Early Identification of Cardiovascular Adverse Events Associated With Rofecoxib Using Real‐World Data From the UK: A Nested Case–Control and Case‐Crossover Study
Donya Moslemzadeh, Patrick C. Souverein, Svetlana V. Belitser, Eibert R. Heerdink, Olaf H. Klungel, Shahab Abtahi

TL;DR
Using UK real-world data, researchers found that rofecoxib's heart risks could have been detected two years after it was sold, much faster than traditional methods.
Contribution
This study shows real-world data can detect drug risks faster than traditional methods, using novel nested case–control and case–crossover designs.
Findings
Rofecoxib's cardiovascular risks were detectable 2 years after market entry using real-world data.
Case-crossover design detected the risk earlier than nested case–control design.
Real-world data analysis can improve drug safety monitoring and detect adverse events sooner.
Abstract
Traditional pharmacovigilance systems have limitations in detecting common adverse drug reactions. We investigated whether real‐world data (RWD) could have detected rofecoxib's cardiovascular adverse effects earlier using nested case–control (NCC) and case‐crossover (CCO) designs. We included adult rofecoxib users from the UK CPRD GOLD (1999–2004). In NCC design, cases of a first major adverse cardiovascular event (MACE) were matched with four controls on age, sex, practice and calendar time. Rofecoxib exposure was categorised as current (≤ 3 months), recent (3–6), or past use (> 6) in NCC, and assessed at the start of each 3‐month interval in CCO design. Exposure odds in CCO were compared between a 3‐month risk with four reference windows. Conditional logistic regression models estimated adjusted intensity ratio (aIR). To identify the shortest time necessary to detect the association,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
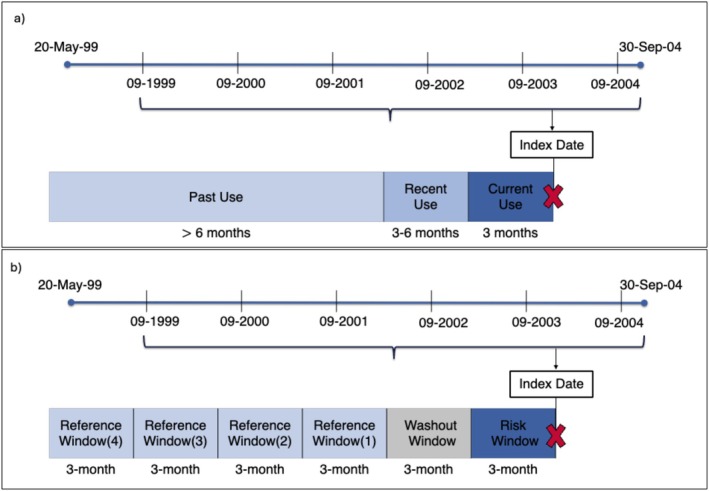 FIGURE 1
FIGURE 1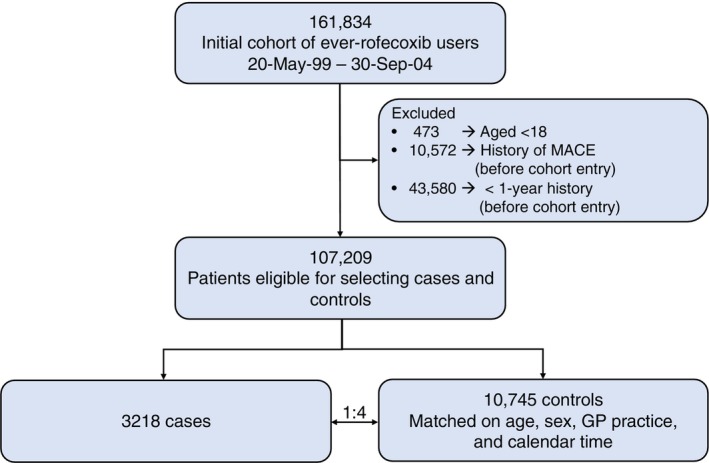 FIGURE 2
FIGURE 2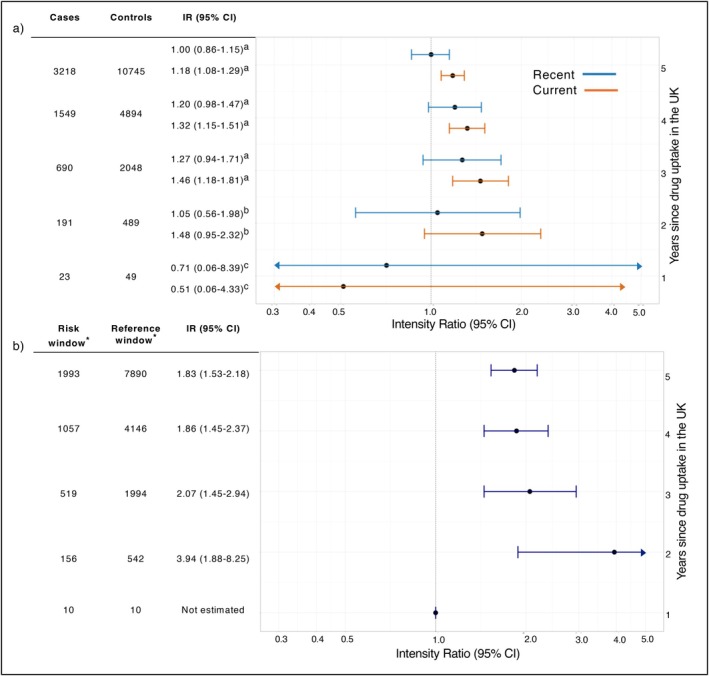 FIGURE 3
FIGURE 3| Characteristics | Cases (% or ±SD) | Controls (% or ±SD) |
|---|---|---|
| Total number | 3218 | 10 745 |
| Sex | ||
| Men | 1103 (34.3%) | 3444 (32.1%) |
| Women | 2115 (65.7%) | 7301 (67.0%) |
