Real-world effectiveness and safety of Sacituzumab Govitecan in metastatic triple-negative breast cancer: results from the multicenter retrospective observational SACISUR cohort in Southern Spain
Alejandro Falcón-González, Elisenda Llabrés-Valenti, Fernando Henao-Carrasco, Rocío Urbano-Cubero, Ana Godoy-Ortiz, Julio César Nieto-Ramírez, Ana Milena Vargas-Prado, Alba González-Haba, Braulio Martín-Calero, Cristina Morales-Estévez, María Valero-Arbizu

TL;DR
This study evaluates the real-world effectiveness and safety of Sacituzumab Govitecan in treating metastatic triple-negative breast cancer in Southern Spain.
Contribution
The study provides real-world data on Sacituzumab Govitecan's effectiveness and safety in metastatic triple-negative breast cancer patients, including those with CNS metastases.
Findings
Median progression-free survival was 4.6 months and overall survival was 10.9 months in mTNBC patients.
Patients with CNS metastases had a median progression-free survival of 2.3 months.
Neutropenia and diarrhea were the most common adverse events, with manageable safety profile overall.
Abstract
Sacituzumab govitecan (SG) has demonstrated efficacy in metastatic triple-negative breast cancer (mTNBC) in clinical trials, but real-world data from routine clinical practice remains limited. This study aimed to evaluate the effectiveness and safety of SG in mTNBC patients in Southern Spain. This observational, multicenter, retrospective study included 159 mTNBC patients who received at least one cycle of SG between January 2022 and December 2023. Primary endpoints included real-world progression-free survival (rwPFS), overall survival (rwOS), and safety. Secondary endpoints explored treatment tolerability and management of adverse events. A pre-specified subset analysis focused on patients with central nervous system (CNS) metastases. The median age of patients at diagnosis was 50 years (46.5% premenopausal). Median rwPFS was 4.6 months (95% CI 3.7-6.3) and rwOS was 10.9 months (95%…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
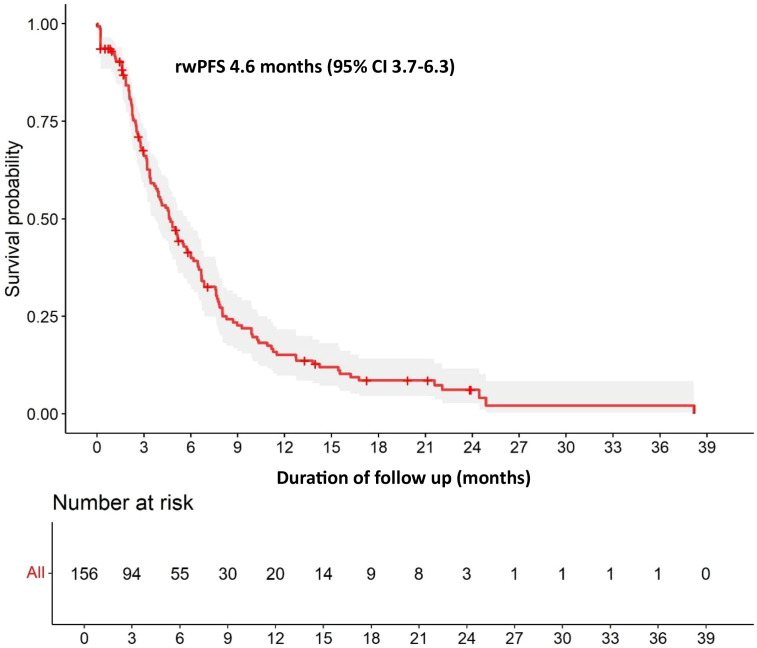 Figure 1
Figure 1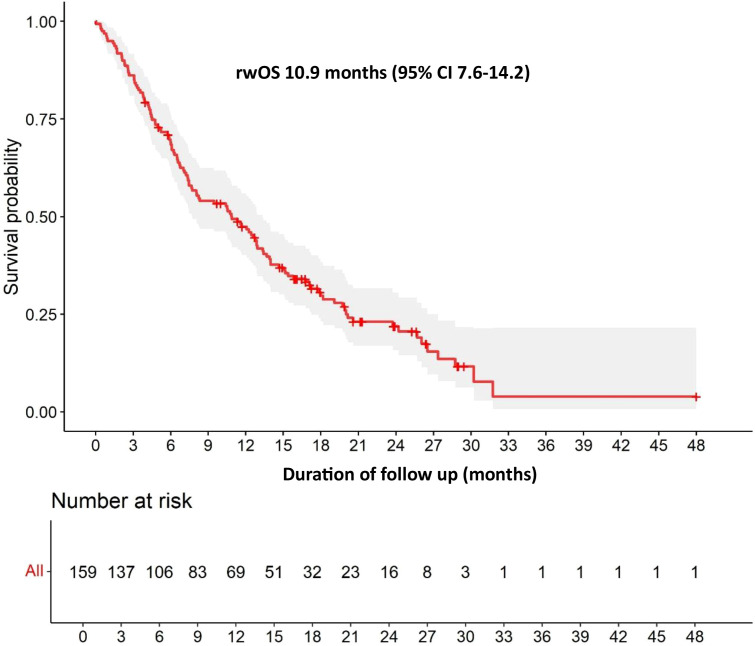 Figure 2
