The effectiveness of Traditional Chinese Medicine in treating cancer related anemia: a systematic review and meta-analysis
Quan-yao Li, Zi-yu Zhang, Wen-xiao Yang, Hui Liu, Xi Li, Wen-chao Qiu, Zhao-wei Guo, Jun Shi

TL;DR
This study reviews and analyzes the effectiveness of Traditional Chinese Medicine in treating cancer-related anemia, finding it improves hemoglobin levels and quality of life.
Contribution
A systematic review and meta-analysis providing high-quality evidence for TCM's efficacy in treating cancer-related anemia.
Findings
TCM treatment improved hemoglobin levels, clinical efficacy, and immune function in cancer-related anemia patients.
The funnel plot indicated low publication bias, suggesting reliable results.
TCM enhanced TCM syndrome efficacy and quality of life for patients with cancer-related anemia.
Abstract
The aim is to systematically evaluate the clinical efficacy of Traditional Chinese Medicine (TCM) in the treatment of cancer related anemia (CRA), and to provide higher quality evidence-based medical evidence for the treatment of CRA with TCM. Pubmed, Embase, Cochrane library, Scopus, Web of Science, China National Knowledge Infrastructure (CNKI), China Biology Medicine Disk (CBM) and WanFang were searched for the literature on TCM treatment of CRA included in the databases from the establishment of the databases to December 2025. Meta-analysis was performed using ReVman5.3 software. 6,201 relevant literatures were retrieved. According to inclusion and exclusion criteria, a total of 58 literatures were included, with a total of 4,308 patients, including 2,157 patients in the treatment group and 2,151 patients in the control group. The treatment group was better than the control group…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
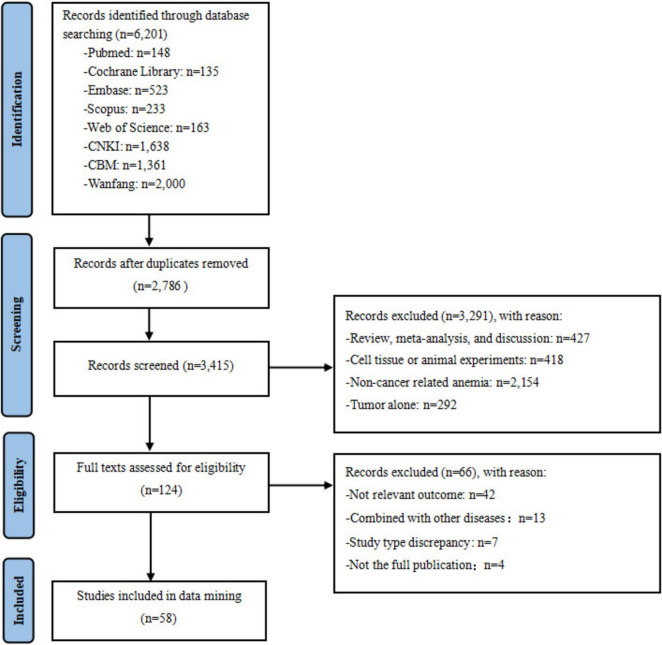 FIGURE 1
FIGURE 1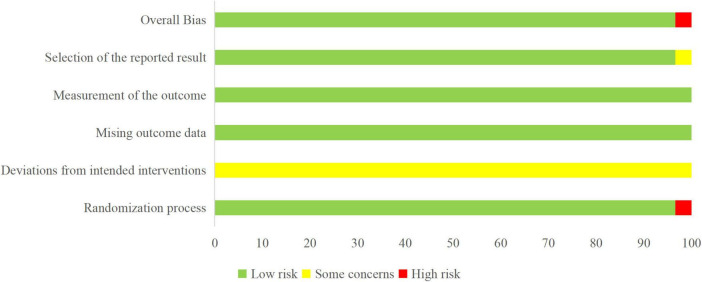 FIGURE 2
FIGURE 2 FIGURE 3
FIGURE 3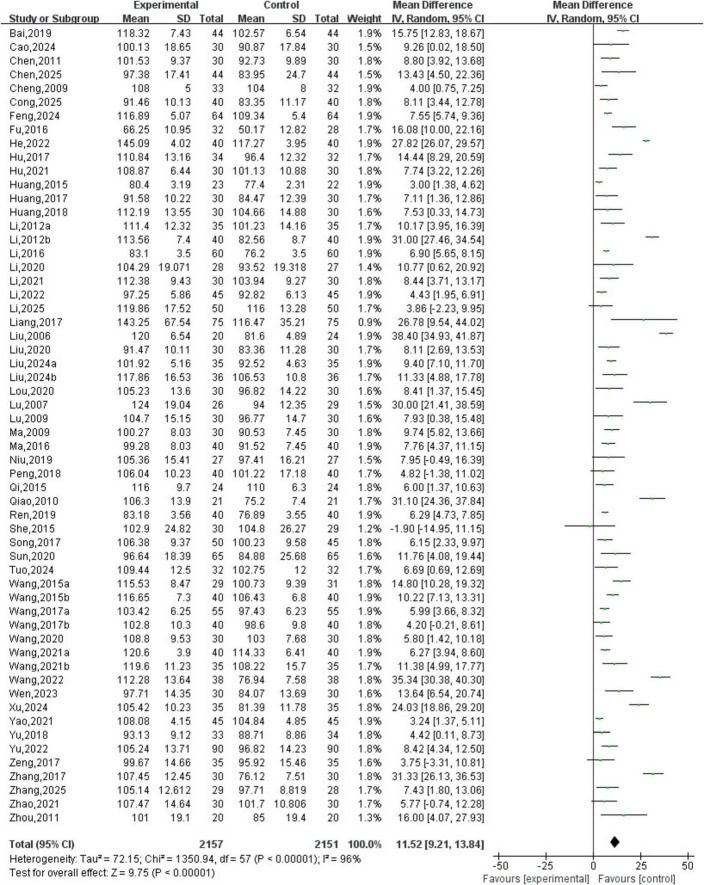 FIGURE 4
FIGURE 4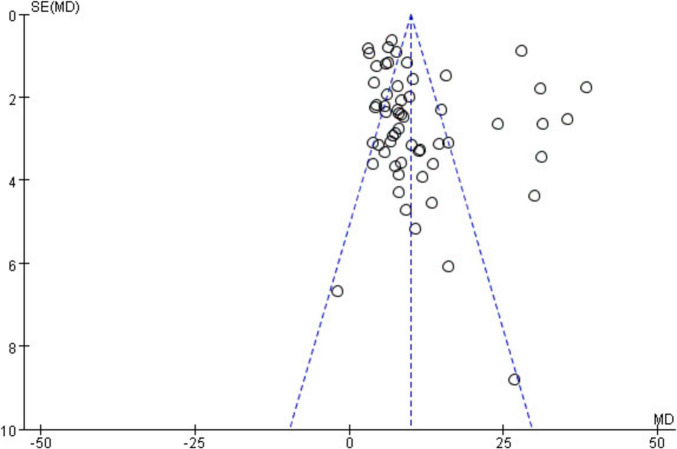 FIGURE 5
FIGURE 5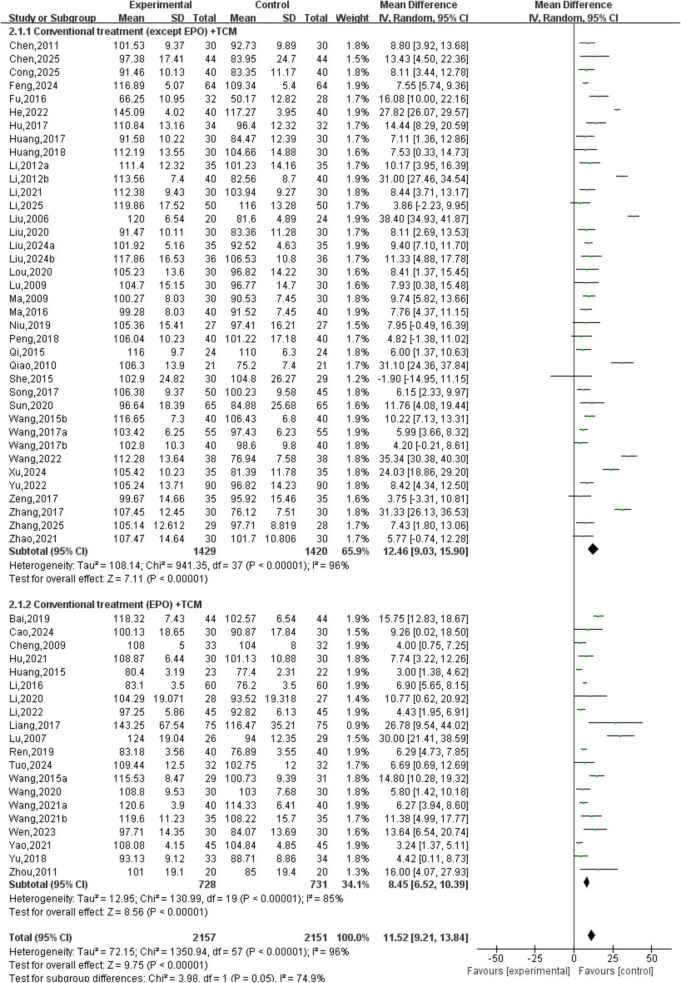 FIGURE 6
FIGURE 6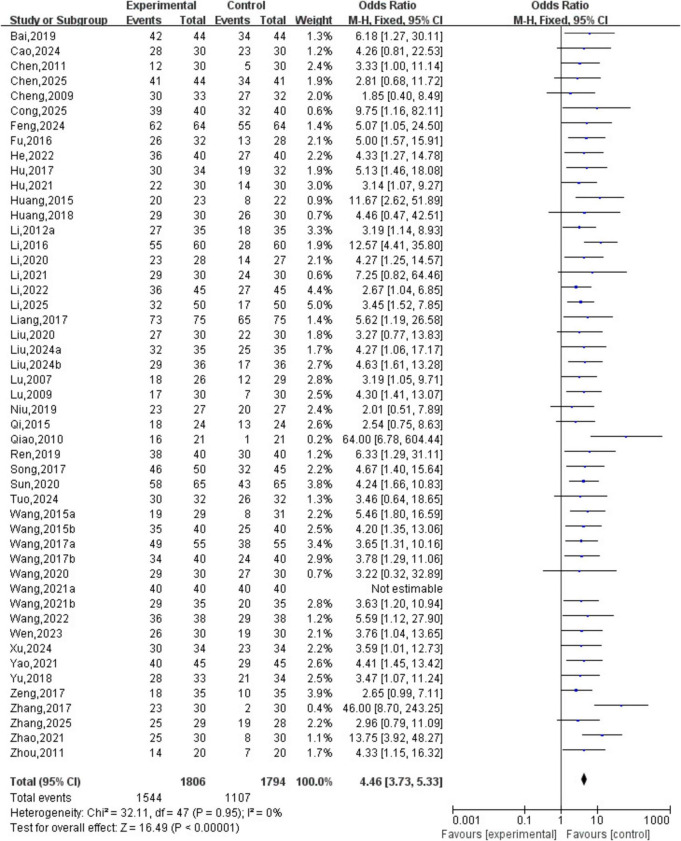 FIGURE 7
FIGURE 7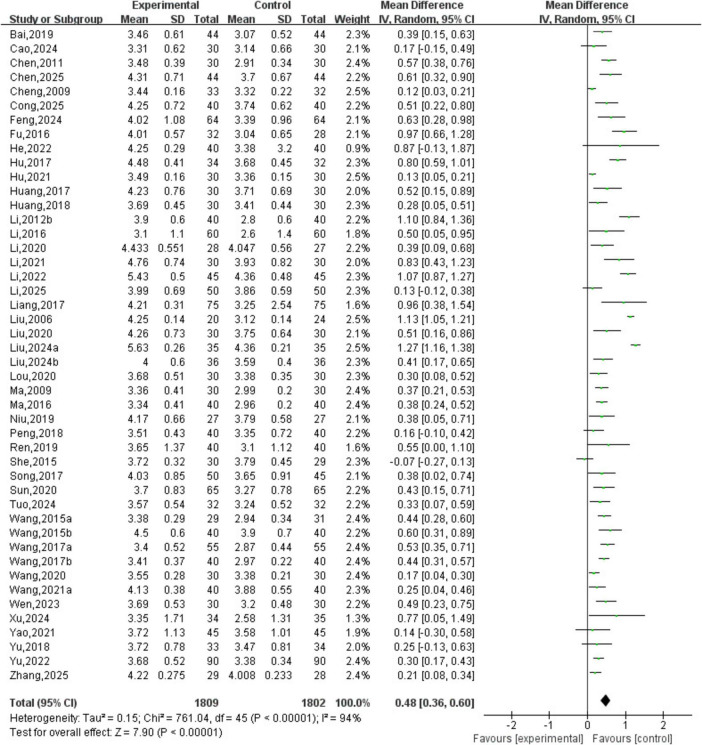 FIGURE 8
FIGURE 8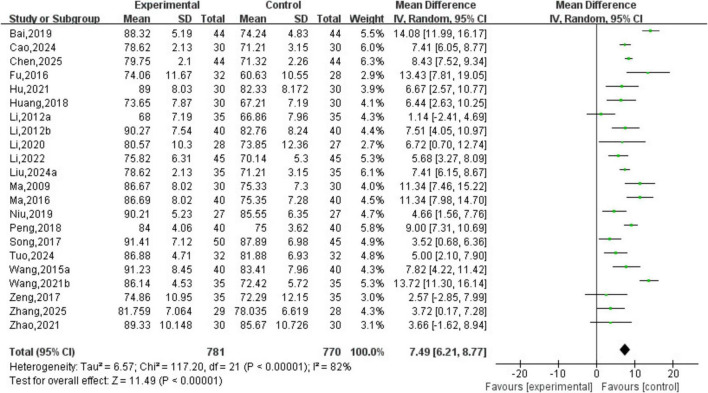 FIGURE 9
FIGURE 9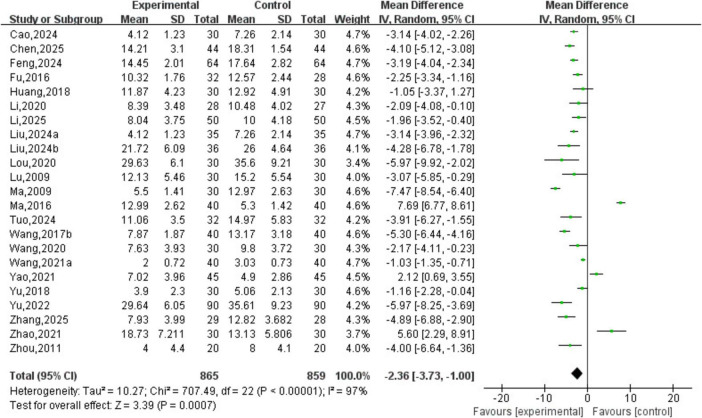 FIGURE 10
FIGURE 10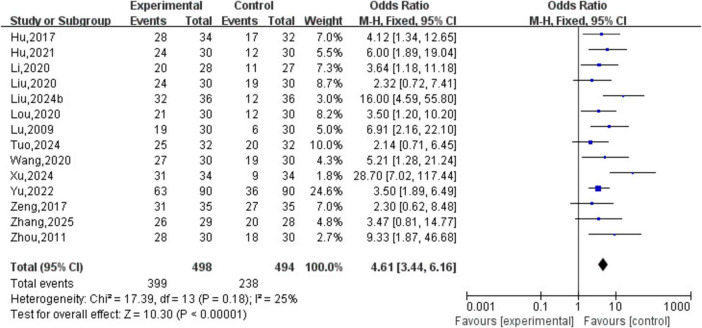 FIGURE 11
FIGURE 11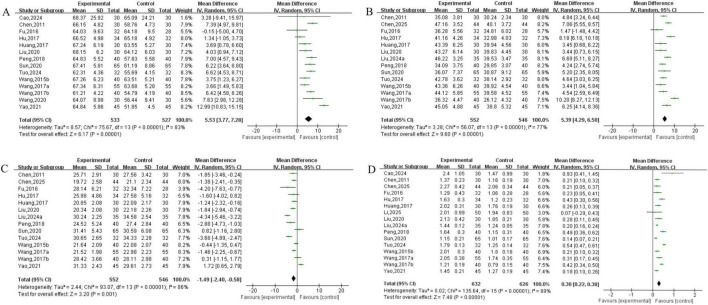 FIGURE 12
FIGURE 12| Included literature | Sample size | Grouping | Baseline | Intervention | Outcome measures | ||