| Mean age in years (±SD) | 73.8 (±10.8) | 72.9 (±10.4) |
| Age groups | ||
| 18–49 | 83 (2.6%) | 271 (2.5%) |
| 50–64 | 527 (16.4%) | 1951 (18.2%) |
| 65–79 | 1506 (46.8%) | 5336 (49.7%) |
| 80+ | 1102 (34.2%) | 3187 (29.7%) |
| Mean BMI (±SD) (at index date) | 27.7 (±5.5) | 27.3 (±5.3) |
| BMI categories | ||
| < 20.0 | 156 (4.9%) | 485 (4.5%) |
| 20.0–24.9 | 777 (24.2%) | 2834 (26.4%) |
| 25.0–29.9 | 1081 (33.6%) | 3833 (35.7%) |
| 30.0–34.9 | 565 (17.6%) | 1811 (16.9%) |
| ≥ 35.0 | 281 (8.7%) | 741 (6.9%) |
| Missing | 358 (11.1%) | 1041 (9.7%) |
| Smoking status (at index date) | ||
| Never | 1170 (36.4%) | 4449 (41.4%) |
| Current | 511 (15.9%) | 1580 (14.7%) |
| Former | 1446 (44.9%) | 4471 (41.6%) |
| Missing | 91 (2.8%) | 245 (2.3%) |
| Healthcare utilisation (±SD) | 15 (±12.2) | 12 (±9.5) |
| Main indications | ||
| Backpain | 1659 (51.6%) | 5234 (48.7%) |
| Osteoarthritis | 2271 (70.6%) | 7309 (68.0%) |
| Rheumatoid arthritis | 231 (7.2%) | 601 (5.6%) |
| Comorbidities (ever before index date) | ||
| Alcohol abuse | 83 (2.6%) | 229 (2.1%) |
| Cardiovascular disease | 1395 (43.4%) | 3099 (28.8%) |
| Chronic kidney disease | 92 (2.9%) | 177 (1.7%) |
| Chronic liver disease | 14 (0.4%) | 26 (0.2%) |
| Chronic respiratory disease | 559 (17.4%) | 1649 (15.4%) |
| Diabetes (type 2) | 410 (12.7%) | 814 (7.6%) |
| Dysmenorrhea | 19 (0.6%) | 75 (0.7%) |
| Hyperlipidaemia | 363 (11.3%) | 926 (8.6%) |
| Hypertension | 1350 (42.0%) | 3878 (36.1%) |
| Malignancies (excluding non‐melanoma skin cancers) | 417 (13.0%) | 1382 (12.9%) |
| Migraine | 195 (6.1%) | 576 (5.4%) |
| Co‐medications (3 months before index date) | ||
| ACE inhibitors and ARBs | 890 (27.7%) | 1894 (17.6%) |
| Aspirin | 948 (29.5%) | 1927 (17.9%) |
| Beta blockers | 640 (19.9%) | 1733 (16.1%) |
| Calcium channel blockers | 625 (19.4%) | 1664 (15.5%) |
| Corticosteroids | 334 (10.4%) | 755 (7.0%) |
| Digoxin and other glycosides | 158 (4.9%) | 195 (1.8%) |
| Diuretics | 1392 (43.3%) | 3399 (31.6%) |
| HRT | 129 (4.0%) | 470 (4.4%) |
| Immunosuppressants | 78 (2.4%) | 170 (1.6%) |
| Lipid lowering agents | 621 (19.3%) | 1389 (12.9%) |
| Nitrates | 397 (12.3%) | 662 (6.2%) |
| NSAIDs (other than rofecoxib) | 699 (21.7%) | 2400 (22.3%) |