Figure 2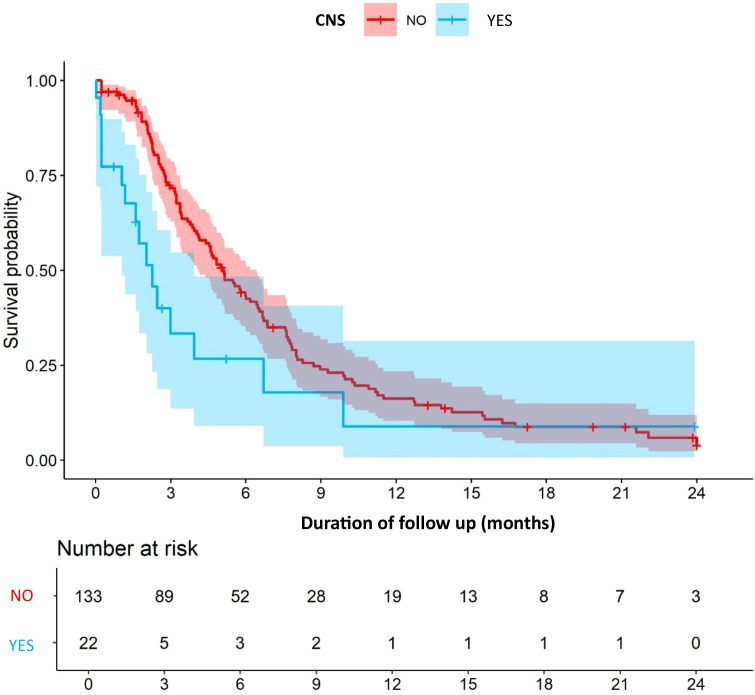 Figure 3
Figure 3| Characteristic | Overall population N (%) | Cohort with CNS metastases N (%) |
|---|---|---|
| N | 159 | 22 |
| Age, median (IQR), y | 50 (21-77) | 45 (30-67) |
| ECOG | ||
| 0 | 61.6% | 63.6% |
| 1 | 31.4% | 22.7% |
| 2 | 5.7% | 9.1% |
| 3 | 1.3% | 4.5% |
| Premenopausal | 74 (46.5%) | 11 (50.0%) |
| Ductal histology | 134 (84.3%) | |
| HER2 status | ||
| HER2 0 | 96 (60.4%) | 11 (50.0%) |
| HER2 low | 56 (35.2%) | 11 (50.0%) |
| Visceral metastases at baseline | 120 (75.5%) | 21 (95.2%) |
| CNS disease | 22 (13.8%) | 22 (100.0%) |
| Disease stage at diagnosis, N (%) | ||
| Recurrent disease | 0 | 0 |
| 28 (17.6%) | 5 (22.7%) | |
| Localized or stage I-III | 129 (81.1%) | 17 (77.3%) |
| Previous line of therapy, median (IQR) | 3 (2-8) | 2.4 (2-4) |
| SG third-line or beyond | 86 (54.1%) | 7 (31.8%) |
| SG second-line | 66 (41.5%) | 15 (68.2%) |
| SG first-line | 6 (3.8%) | 0 (0%) |
| SG cycles, median (IQR) | 7.9 (1-52) | 4.68 (1-27) |
| Neoadjuvant chemotherapy in early disease | 97 (61.0%) | 13 (59.1%) |
| pCR | 17 (17.5%)1 | 12 (54.5%)2 |
| Immunotherapy | 7 (4.4%) | |
| Immunotherapy in first-line | 27 (17.0%) | 4 (18.2%) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAdvanced Breast Cancer Therapies · HER2/EGFR in Cancer Research · Cancer Treatment and Pharmacology
Introduction
Triple-negative breast cancer (TNBC) - an aggressive molecular subtype defined by the absence of estrogen receptor (ER), progesterone receptor (PR), and human epidermal growth factor receptor 2 (HER2) expression – accounts for 15%-20% of invasive breast carcinomas (1, 2). This biologically heterogeneous malignancy exhibits a clinically aggressive phenotype with a poor prognosis (3), and median overall survival is limited to 12–18 months despite therapeutic advances (4). The absence of actionable targets, such as hormone receptors or HER2 overexpression, excludes the use of endocrine therapies and HER2-directed treatments, positioning cytotoxic chemotherapy as the predominant therapeutic approach for the majority of advanced cases.