|---|---|---|---|---|---|---|---|
| Control group | Treatment group | Control group | Treatment group | ||||
| Bai ( | 44 | 44 | Simple randomization | Coincide | EPO | EPO+TCM | ➀➁➂➃ |
| Cao et al. ( | 30 | 30 | Randomization | Coincide | EPO | EPO+TCM | ➀➁➂➃➄➆➉ |
| Chen ( | 30 | 30 | Randomization | Coincide | Symptomatic treatment | Standard chemotherapy+TCM | ➀➁➂➆➇➈➉ |
| Chen et al. ( | 44 | 44 | Randomization | Coincide | Conventional treatment | Conventional treatment+TCM | ➀➁➂➃➄➇➈➉ |
| Cheng et al. ( | 32 | 33 | Lottery method | Coincide | EPO | EPO+TCM | ➀➁➂ |
| Cong ( | 40 | 40 | Random number table | Coincide | Conventional treatment | Conventional treatment+TCM | ➀➁➂ |
| Feng et al. ( | 64 | 64 | Random number table | Coincide | Symptomatic treatment | Symptomatic treatment+TCM | ➀➁➂➄ |
| Fu et al. ( | 28 | 32 | Random number table | Coincide | Conventional treatment | TCM | ➀➁➂➃➄➇➈➉ |
| He et al. ( | 40 | 40 | Random number table | Coincide | Conventional treatment | Conventional treatment+TCM | ➀➁➂ |
| Hu and Jiang ( | 32 | 34 | Randomization | Coincide | Donkey-hide gelatin granules | TCM | ➀➁➂➅➆➇➈➉ |
| Hu and Liao ( | 30 | 30 | Envelope method | Coincide | EPO | EPO+TCM | ➀➁➂➃➅ |
| Huang ( | 22 | 23 | Randomization | Coincide | Shengxue Ning+EPO | Shengxue Ning+EPO+TCM | ➀➁ |
| Huang et al. ( | 30 | 30 | Random number table | Coincide | Conventional treatment | TCM | ➀➂➆➇➈➉ |
| Huang et al. ( | 30 | 30 | Randomization | Coincide | Xiangsha LiuJun BuGuZhi Decoction combined with SiWu Decoction | Xiangsha LiuJun BuGuZhi Decoction combined with SiWu Decoction+TCM | ➀➁➂➃➄ |
| Li ( | 35 | 35 | Lottery method | Coincide | Compound Donkey-hide gelatin slurry | TCM | ➀➁➃ |
| Li ( | 40 | 40 | Randomization | Coincide | Symptomatic treatment | Symptomatic treatment+TCM | ➀➂➃ |
| Li ( | 60 | 60 | Randomization | Coincide | EPO | EPO+TCM | ➀➁➂ |
| Li ( | 30 | 30 | Random number table | Coincide | EPO | EPO+TCM | ➀➁➂➃➄➅ |
| Li and Jin ( | 30 | 30 | Random number table | Coincide | Ferralia | Ferralia+TCM | ➀➁➂ |
| Li ( | 45 | 45 | Random number table | Coincide | EPO | EPO+TCM | ➀➁➂➃ |
| Li et al. ( | 50 | 50 | Randomization | Coincide | Conventional treatment | Conventional treatment+TCM | ➀➁➂➄➉ |
| Liang ( | 75 | 75 | Randomization | Coincide | EPO | EPO+TCM | ➀➁➂ |
| Liu et al. ( | 22 | 22 | Randomization | Coincide | Conventional treatment | Conventional treatment+TCM | ➀➂ |