| Platelet aggregation inhibitors | 172 (5.3%) | 161 (1.5%) |
| Vasodilators | 6 (0.2%) | 8 (0.1%) |
| MACE cases (% total) | Controls (% total) | Crude IR (95% CI) | Adjusted IR | |
|---|---|---|---|---|
| Total | 3218 | 10 745 | ||
| Rofecoxib exposure | ||||
| Past use | 1533 (47.6%) | 5532 (51.5%) | Reference | |
| Current use | 1350 (42.0%) | 4025 (37.5%) | 1.18 (1.08–1.29) | 1.18 (1.08–1.29) |
| Recent use | 335 (10.4%) | 1188 (11.1%) | 1.01 (0.88–1.15) | 1.00 (0.86–1.15) |
| Dose–response (among current users) | ||||
| < 25 mg | 768 (23.9%) | 2267 (21.1%) | 1.16 (1.05–1.29) | 1.19 (1.06–1.32) |
| ≥ 25 mg | 582 (18.1%) | 1758 (16.4%) | 1.21 (1.08–1.36) | 1.17 (1.04–1.32) |
| Duration‐response (among current users | ||||
| ≤ 1 month | 397 (12.3%) | 1376 (12.8%) | 1.02 (0.90–1.17) | 1.05 (0.91–1.20) |
| 1–3 months | 319 (9.9%) | 1015 (9.5%) | 1.09 (0.95–1.26) | 1.12 (0.96–1.30) |
| 3–6 months | 247 (7.7%) | 646 (6.0%) | 1.34 (1.14–1.57) | 1.28 (1.08–1.52) |
| > 6 months | 542 (16.8%) | 1514 (14.1%) | 1.27 (1.13–1.43) | 1.25 (1.11–1.42) |
| Rofecoxib exposure windows | Risk window | Reference windows | Adjusted IR | ||
|---|---|---|---|---|---|
| Total | Exposed | Total | Exposed | ||
| Main analysis | |||||
| 3‐month | 3210 | 1344 (41.9%) | 12 737 | 3700 (29.1%) | 1.83 (1.53–2.18) |
| Sensitivity analyses | |||||
| 1‐month | 3218 | 825 (25.6%) | 12 858 | 2746 (21.4%) | 1.46 (1.26–1.71) |
| 6‐month | 3180 | 1650 (51.9%) | 11 915 | 3324 (27.1%) | 1.83 (1.44–2.32) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPharmacovigilance and Adverse Drug Reactions · Inflammatory mediators and NSAID effects · Forensic Toxicology and Drug Analysis
Introduction
1
Rofecoxib, a selective COX‐2 inhibitor, was withdrawn from the market in 2004 due to cardiovascular adverse events [1]. During its marketing period (May 1999–September 2004), over 80 million patients used rofecoxib worldwide [2]. The Adenomatous Polyp Prevention on Vioxx (APPROVe) trial [3, 4], revealed 16 excess myocardial infarction (MI) or stroke events per 1000 patients without cardiovascular disease history [2], potentially translating to 1.3 million additional major adverse cardiovascular events (MACE) globally during rofecoxib's marketing period.