Sacituzumab govitecan (SG) emerged as a therapeutic breakthrough following its April 2020 FDA accelerated approval for metastatic triple-negative breast cancer (mTNBC) refractory to ≥2 prior systemic therapies, including at least one for advanced disease. Full approval was obtained in 2021, and it is currently authorized in patients with pre-treated HR+/HER2- metastatic breast cancer. This antibody-drug conjugate (ADC) uses a humanized monoclonal antibody (hRS7 IgG1κ) to target trophoblast cell-surface antigen-2 (Trop-2) coupled to SN-38 – the active metabolite of irinotecan – though a hydrolysable CL2A linker. Upon Trop-2-mediated internalization, enzymatic cleavage releases SN-38, inducing topoisomerase I inhibition, DNA double-strand breaks, and subsequent apoptosis. SG demonstrated remarkable efficacy in this pretreated patient population in which most had received two to three prior lines of chemotherapy.
In the ASCENT trial (5), a total of 529 patients with triple-negative breast cancer were enrolled between November 2017 and September 2019 at 88 sites in 7 countries and were randomly assigned in a 1:1 ratio to receive SG or single-agent chemotherapy, with 61 patients with stable brain metastases (stable for at least 4 weeks before treatment) at baseline. Patients achieved median progression-free survival (PFS) of 4.8 vs 1.7 months (HR 0.41) and overall survival (OS) of 11.8 vs 6.9 months (HR 0.48) with SG or single-agent chemotherapy, respectively. The clinical impact of SG extends beyond TNBC, as evidenced by the TROPiCS-02 trial (6) in patients with hormone receptor-positive (HR+) and luminal HER2-negative locally recurrent inoperable or metastatic breast cancer, where it extended median overall survival to 14.4 months versus 11.2 months with standard chemotherapy (p = 0.020). Crucially, survival benefits occurred irrespective of Trop-2 expression levels, highlighting the broad efficacy of this therapeutic approach. These patients had received at least one previous endocrine therapy, a taxane, and a CDK4/6 inhibitor in any setting, along with 2 to 4 previous chemotherapy regimens for metastatic disease.
The imperative for real-world data in oncology arises from its unique capacity to validate therapeutic interventions across unselected patient populations and routine clinical practice – a critical consideration for mTNBC, where rapid disease evolution and therapeutic scarcity call for urgent insights beyond protocol-restricted trial cohorts. For this reason, the primary objective of this study was to characterize the clinical and demographic profile of patients with mTNBC receiving SG in a routine clinical practice setting in Southern Spain. Key endpoints included effectiveness, measured as real-world progression-free survival (rwPFS) and overall survival (rwOS), alongside an analysis of the safety profile, particularly the management of neutropenia and diarrhea. Treatment management patterns, including dose modifications and supportive care strategies, were also assessed. Special emphasis was placed on subpopulations, such as patients with brain metastases, given their exclusion from pivotal clinical trials and their distinct clinical challenges.
Methods
Study design and population
This was an observational, multicenter, retrospective cohort study conducted across healthcare institutions in Southern Spain as part of the SACISUR cohort study. We included patients with mTNBC who received at least one cycle of SG between January 1, 2022, and December 31, 2023. For inclusion, patients had to present TNBC according to standard American Society of Clinical Oncology–College of American Pathologists criteria (7) determined at the time of the most recent available biopsy. If a metastatic biopsy specimen was available, TNBC status was defined based on this sample; otherwise, the receptor status at initial diagnosis was used. Disease classification was based on the timing and extent of metastatic involvement at initial diagnosis. De novo stage IV disease was defined as patients presenting with metastatic disease (classified as stage IV according to the American Joint Committee on Cancer TNM staging criteria) within 3 months of their initial breast cancer diagnosis. Relapse after early stage was defined as patients initially diagnosed with non-metastatic breast cancer (stages I-III) with no evidence of distant metastases who had relapsed after surgery. Menopausal status was assessed based on clinical and laboratory parameters documented in the patient’s medical records. Premenopausal status was defined as women with regular menstrual cycles or amenorrhea for less than 12 months before receiving chemotherapy. Patients who had undergone bilateral oophorectomy were classified as postmenopausal regardless of age. Those with hysterectomy but preserved ovaries were classified based on age and hormonal parameters, if available.