| Liu et al. ( | 30 | 30 | Random number table | Coincide | Conventional treatment | TCM | ➀➁➂➅➆➇➈➉ |
| Liu and Wang ( | 35 | 35 | Random number table | Coincide | Symptomatic treatment | Symptomatic treatment+TCM | ➀➁➂➃➄➇➈➉ |
| Liu ( | 36 | 36 | Random number table | Coincide | Symptomatic treatment | Symptomatic treatment+TCM | ➀➁➂➄➅ |
| Lou et al. ( | 30 | 30 | Randomization | Coincide | Conventional treatment | Conventional treatment+TCM | ➀➂➄➅ |
| Lu et al. ( | 29 | 26 | Random number table | Coincide | EPO | EPO+TCM | ➀➁ |
| Lu ( | 30 | 30 | Simple randomization | Coincide | Symptomatic treatment | TCM | ➀➁➄➅ |
| Ma ( | 30 | 30 | Random number table | Coincide | Symptomatic treatment | TCM | ➀➂➃➄ |
| Ma ( | 40 | 40 | Randomization | Coincide | Symptomatic treatment | Symptomatic treatment+TCM | ➀➂➃➄ |
| Niu ( | 27 | 27 | Random number table | Coincide | Conventional treatment | TCM | ➀➁➂➃ |
| Peng et al. ( | 40 | 40 | Randomization | Coincide | Symptomatic treatment | TCM | ➀➂➃➆➇➈➉ |
| Qi and Wang ( | 24 | 24 | Random number table | Coincide | Symptomatic treatment | TCM | ➀➁ |
| Qiao ( | 21 | 21 | Randomization | Coincide | Symptomatic treatment | Symptomatic treatment+TCM | ➀➁ |
| Ren and Bie ( | 40 | 40 | Random number table | Coincide | EPO | EPO+TCM | ➀➁➂ |
| She et al. ( | 29 | 30 | Randomization | Coincide | Compound Donkey-hide gelatin slurry | TCM | ➀➂ |
| Song et al. ( | 50 | 50 | Random number table | Coincide | Symptomatic treatment | Symptomatic treatment+TCM | ➀➁➂➃ |
| Sun et al. ( | 56 | 65 | Randomization | Coincide | Symptomatic treatment | TCM | ➀➁➂➆➇➈➉ |
| Tuo ( | 32 | 32 | Random number table | Coincide | EPO | TCM | ➀➁➂➃➄➅➆➇➈➉ |
| Wang ( | 30 | 30 | Randomization | Coincide | EPO | EPO+TCM | ➀➁➂ |
| Wang and Li ( | 40 | 40 | Random number table | Coincide | Symptomatic treatment | TCM | ➀➁➂➃➆➇➈➉ |
| Wang et al. ( | 55 | 55 | Random number table | Coincide | Symptomatic treatment | TCM | ➀➁➂➆➇➈➉ |
| Wang and Li ( | 40 | 40 | Randomization | Coincide | Conventional treatment | TCM | ➀➁➂➄➆➇➈➉ |
| Wang ( | 30 | 30 | Randomization | Coincide | EPO | EPO+TCM | ➀➁➂➄➅➆ |
| Wang et al. ( | 40 | 40 | Random number table | Coincide | EPO | TCM | ➀➁➂➄ |
| Wang ( | 35 | 35 | Random number table | Coincide | EPO | EPO+TCM | ➀➁➃ |
| Wang ( | 38 | 38 | Randomization | Coincide | Symptomatic treatment | Symptomatic treatment+TCM | ➀➁ |
| Wen et al. ( | 30 | 30 | Random number table | Coincide | EPO | EPO+TCM | ➀➁➂ |
| Xu and Long ( | 34 | 34 | Randomization | Coincide | Symptomatic treatment | Symptomatic treatment+TCM | ➀➁➂➅ |