Approximately 4% of newly introduced drugs are eventually withdrawn from the market due to serious adverse effects not detected during pre‐marketing trials [5]. While pre‐authorisation clinical trials aim to identify potential risks, certain adverse reactions only emerge when medications are used in larger, more diverse populations over extended periods. This highlights the importance of effective post‐market surveillance. Current pharmacovigilance primarily relies on post‐authorisation spontaneous reporting systems (SRSs), where patients and healthcare professionals report suspected adverse events to pharmacovigilance centres. However, SRSs have significant limitations including substantial underreporting (estimated at > 90% for serious adverse drug reactions, ADRs), inability to detect delayed adverse events, and poor detection of common events in general populations, such as cardiovascular events [6, 7, 8]. Moreover, post‐authorisation randomised controlled trials (RCTs) are quite expensive, lengthy, and usually contain a relatively small study population, which hampers their use for swift detection of an ADR. Perhaps a combination of these limitations of SRSs and post‐authorisation RCTs led to such delayed withdrawal of rofecoxib from the market.
The emergence of real‐world data (RWD), coupled with advances in IT infrastructure, improved data quality, and refined pharmacoepidemiological methods, offers new opportunities for drug safety monitoring [9]. Electronic health records (EHRs) and administrative or claims databases provide longitudinal information on diverse populations, making them valuable for evidence generation for regulatory use [10]. RWD studies can vary from traditional pharmacoepidemiologic approaches such as case–control design to more novel methods such as case‐only designs [11].
This study aimed to assess whether cardiovascular adverse effects of rofecoxib could have been detected earlier using RWD from the UK. We employed both a nested case–control (NCC) and case‐crossover (CCO) study to evaluate the association between rofecoxib and MACE at different time windows after drug marketing. By comparing our findings with those from pivotal RCTs, we sought to validate the utility of RWD for early adverse event detection.
Methods
2
Data Source
2.1
This study used data from the Clinical Practice Research Datalink (CPRD) GOLD, one of the world's largest primary care databases. The CPRD contains anonymised medical records from the UK's general practitioners (GPs) [12], covering over 21.5 million total patients with acceptable data for research purposes as of December 2024 [13]. The database comprises comprehensive patients' information, including demographics, symptoms, diagnoses, prescriptions, vaccination history, laboratory results, and referrals to hospital and specialist care (secondary care) since 1987 with demonstrated high validity for cardiovascular outcomes [14, 15].
Study Population
2.2
The study population (i.e., base cohort) comprised adult patients (≥ 18 years old) with at least one rofecoxib prescription between 20 May 1999 (UK market entry) and 30 September 2004 (withdrawal). The cohort entry date was defined as the date of the first rofecoxib prescription. All patients were required to have at least 1 year of pre‐cohort history to ensure complete medical records and valid registration status throughout the study period.