Data collection included patient demographics, clinical characteristics, treatment patterns, adverse events, and survival outcomes.
Data analysis
As this was an exploratory study with a descriptive aim of collecting, summarizing, and providing data on routine clinical management and outcomes in patients with mTNBC treated with SG, no prespecified hypothesis was made; therefore, sample size was not estimated.
Descriptive statistical analysis was performed on all study variables. For quantitative variables, measures of central tendency and dispersion were calculated (mean and standard deviation [SD]; median and interquartile ranges [IQR]). For qualitative variables frequencies and percentages were reported.
Data collected from medical records included: date of initial diagnosis, Eastern Cooperative Oncology Group (ECOG), histology, menopausal status, tumor grade, tumor stage, visceral involvement as well as CNS involvement, HR-negative or HR positive, HER2 intensity (0 vs low 1+ or 2+ with ISH negative), Ki-67 and BRCA status. Related to previous treatment we also included neo- or adjuvant therapy in early disease, previous treatments for advanced disease, and the associated response to each treatment.
Time-to-event endpoint analysis (rwPFS and rwOS) were estimated using the Kaplan-Meier method and compared between groups using the log rank test (Mantel-Cox), with supporting tests including Breslow (generalized Wilconxon) and Tarone-Ware tests for robustness verification. Median survival times with 95% confidence intervals (CI) were reported. rwPFS was defined as time from SG initiation until objective tumor progression or death or was censored at the last radiographic assessment in the case of patients without progression or death, while rwOS was calculated from treatment initiation to death from any cause. Patients without events were censored at the date of the last follow-up. The objective response rate (ORR) was assessed per investigator according to Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1 (8), defined as the proportion of patients achieving either complete response (CR) or partial response (PR) as their best overall response, based on radiological assessments performed at regular intervals in accordance with institutional standards of care. The disease control rate (DCR) was defined as the proportion of patients achieving either an objective response (CR or PR) or stable disease lasting at least 6 months, as determined by radiological assessments performed according to institutional guidelines and evaluated using RECIST v1.1 criteria (8). A pre-specified subset analysis was performed on patients with central nervous system (CNS) metastases, a high-risk population typically underrepresented in clinical trials, to evaluate treatment outcomes in this specific subgroup of interest.
Missing data was not considered in the analyses. Statistical analyses were conducted using two statistical software packages: IBM SPSS Statistics version 31.0 and R version 4.x (R Foundation for Statistical Computing, Vienna, Austria). All R code was documented for reproducibility.
Ethics approval
The study was conducted in accordance with the principles of the Declaration of Helsinki and approved by the Ethics Committee of Virgen Macarena University Hospital (Meeting 26/05/2023, ACTA 11/2023). All patient data were anonymized and processed according to applicable data protection regulations. All patients included in this retrospective observational study had previously provided general consent for the use of their clinical data in research studies as part of their standard care documentation.
Results
Patient characteristics
A total of 159 patients with mTNBC were included in this study. The median age at diagnosis was 50 years (range 21-77); 74 (46.5%) patients were premenopausal. The majority of patients (93.0%) had an ECOG performance status of 0–1 at treatment initiation. Regarding disease characteristics, 81.1% presented with initial localized stage I-III metastatic disease, while 17.6% had de novo stage IV. The median number of previous lines of therapy was 3 (range 2-8), with patients receiving a median of 7.9 cycles of SG. SG was administered as third-line or beyond in 86 (54.1%) patients, as second-line therapy in 66 (41.5%) patients, and as first-line therapy in 6 (3.8%) patients; 17% of patients had received immunotherapy as first-line treatment (Table 1).
Twenty-two study patients (13.8%) had CNS metastases at the time of SG initiation. The median age of this population was 45 years (range 30-67). This subgroup demonstrated a higher proportion of visceral disease involvement (95.2% vs 75.5% in the overall population) and a more extensive metastatic profile, with a higher proportion of de novo stage IV disease (22.7% vs 17.6% in the overall cohort). All had been treated with radiotherapy prior to SG (Table 1).