| Yao ( | 45 | 45 | Random number table | Coincide | EPO | EPO+TCM | ➀➁➂➄➆➇➈➉ |
| Yu et al. ( | 34 | 33 | Envelope method | Coincide | EPO | EPO+TCM | ➀➁➂➄ |
| Yu ( | 90 | 90 | Randomization | Coincide | Symptomatic treatment | Symptomatic treatment+TCM | ➀➂➄➅ |
| Zeng ( | 35 | 35 | Random number table | Coincide | Conventional treatment | Conventional treatment+TCM | ➀➁➃➅ |
| Zhang ( | 30 | 30 | Randomization | Coincide | Symptomatic treatment | Symptomatic treatment+TCM | ➀➁ |
| Zhang ( | 28 | 29 | Randomization | Coincide | Conventional treatment | Conventional treatment+TCM | ➀➁➂➃➄➅ |
| Zhao ( | 30 | 30 | Random number table | Coincide | Danggui Buxue decoction | TCM | ➀➁➃➄➅ |
| Zhou ( | 20 | 20 | Randomization | Coincide | EPO | EPO+TCM | ➀➁➄ |
| Outcome measures | Included literature | Bias risk | Inconsistency | Indirect | Uncertainty | Publication bias | Group | Statistical measure (95% CI) | Grading | |
|---|---|---|---|---|---|---|---|---|---|---|
| Control group | Treatment group | |||||||||
| Hemoglobin | 58 | Serious | No | No | No | No | 2157 | 2151 | MD = 11.52, 95% CI [9.21, 13.84] | Middle |
| Clinical efficacy | 49 | Serious | Serious | No | No | No | 1806 | 1794 | OR = 4.46, 95% CI [3.73, 5.33] | Low |
| Red blood cell count | 46 | Serious | Serious | No | No | No | 1809 | 1802 | MD = 0.48, 95% CI [0.36, 0.60] | Low |
| KPS score | 22 | Serious | Serious | No | No | No | 781 | 770 | MD = 7.49, 95% CI [6.21, 8.77] | Low |
| TCM syndrome score | 23 | Serious | Serious | No | No | No | 865 | 859 | MD = −2.36, 95% CI [−3.73, −1.00] | Low |
| TCM syndrome efficacy | 14 | Serious | No | No | No | No | 498 | 494 | OR = 4.61, 95% CI [3.44, 6.16] | Middle |
| CD3+ | 14 | Serious | Serious | No | No | No | 533 | 527 | MD = 5.53, 95% CI [3.77, 7.28] | Low |
| CD4+ | 14 | Serious | Serious | No | No | No | 552 | 546 | MD = 5.39, 95% CI [4.29, 6.50] | Low |
| CD8+ | 14 | Serious | Serious | No | No | No | 552 | 546 | MD = −1.49, 95% CI [−2.40, −0.58] | Low |
| CD4+/CD8+ | 16 | Serious | Serious | No | No | No | 632 | 626 | MD = 0.30, 95% CI [0.22, 0.38] | Low |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsErythropoietin and Anemia Treatment · Plant-based Medicinal Research · Traditional Chinese Medicine Studies
Introduction
1