Exposure and Outcome
2.3
The primary outcome was the first MACE defined as MI, stroke, and heart failure (HF) [16]. These outcomes were identified using validated Read‐codes in CPRD. The index date was defined as the date of outcome occurrence. To capture incident cases only, we excluded individuals with any recorded MACE before cohort entry.
The exposure of interest was rofecoxib prescription which was retrieved using CPRD product codes. Exposure to rofecoxib was stratified based on the most recent prescription before the index date into current (≤ 3 months), recent (3–6 months), and past use (> 6 months) for the NCC and was assessed at the start of each 3‐month interval for the CCO design. Information on dose and treatment duration was mapped using prescribed daily dose (dosageid), number of tablets (qty), and strength from the Therapy file and CPRD GOLD's Products dictionary.
We adopted the two NCC and CCO designs in this case‐study because both are recognised tools for post‐authorisation safety monitoring [17]. The NCC is the standard design for rare outcomes, needs far less person‐time, and is computationally lighter and faster to run than a cohort. Also by sampling controls only from ever‐users, it improves baseline comparability and reduces confounding by indication [18, 19]. The CCO complements this by comparing each case's exposure immediately before the event with the same person's earlier records, cancelling all time‐invariant confounders. It is preferred when the outcome is acute and the exposure is transient [20], as was the case of rofecoxib and sudden cardiovascular events.
Nested Case–Control (NCC) Design
2.4
Cases were defined as patients who experienced first MACE during study period (Figure 1). For each case, up to four controls were matched on age, sex, GP practice, and calendar time (±30 days). The index date for controls was the same date as that of the corresponding case.
Nested case–control and case‐crossover design. The index date is the date of the first occurrence of the outcome. (a) Rofecoxib exposure was classified based on the most recent prescription before the index date into current (≤ 3 months), recent (3–6 months), and past use (> 6 months). (b) Only among the cases, we defined a 3‐month risk window before the index date, a 3‐month washout window before that, and up to four prior 3‐month reference windows.
In secondary analyses, we examined dose–response and duration‐response relationships among current users, by categorising daily doses (< 25 mg and ≥ 25 mg) and duration of continuous use (≤ 1 month, 1–3 months, 3–6 months and > 6 months) [21, 22], using the method explained previously [23, 24]. Here, if the daily dose value was missing or zero, it was assumed to be ‘as needed (pro‐re‐nata, PRN)’ and replaced by 0.5. The missing or zero value for the duration was replaced by the median duration of use (i.e., 28 days), and implausibly high values were replaced by the 3rd interquartile range (i.e., 112 days).
We conducted subgroup analysis stratified by sex, age groups (18–49, 50–64, 65–79, ≥ 80), main indications for rofecoxib use (rheumatoid arthritis (RA), back pain, osteoarthritis (OA)), and history of cardiovascular disease (post hoc analysis).
Case‐Crossover (CCO) Design
2.5
In this second design, only the cases were included, and their past experience served as their own control. In this CCO design, we defined ‘risk window’, which entailed the last 3 months before the index date and up to four ‘reference windows’, which were 3‐month periods in the past, and by definition at least 3‐months apart from the risk window with a ‘washout window’ (Figure 1). The reference windows must be between May 1999 and Sep 2004 when the drug was on the market. Moreover, only cases with an index date equal to or above 9 months (≥ 273 days) after the drug's market approval were included so every case had at least one reference window (i.e., a 91‐days reference +91‐days washout +91‐days risk windows).
As a sensitivity analysis, we repeated the analyses with a risk and reference windows of 1‐month and 6‐months, but the washout window remained at 3‐months to not mix the exposure classification between the risk and reference windows. Cases were included if they had at least one reference window.
