández‐Melchor: data curation, writing – review and editing. Esther López‐Bayghen: conceptualization, investigation, project administration, resources, supervision, writing – original draft, writing – review and editing.
Funding
The authors have nothing to report.
Ethics Statement
The patient signed an informed consent form, and all identifiable data were anonymized in accordance with the Declaration of Helsinki and local clinical research regulations.
Consent
The patient provided written informed consent to publish this report in accordance with the journal's patient consent policy. The patient and her partner also provided written informed consent to participate in this study, in accordance with the Declaration of Helsinki and to the publication of their anonymized information in this article.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1M. S. Awadalla , R. Agarwal , J. R. Ho , L. K. Mc Ginnis , and A. Ahmady , “Effect of Trophectoderm Biopsy for PGT‐A on Live Birth Rate Per Embryo in Good Prognosis Patients,” Archives of Gynecology and Obstetrics 306, no. 4 (2022): 1321–1327.35821525 10.1007/s 00404-022-06679-x PMC 9470687 · doi ↗ · pubmed ↗
- 2N. Bich Trinh , A. Dinh Bao Vuong , and P. Nhon Nguyen , “Successful Management of Pregnancy in Turner Syndrome (Monosomy X): A Rare Condition‐Based Learning Experience From Vietnam,” International Journal of Reproductive Bio Medicine 22, no. 5 (2024): 411–416.39091431 10.18502/ijrm.v 22i 5.16442 PMC 11290197 · doi ↗ · pubmed ↗
- 3N. B. Trinh , A. D. B. Vuong , and P. N. Nguyen , “Successful Management by Selective Embryo in the Carnitine‐Acylcarnitine Translocase Deficiency With SLC 25A 20 C.199‐10T>G Variation: The First Case Report From Vietnam and Literature Review,” Oman Medical Journal 40, no. 3 (2025): e 763.41018717 10.5001/omj.2025.17PMC 12461142 · doi ↗ · pubmed ↗
- 4T. Rojas‐Perez , M. A. Alcantara‐Ortigoza , A. Gonzalez‐Del‐Angel , F. Camargo‐Diaz , and E. Lopez‐Bayghen , “Whole Genomic Amplification for Detecting Single‐Gene Variants Causing Inherited Disease,” Methods in Molecular Biology 3003 (2026): 187–201.41478957 10.1007/978-1-0716-5060-8_14 · doi ↗ · pubmed ↗
- 5A. Ocampo , J. Pedraza , G. Ortiz , E. Hernández‐Pérez , L. Porchia , and E. López‐Bayghen , “Assessment of Prostaglandin‐Endoperoxide Synthase 2 and Versican Gene Expression Profile From the Cumulus Cells: Association With Better In Vitro Fertilization Outcomes,” Journal of Ovarian Research 11, no. 1 (2018): 84.30241554 10.1186/s 13048-018-0456-2PMC 6148785 · doi ↗ · pubmed ↗
- 6N. X. Jiang and X. L. Li , “The Disorders of Endometrial Receptivity in PCOS and Its Mechanisms,” Reproductive Sciences 29, no. 9 (2022): 2465–2476.34046867 10.1007/s 43032-021-00629-9 · doi ↗ · pubmed ↗
- 7D. Hernandez‐Melchor , “Obesity Attenuates the Beneficial Effect of an Intrauterine Infusion of Autologous Platelet‐Rich Plasma During In Vitro Fertilization,” American Journal of Translational Research 16, no. 3 (2024): 838–854.38586113 10.62347/RDXA 5841 PMC 10994790 · doi ↗ · pubmed ↗
- 8C. Palafox‐Gomez , G. Ortiz , I. Madrazo , and E. Lopez‐Bayghen , “Adding a Ketogenic Dietary Intervention to IVF Treatment in Patients With Polycystic Ovary Syndrome Improves Implantation and Pregnancy,” Reproductive Toxicology 119 (2023): 108420.37290496 10.1016/j.reprotox.2023.108420 · doi ↗ · pubmed ↗