Cancer related anemia (CRA) is a common complication occurring during the development and treatment of tumors (1). Its primary manifestations include fatigue, pallor, and dizziness. CRA has a high occurrence rate, studies have shown that the incidence of CRA in China reaches 49.24%, and the incidence rises to as high as 90% after chemotherapy. However, the treatment rate remains low, with up to 92.84% of CRA patients receiving no anemia-correcting therapy (2), leading to aggravated anemia symptoms and severely compromised quality of life. Relevant studies indicate that cancer patients with anemia have a 65% increased overall risk of mortality compared to those without anemia (1). CRA is generally induced by multiple factors, including cancer-related factors, and antitumor treatments. Current evidence tends to implicate inflammation, malnutrition, renal impairment, abnormal iron metabolism, and bone marrow hematopoietic dysfunction, among others (3). The main modern medical treatments for CRA include blood transfusion, erythropoiesis-stimulating agents (ESAs), and iron supplementation. Although blood transfusion can rapidly correct blood loss, it carries risks of complications such as infection, hemolysis, and thrombosis (4). According to the 2022 guidelines of the Chinese Society of Clinical Oncology (3), erythropoietin (EPO) therapy has certain limitations and is not recommended, and it exhibits a delayed onset of action, and is effective in only a subset of patients. Iron supplements are only about 10% absorbed by the human body and are often associated with severe gastrointestinal irritation. Traditional Chinese Medicine (TCM) has a long history in the treatment of CRA and offers unique advantages with a favorable safety profile. Therefore, it is of great significance to actively investigate the therapeutic role of TCM in CRA. Although preliminary studies (5, 6) have explored the role of TCM in the treatment of CRA, limitations such as earlier search timeframes, limited database coverage, and insufficient assessment of evidence quality remain. Therefore, this study further updates the search period, incorporates databases including Embase, Scopus, and Web of Science, strictly adheres to the PRISMA guidelines, applies the GRADE approach to grade the quality of evidence, and systematically evaluates the clinical efficacy of oral Chinese herbal medicine in treating CRA. The aim of this study is to provide higher-quality evidence-based support for TCM in the treatment of CRA through a more comprehensive, rigorous, and updated evidence synthesis.
Research methods
2
The study was conducted in strict compliance with the PRISMA guidelines for systematic reviews and meta-analyses.