Cumulative Uptake Time Analysis
2.6
Additionally, we conducted a cumulative uptake time analysis in both NCC and CCO designs. The idea was to identify the shortest time necessary to detect the association between rofecoxib use and MACE since the drug was initially introduced to the market, considering sufficient sample size and the plausible biological mechanism behind. To do that, we classified our study period into the following time windows: 1‐, 2‐, 3‐, 4‐ and 5‐years after the market uptake time (20 May 1999).
Potential Confounders
2.7
Potential confounders were identified based on established risk factors for cardiovascular events and clinical relevance. Age, sex, GP practice and calendar time were addressed through matching. The most recent information on smoking, and body mass index (BMI) was determined at the index date. To account for heathy‐use and surveillance biases, we assessed healthcare utilisation by measuring the frequency of GP contacts in the year preceding the index date. A history of the following comorbidities before the index date was assessed: alcohol abuse, back pain, cardiovascular diseases, chronic kidney disease (CKD), chronic liver disease, chronic respiratory diseases, diabetes (type 2), dysmenorrhea, hyperlipidaemia, hypertension, malignant neoplasms (excluding non‐melanoma skin cancers), RA, OA and migraine. Additionally, the use of comedications in the 3‐months prior to the index date was considered: angiotensin‐converting enzyme inhibitors and angiotensin receptor blockers, aspirin, beta‐blockers, calcium channel blockers, corticosteroids, diuretics, glycosides (e.g., digoxin), hormone replacement therapy, immunosuppressants (other than corticosteroids), lipid‐lowering agents (e.g., statins, fibrates, nicotinic acid or niacin, ezetimibe), nitrates, NSAIDs (other than rofecoxib), platelet aggregation inhibitors and vasodilators.
Statistical Analysis
2.8
Baseline characteristics were summarised using descriptive statistics, with continuous variables presented as means (±SD) and categorical variables as frequencies and proportions. Conditional logistic regression models were fitted in both NCC and CCO analyses to estimate the association between rofecoxib use and MACE (using the SAS PHREG procedure). Following the multiplicative intensity model proposed by Aalen [25, 26], we estimated intensity ratios (IRs) with 95% confidence intervals. In the NCC regression model, past use was considered as a reference for comparison. The final set of confounders in the conditional logistic regression model of the NCC design was selected after checking in univariate models (using the change‐in‐estimate criterion with a 10% cut‐off) [27], and broadened based on experts' opinion and subject matter knowledge due to the screening nature of the study. In the CCO study, age was included in the model as the only time‐varying confounder. Collinearity between potential confounders was assessed, and if detected, comorbidities were prioritised over comedications. Data were analysed using SAS version 9.4.
Results
3
We identified 3218 cases with first MACE between 1999 and 2004, who were matched with 10 745 controls (Figure 2). The mean age was 74 years (±11 years) among cases and 66% were women (Table 1). Cases exhibited a higher burden of cardiovascular risk factors compared to controls, including higher prevalence of cardiovascular diseases (43% vs. 29%), hypertension (42% vs. 36%), and diabetes (13% vs. 8%). In the 3‐months preceding the index date, cases more frequently used medications, particularly aspirin (30% vs. 18%), diuretics (43% vs. 32%), and corticosteroids (10% vs. 7%).
Flowchart of the establishment of the study population.
NCC Analysis
3.1
Among the cases, 1350 (42%) were current users of rofecoxib, 335 (10%) were recent users and the remaining 1533 (48%) were past users. Current use of rofecoxib was associated with a 19% increased risk of MACE compared to past use (adjusted IR [aIR] 1.18, 95% CI 1.08–1.29), while recent use showed no significant association (aIR 1.00, 95% CI 0.86–1.15) (Table 2). The cumulative uptake time analysis revealed that this association became statistically significant only after 3 years of market availability (year 3‐aIR 1.46, 95% CI 1.18–1.81), with no significant associations earlier (year 1‐aIR 0.51, 95% CI 0.06–4.33, year 2‐aIR 1.48, 95% CI 0.95–2.32) (Figure 3).