Effectiveness
With a median follow-up of 11.6 months in the overall population, the median rwPFS was 4.6 months (95% CI 3.7-6.3) (Figure 1) and the median rwOS was 10.9 months (95% CI 7.6-14.2) (Figure 2). The ORR (CR or PR) was 31.2%, with a DCR (stable disease or objective response) of 68.9%.
Overall rwPFS. rwPFS, real-world Progression-Free Survival.
Overall rwOS. rwOS, real-world Overall Survival.
In patients with CNS metastases at baseline, the median follow-up was 6.0 months, during which the median rwPFS was 2.3 months (95% CI, 1.3–3.2) vs 5.1 months (95% CI, 4.1–5.9) in patients without CNS metastases (Figure 3). The ORR in this subgroup was 13.6%, with a DCR of 36.3%.
CNS metastases stratified rwPFS. CNS, central nervous system; rwPFS, Real-World Progression-Free Survival.
Safety profile
SG was associated with diverse adverse events. Neutropenia was the most common, occurring in 59.4% of patients, with 30.4% experiencing grade 3–4 severity. Diarrhea affected 49.0% of patients, with 8.2% reporting grade 3–4 events. Nausea was observed in 45.3% of patients, although only 0.6% presented severe (grade 3-4) nausea. Elevation of liver enzymes (ALT/AST) was noted in 24.5% of patients, with 1.9% experiencing grade 3–4 elevations.
Granulocyte colony-stimulating factor (G-CSF) was administered as primary prophylaxis in 29.6% of patients and as secondary prophylaxis in 17.6%. Treatment discontinuation due to adverse events occurred in 5.7% of patients, while 43.4% required at least one dose reduction during their treatment.
In patients with CNS metastases, the most prevalent side effect of SG was also neutropenia, which occurred in 45.5% of patients, of which 27.2% experienced grade 3–4 severity. Diarrhea affected 36.8% of patients, with 9.1% reporting grade 3–4 events. Nausea was observed in 21.1% of patients, with 5.3% reporting grade 3–4 severity. Elevation of liver enzymes (ALT/AST) was noted in 30% of patients, although no grade 3–4 elevations were reported.
G-CSF was administered as primary prophylaxis in 18.2% of patients and as secondary prophylaxis in an additional 18.2%. Notably, no patients discontinued treatment due to adverse events, although 31.8% required at least one dose reduction during their treatment.
Discussion
The results of our multicenter retrospective cohort have shown that SG is a safe and effective treatment option for patients with mTNBC in clinical practice. Our findings closely align with those of the pivotal ASCENT trial, even though our cohort included a broader patient population with potentially worse prognostic factors. The median rwPFS of 4.6 months and rwOS of 10.9 months observed in our study were comparable with the ASCENT trial results (median PFS 4.8 months, OS 11.8 months). Our ORR of 31.2% and DCR of 68.9% were in line with ASCENT’s ORR of 35% and DCR of 45%, suggesting preserved efficacy of SG in real-world settings. However, patients with CNS metastases demonstrated inferior survival outcomes, with a median rwPFS of 2.3 months compared with 5.1 months in patients without CNS involvement. This consistency with ASCENT is particularly noteworthy given our broader inclusion criteria, which encompassed patients with active brain metastases and poorer performance status. The slight differences in survival outcomes may be attributed to the inherent heterogeneity of real-world patient populations. For example, in our cohort 13.8% of patients presented CNS metastases, a subgroup that demonstrated inferior outcomes with a median rwPFS of 2.3 months. Other studies using real-world data have also reported similar results to those observed in clinical trials (9–12).
Our ORR and DCR compare favorably to those reported in ASCENT’, suggesting that the efficacy of SG is preserved, if not enhanced, in real-world clinical practice. The higher DCR in our study might reflect the potential for longer-term disease stabilization in a less strictly selected patient population. The consistency of these results across different studies based on routine clinical practice further supports the effectiveness of SG. For example, a retrospective analysis presented at the 42^nd^ Annual Miami Breast Cancer Conference (13) reported a median rwPFS of 5.0 months and rwOS of 11.3 months in patients receiving SG in the second-line or later setting, closely mirroring our findings and those of ASCENT (5).