Literature search
2.1
The literature search strategy was developed in accordance with the Cochrane Systematic Reviews Handbook guidelines. The following databases were searched from their inception to December 2025 for relevant clinical studies on the treatment of CRA with TCM, such as PubMed, Embase, Cochrane Library, Scopus, Web of Science, China National Knowledge Infrastructure (CNKI), China Biology Medicine Disk (CBM), and WanFang. The search terms included “Cancer related anemia,” “Tumor related anemia,” “Anemia,” “Traditional Chinese Medicine,” “Chinese herbal,” “Herbal medicine,” “TCM,” “Randomized” and “RCT.” And the search strategy was adjusted according to different databases. The search strategy takes pubmed as an example: ((((Cancer related anemia) OR (Tumor related anemia)) OR (Anemia)) AND ((((Traditional Chinese Medicine) OR (Chinese herbal)) OR (Herbal medicine)) OR (TCM))) AND ((Randomized[Title/Abstract]) OR (RCT[Title/Abstract])). In addition, we manually searched for relevant studies to obtain as much information as possible. The manual search method is as follows: (1) scanning the reference lists of all included articles and relevant systematic reviews. (2) Searching the trial registries ClinicalTrials.gov, Chinese Clinical Trial Registry, and the International Traditional Medicine Clinical Trial Registry. (3) Reviewing the tables of contents of key Chinese medicine journals (e.g., Zhongguo Za Zhi, Zhongguo Zhong Yao Za Zhi) from the past 10 years.
Inclusion criteria
2.2
(1) Design: randomized controlled trials (RCTs).
(2) Participant: patients with a histologically or cytologically confirmed diagnosis of malignant tumors who also met the diagnostic criteria for anemia.
(3) Interventions: the control group received conventional or symptomatic treatment (e.g., iron supplements, folic acid, EPO, etc.). The treatment group received oral Chinese herbal medicine (either proprietary Chinese medicine or decoction), either as a standalone intervention or in addition to the control group’s regimen.
(4) Outcomes: Primary Outcome: Hemoglobin level (g/L). Secondary Outcomes: Clinical efficacy, Red blood cell count, Karnofsky Performance Status (KPS) score, TCM syndrome score, TCM syndrome efficacy, and immune function indicators (CD3+, CD4+, CD8+, CD4+/CD8+).
(5) Publication: full-text articles published in peer-reviewed journals.
Exclusion criteria
2.3
(1) Conference literature.
(2) Literature from which valid data could not be extracted.
(3) Duplicate publications.
Data extraction
2.4
Two researchers independently screened the literature according to the inclusion and exclusion criteria. Initial screening was performed based on the title, abstract, and keywords, followed by a full-text review for secondary screening. The screening results were cross-checked by both researchers. Any discrepancies were resolved through consultation with a third researcher holding a senior professional title. The primary extracted information including author(s), year of publication, group size, randomization method, interventions, and outcome measures.
Quality assessment criteria
2.5
The Cochrane-recommended risk of bias assessment tool, RoB 2.0, was used to evaluate the quality of the included literature. This assessment covered the following domains: randomization process, deviations from intended interventions, definite outcome indicator, outcome measurement, and selection of the reported result. Two researchers independently performed the risk assessment. Any discrepancies were resolved through consultation with a third researcher.
Statistical analysis
2.6
Meta-analysis of the included literature was performed using RevMan software (version 5.3). Firstly, a heterogeneity testing was conducted for each study. If no statistical significance was observed (P > 0.05, I^2^ < 50%), the included studies were considered to lack heterogeneity, and a fixed-effects model was applied for analysis. Conversely, if statistical significance was present (P < 0.05, I^2^ > 50%), heterogeneity among the included studies was indicated, necessitating further investigation into its sources to determine the suitability of a random-effects model for analysis. For dichotomous data, the odds ratio (OR) with a 95% confidence interval (CI) was used as the statistical measure for efficacy analysis. For continuous data, the mean difference (MD) with a 95% CI was employed as the statistical measure for efficacy analysis.
Results
3
Literature search results
3.1
This study identified 6,201 relevant articles through literature search. After removing 2,786 duplicate records using Note Express software. Subsequent screening of remaining articles through title and abstract analysis removed 3,291 articles. The full texts of the remaining 124 articles were thoroughly reviewed. Finally, according to the inclusion and exclusion criteria, 58 articles were included in the study. See Figure 1.
Flow chart of literature search.
Basic characteristics and quality assessment of included literature
3.2
A total of 58 randomized controlled trials were included in this study, involving 4,308 patients with CRA. Among these patients, 2,157 were assigned to the treatment group and 2,151 to the control group. The baseline characteristics, such as age and gender, were consistent across the included studies, indicating comparability among the study groups. See Table 1.
Among the 58 included clinical studies, 27 studies (7–32) employed random number table for group allocation, 2 studies (33, 34) employed the envelope method, 2 studies (11, 35) used a lottery method, and 2 studies (36, 37) applied simple randomization. The remaining 25 studies (9, 35, 38–62) only mentioned randomization without specifying the method. Additionally, allocation concealment was inadequate in 2 studies (36, 56). Blinding was not mentioned in any of the studies. All studies reported complete outcome data with no selective reporting. See Figures 2, 3.
Risk-of-bias graph.
Risk-of-bias summary.
Meta-analysis results
3.3
Primary outcome measure
3.3.1
Analysis of hemoglobin
3.3.1.1
A total of 58 studies involving 4,308 patients were included. The heterogeneity testing indicated significant heterogeneity among the 58 studies (P < 0.05, I^2^ = 96%), and thus a random-effects model was applied. The meta-analysis demonstrated a statistically significant difference in hemoglobin levels between the two groups (MD = 11.52, 95% CI [9.21, 13.84], P < 0.05). See Figure 4.
Hemoglobin analysis.
Publication bias
3.3.1.2
A funnel plot was constructed for the primary outcome measure. The results demonstrated that the funnel plot was largely symmetrical on both sides, indicating a low likelihood of publication bias in this study. It can be concluded that TCM significantly increases hemoglobin levels and improves anemia in patients. See Figure 5.
Funnel diagram of hemoglobin analysis.
Subgroup analysis
3.3.1.3
A subgroup analysis of hemoglobin levels was performed, with subgroups stratified based on whether conventional treatment involved EPO. The interventions were divided into two subgroups: conventional treatment (excluding EPO) combined with TCM and conventional treatment (including EPO) combined with TCM. The subgroup analysis revealed that the overall results remained consistent regardless of whether EPO was included in the conventional treatment. TCM was identified as the core component of the intervention, suggesting that the study findings are robust. See Figure 6.
Subgroup analysis of hemoglobin.
Secondary outcome measures
3.3.2
Analysis of clinical efficacy
3.3.2.1
A total of 49 studies involving 3,600 patients were included. The heterogeneity testing indicated homogeneity among the 49 studies (P > 0.05, I^2^ = 0%), and thus a fixed-effects model was applied. The meta-analysis demonstrated a statistically significant difference in clinical efficacy between the two groups (OR = 4.46, 95% CI [3.73, 5.33], P < 0.05). See Figure 7.
Clinical effect analysis.
Analysis of red blood cell count
3.3.2.2
A total of 46 studies involving 3,611 patients were included. The heterogeneity testing indicated significant heterogeneity among the 46 studies (P < 0.05, I^2^ = 94%), and thus a random-effects model was applied. The meta-analysis demonstrated a statistically significant difference in red blood cell count between the two groups (MD = 0.48, 95% CI [0.36, 0.60], P < 0.05). See Figure 8.
Red blood cell count analysis.
Analysis of KPS scores
3.3.2.3
A total of 22 studies involving 1,551 patients were included. The heterogeneity testing indicated significant heterogeneity among the 22 studies (P < 0.05, I^2^ = 82%), and thus a random-effects model was applied. The meta-analysis demonstrated a statistically significant difference in KPS scores between the two groups (MD = 7.49, 95% CI [6.21, 8.77], P < 0.05). See Figure 9.
Karnofsky Performance Status (KPS) scores analysis.
Analysis of TCM syndrome score
3.3.2.4
A total of 23 studies involving 1,724 patients were included. The heterogeneity testing indicated significant heterogeneity among the 23 studies (P < 0.05, I^2^ = 97%), and thus a random-effects model was applied. The meta-analysis demonstrated a statistically significant difference in TCM syndrome scores between the two groups (MD = −2.36, 95% CI [−3.73, −1.00], P < 0.05). See Figure 10.
Traditional Chinese Medicine (TCM) syndrome scores analysis.
Analysis of TCM syndrome efficacy
3.3.2.5
A total of 14 studies involving 992 patients were included. The heterogeneity testing indicated homogeneity among the 10 studies (P > 0.05, I^2^ = 0%), and thus a fixed-effects model was applied. The meta-analysis demonstrated a statistically significant difference in TCM syndrome efficacy between the two groups (OR = 4.61, 95% CI [3.44, 6.16], P < 0.05). See Figure 11.
Curative effect analysis of TCM syndromes.
Immune function analysis
3.3.2.6
Analysis of CD3+ cells included 14 studies involving 1,060 patients. The heterogeneity testing indicated significant heterogeneity among the 14 studies (P < 0.05, I^2^ = 83%), and thus a random-effects model was applied. The meta-analysis demonstrated a statistically significant difference in CD3+ levels between the two groups (MD = 5.53, 95% CI [3.77, 7.28], P < 0.05). See Figure 12A. Analysis of CD4+ cells included 14 studies involving 1,098 patients. The heterogeneity testing indicated significant heterogeneity among the 14 studies (P < 0.05, I^2^ = 77%), and thus a random-effects model was applied. The meta-analysis demonstrated a statistically significant difference in CD4+ levels between the two groups (MD = 5.39, 95% CI [4.29, 6.50], P < 0.05). See Figure 12B. Analysis of CD8+ cells included 14 studies involving 1,098 patients. The heterogeneity testing indicated significant heterogeneity among the 14 studies (P < 0.05, I^2^ = 86%), and thus a random-effects model was employed. The meta-analysis demonstrated a statistically significant difference in CD8+ levels between the two groups (MD = −1.49, 95% CI [−2.40, −0.58], P < 0.05). See Figure 12C. Analysis of the CD4+/CD8+ included 16 studies involving 1,258 patients. The heterogeneity testing indicated significant heterogeneity among the 16 studies (P < 0.05, I^2^ = 89%), and thus a random-effects model was applied. The meta-analysis demonstrated a statistically significant difference in the CD4+/CD8+ between the two groups (MD = 0.30, 95% CI [0.22, 0.38], P < 0.05). See Figure 12D.
Immune function analysis (A) CD3+, (B) CD4+, (C) CD8+, (D) CD4+/CD8+.
Grading evidence
3.3.3
A total of 10 outcome indicators were systematically evaluated in this study. None of the included studies involved allocation concealment or blinding, which was rated as a serious risk of bias. The literature included for the Hemoglobin and TCM syndrome efficacy outcomes demonstrated homogeneity, therefore, the inconsistency of the remaining outcome indicators was rated as serious. All outcome indicators were considered direct evidence, with no indirectness present. The data from the literature included in this study were complete, with no selective reporting identified. See Table 2.
Discussion
4
Traditional Chinese Medicine has a long history in the treatment of anemia and possesses unique advantages. CRA falls within the categories of “blood depletion” and “consumptive disease” in TCM, primarily characterized by deficiency of qi and blood. Its disease location is in the spleen and kidney, and it is closely related to the liver. According to TCM theory, in patients with malignant tumors, prolonged illness leads to visceral deficiency, or radiotherapy and chemotherapy consume healthy qi, resulting in dysfunction of the spleen and stomach in transportation and transformation, which consequently leads to insufficient generation and transformation of qi and blood. Additionally, patients often present with qi stagnation, blood stasis, phlegm coagulation, dampness accumulation, and heat toxin, which affect the liver’s function of storing blood, leading to a reduction in blood volume. The kidney stores essence, prolonged illness damages the kidney, leading to kidney essence deficiency and liver blood depletion, which consumes blood and injures essence. Under the combined action of “cancer” and “toxin,” the key pathogenesis characterized primarily by “deficiency” accompanied by “toxin and stasis” is formed (63). Therefore, the treatment principle should focus on tonifying deficiency, combined with resolving toxin and removing stasis.