A notably lower incidence of neutropenia was observed in our cohort compared with pivotal clinical trials. This reason for this is likely multifactorial: first, the use of primary prophylactic G-CSF was more common in our cohort, a strategy supported by recent data showing that prophylactic growth factor administration significantly reduces both the incidence and severity of SG-related neutropenia (14); second, recording neutropenia on day 8 of each cycle allowed clinicians to individualize each assessment and take timely action, such as delaying treatment or administering G-CSF to further reduce the risk and impact of neutropenic events (15).
This study has several strengths and limitations. Among the strengths, the multicenter, real-world design improves the generalizability of our findings across diverse healthcare settings in Southern Spain, providing valuable insights into the effectiveness and safety of SG in a broader patient population than typically included in clinical trials. The inclusion of patients with brain metastases, often excluded from pivotal trials, offers crucial data on this challenging subgroup. However, some limitations must also be mentioned, including the study’s retrospective design, which introduces potential biases in data collection and interpretation. The lack of stratification between stable and active brain metastases limits the granularity of the conclusions that can be drawn from this subpopulation. Additionally, the absence of a control group precludes direct comparisons with alternative treatments, and the relatively short follow-up period may not capture long-term outcomes or rare adverse events.
Conclusion
In conclusion, this study demonstrates that SG shows clinically meaningful activity and is generally well-tolerated in patients with mTNBC treated in routine clinical practice. The efficacy outcomes, including median rwPFS of 4.6 months and rwOS of 10.9 months, closely mirror those observed in the pivotal ASCENT trial, despite the inclusion of patients with potentially worse prognostic factors such as active brain metastases and poorer performance status. The comparable ORR and higher DCR further support the preserved efficacy of SG in real-world settings. The study also highlights the challenges involved in treating patients with CNS metastases – a subgroup with inferior survival outcomes. However, the drug is considered both effective and safe in the treatment of this patient group.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Obidiro O Battogtokh G Akala EO . Triple negative breast cancer treatment options and limitations: future outlook. Pharmaceutics. (2023) 15:1796. doi: 10.3390/pharmaceutics 15071796, PMID: 37513983 PMC 10384267 · doi ↗ · pubmed ↗
- 2Xiong N Wu H Yu Z . Advancements and challenges in triple-negative breast cancer: a comprehensive review of therapeutic and diagnostic strategies. Front Oncol. (2024) 14:1405491. doi: 10.3389/fonc.2024.1405491, PMID: 38863622 PMC 11165151 · doi ↗ · pubmed ↗
- 3Huppert LA Gumusay O Rugo HS . Emerging treatment strategies for metastatic triple-negative breast cancer. Ther Adv Med Oncol. (2022) 14:17588359221086916. doi: 10.1177/17588359221086916, PMID: 35422881 PMC 9003656 · doi ↗ · pubmed ↗
- 4Jacobs F Agostinetto E Miggiano C De Sanctis R Zambelli A Santoro A . Hope and hype around immunotherapy in triple-negative breast cancer. Cancers (Basel). (2023) 15:2933. doi: 10.3390/cancers 15112933, PMID: 37296893 PMC 10252021 · doi ↗ · pubmed ↗
- 5Bardia A Hurvitz SA Tolaney SM Loirat D Punie K Oliveira M . Sacituzumab govitecan in metastatic triple-negative breast cancer. N Engl J Med. (2021) 384:1529–41. doi: 10.1056/NEJ Moa 2028485, PMID: 33882206 · doi ↗ · pubmed ↗
- 6Rugo HS Bardia A MarméF Cortés J Schmid P Loirat D . Overall survival with sacituzumab govitecan in hormone receptor-positive and human epidermal growth factor receptor 2-negative metastatic breast cancer (TRO Pi CS-02): a randomised, open-label, multicentre, phase 3 trial. Lancet. (2023) 402:1423–33. doi: 10.1016/S 0140-6736(23)01245-X, PMID: 37633306 · doi ↗ · pubmed ↗
- 7Hammond MEH Hayes DF Dowsett M Allred DC Hagerty KL Badve S . American Society of Clinical Oncology/College Of American Pathologists guideline recommendations for immunohistochemical testing of estrogen and progesterone receptors in breast cancer. J Clin Oncol. (2010) 28:2784–95. doi: 10.1200/JCO.2009.25.6529, PMID: 20404251 PMC 2881855 · doi ↗ · pubmed ↗
- 8Eisenhauer EA Therasse P Bogaerts J Schwartz LH Sargent D Ford R . New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur J Cancer. (2009) 45:228–47. doi: 10.1016/j.ejca.2008.10.026, PMID: 19097774 · doi ↗ · pubmed ↗