A total of 48 studies on TCM for the treatment of CRA were included in this analysis. The results demonstrated that the combination of TCM with conventional treatment or the use of TCM alone significantly increased hemoglobin (MD = 11.52, 95% CI [9.21, 13.84], P < 0.05) and improved clinical efficacy (OR = 4.46, 95% CI [3.73, 5.33], P < 0.05) in patients with CRA compared to conventional treatment alone. Improvements were also observed in red blood cell count, KPS score, TCM syndrome score, and TCM syndrome efficacy. Furthermore, TCM treatment exhibited a positive immunomodulatory effect, as indicated by increased proportions of CD3+ and CD4+ T cells and an elevated CD4+/CD8+. Funnel plot analysis of hemoglobin showed approximate symmetry, suggesting a low risk of publication bias and supporting the reliability of the study conclusions. These findings indicate that TCM may provide an effective adjunctive strategy for the comprehensive management of CRA. In addition, some of the included studies compared the safety profiles of TCM and conventional treatment. Overall, conventional treatment for CRA was associated with adverse reactions such as dizziness, headache, abdominal pain, bloating, nausea, vomiting, skin allergies, and even abnormal liver function. In contrast, TCM treatment for CRA not only enhanced clinical efficacy but also resulted in a significantly lower incidence of adverse reactions compared to conventional treatment.
From a modern medical perspective, TCM ameliorates CRA through multi-target mechanisms. The study found that TCM can improve immune function indicators, which is related to its ability to modulate the immunosuppressive state within the tumor microenvironment and mitigate inflammatory responses. Inflammatory responses can lead to anemia by regulating hepcidin, thereby inhibiting iron absorption and release and causing iron metabolism disorders (64). Many TCM herbs for replenishing Qi and nourishing blood possess anti-inflammatory properties, stimulate bone marrow hematopoiesis, and enhance immune function. This aligns with the TCM theory of “fortifying the spleen and tonifying the kidney, replenishing Qi and nourishing blood” for improving CRA and provides further evidential support for the clinical efficacy observations in this study.
The findings of this study are consistent with earlier meta-analyses by Huang et al. (5) and Dang et al. (6), all supporting the positive efficacy of TCM for CRA. However, the study significantly extends and deepens previous meta-analyses in several key aspects. First, the literature search was updated to 2025 and covered multiple international databases, incorporating high-quality clinical studies published in recent years, thereby enhancing the timeliness and comprehensiveness of the evidence. Second, this study strictly adhered to the PRISMA guidelines and, for the first time in a systematic review on this topic, applied the Cochrane RoB 2.0 tool and the GRADE approach to standardize the assessment of evidence quality, making the conclusions of this study more objective and standardized.
Limitations
5
There are some limitations in the application of TCM for CRA. Firstly, the protocol for this systematic review was not prospectively registered, and the number of cases in the literature included in this study was relatively small, and large-sample clinical studies are lacking. Moreover, there is no standardized protocol for treatment duration and observation periods in clinical study. Secondly, variations in participant characteristics across the included studies resulted in significant clinical heterogeneity, which may affect the assessment of therapeutic efficacy. Finally, most studies had a relatively high risk of bias, and two studies included in this study did not adequately implement blinding, which may introduce selection bias, performance bias, and measurement bias (65). Therefore, future large-sample, multicenter, prospective studies are warranted to evaluate the clinical efficacy of TCM in treating CRA, with the aim of providing higher-quality medical evidence.
Conclusion
6
In summary, current clinical evidence indicates that as an effective complementary therapy for CRA, TCM can safely and effectively improve hemoglobin, immune function, clinical symptoms, and quality of life in patients with CRA. In clinical practice, for CRA patients who respond poorly to conventional treatments or cannot tolerate its side effects, considering the combined use of TCM under the guidance of TCM syndrome differentiation by a qualified TCM practitioner represents a reasonable therapeutic option. However, given the overall low certainty of the current evidence, it is presently insufficient to formulate a strong recommendation for the routine inclusion of TCM in CRA treatment guidelines. The primary value of this study lies in systematically reviewing the existing evidence, clarifying its strengths and limitations, and providing direction for future pivotal research aimed at generating higher-level evidence.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Avancini A Belluomini L Tregnago D Trestini I Milella M Lanza M Exercise and Anemia in cancer patients: could it make the difference? Expert Rev Hematol. (2021) 14:979–85. 10.1080/17474086.2021.200776434784852 · doi ↗ · pubmed ↗
- 2Song ZB Lu S Feng JF Xu JM Liu YP Liu W Epidemiological investigation on the incidence and treatment status of cancer-related anemia in China. Chin J Oncol. (2019) 28:718–22.
- 3Chinese Society of Clinical Oncology Guidelines Working Committee Chinese Society of Clinical Oncology (CSCO) Clinical Practice Guidelines for Cancer-Related Anemia 2022. Beijing: People’s Medical Publishing House (2022).
- 4Chen Y Li YL Zhou ZP Pu SM. Causes of cancer-related anemia. Chem J Life. (2021) 41:1747–53. 10.13488/j.smhx.20210092 · doi ↗
- 5Dang Z Liu X Wang X Li M Jiang Y Wang X Comparative effectiveness and safety of traditional Chinese medicine supporting Qi and enriching blood for cancer related anemia in patients not receiving chemoradiotherapy: a meta-analysis and systematic review. Drug Des Devel Ther. (2018) 13:221–30. 10.2147/DDDT.S 181182 PMC 631269230643388 · doi ↗ · pubmed ↗
- 6Huang MN Jia YJ Chen J Li XJ Lin LS. Meta-analysis of the efficacy of traditional Chinese medicine in the treatment of cancer-related anemia. Chin J Integr Trad Western Med Surg. (2017) 23:343–8.
- 7Cong SD. The impact of modified Chinese herbal medicine Danggui Buxue Decoction on the prognosis of patients with chemotherapy-induced anemia caused by tumors. Inner Mongol J Trad Chin Med. (2025) 44:40–2. 10.16040/j.cnki.cn 15-1101.2025.08.026 · doi ↗
- 8Feng JL Wu DP He B. Efficacy of Shenqi Yangxue granules in treating tumor-related anemia and its impact on immune function. Liaon J Trad Chin Med. (2024) 51:91–4. 10.13192/j.issn.1000-1719.2024.04.025 · doi ↗