*Results of the cumulative uptake time analysis from: (a) the nested case–control and (b) and case‐crossover designs. aAdjusted for smoking status, BMI, alcohol abuse, RA, OA, back pain, migraine, cardiovascular disease, hyperlipidaemia, hypertension, chronic liver disease, chronic kidney disease, diabetes, malignant neoplasms, corticosteroids, platelet aggregation inhibitors, NSAIDs and healthcare utilisation. bAdjusted for smoking status, BMI, RA, OA, back pain, migraine, cardiovascular disease, hyperlipidaemia, hypertension, diabetes, malignant neoplasms, corticosteroids, NSAIDs and healthcare utilisation. cAdjusted for smoking status, cardiovascular disease and diabetes. Number of discordant risk and reference windows was reported in the case‐crossover graph.
Secondary analyses demonstrated similar risk elevations for both current high (≥ 25 mg: aIR 1.17, 95% CI 1.04–1.32) and low‐dose rofecoxib use (< 25 mg: aIR 1.19, 95% CI 1.06–1.32) (Table 2). Duration‐response analysis showed increased risk only with continuous use exceeding 3 months (3–6 months: aIR 1.28, 95% CI 1.08–1.52, and > 6 months: aIR 1.25, 95% CI 1.11–1.42).
Subgroup analyses revealed a numerically stronger association among men (current use: aIR 1.26, 95% CI 1.07–1.48) compared to women (current use: aIR 1.14, 95% CI 1.02–1.28). Among indication‐specific analyses, a positive association was observed in patients with back pain (aIR 1.30, 95% CI 1.11–1.51) and OA (aIR 1.19, 95% CI 1.06–1.34), while the association in RA patients was statistically nonsignificant. Additionally, current use of rofecoxib only in patients with no history of cardiovascular disease had a significant association with MACE (aIR 1.23, 95% CI 1.18–1.41) (Table S1).
CCO Analysis
3.2
The CCO analysis included 3210 risk windows matched to 12 737 reference windows (Table 3). Of 15 947 total risk and reference windows, 9883 (62%) were included as discordant sets in the analysis (1993 risk windows–50% exposed, 7890 reference windows–30% exposed). The overall association between rofecoxib use and MACE was stronger in the CCO design (aIR 1.83, 95% CI 1.53–2.18) compared to the NCC design. The cumulative uptake time analysis detected a significant association 2 years after market entry in the UK (aIR of 3.94, 95% CI 1.88–8.25), but not earlier (Figure 3).
The sensitivity analysis assuming risk and reference windows of 1‐month yielded a 46% increased risk of MACE (aIR 1.46, 95% CI 1.26–1.71), while with exposure windows of 6‐months long there was an 83% increased risk of MACE (aIR 1.83, 95% CI 1.44–2.32) (Table 3).
Discussion
4
Using RWD from the UK, we investigated the earliest possible detection of cardiovascular adverse effects associated with rofecoxib after its market introduction. The NCC design identified a 18% increased risk of MACE among current users compared to past users, with the association becoming statistically significant 3 years after market entry. The CCO design detected a stronger association, that is, 83% increased risk, and identified the signal 2 years after market introduction, suggesting potential advantages of self‐controlled designs for early safety signal detection.
Our findings align with evidence from pivotal RCTs, though with varying effect magnitudes. The VIGOR trial [22], first documented this association, reporting a 2.4‐times increased risk of MI in rofecoxib users compared to naproxen users. The APPROVe trial, comparing rofecoxib to placebo [3], found a 1.9‐fold increased risk of cardiovascular events (a broader definition than ours), more closely aligned with our CCO estimates. The differing effect sizes likely reflect variations in outcome definitions, comparison groups, study populations, and unmeasured confounding in our study.
Our NCC results are partially consistent with earlier observational studies. The case–control study by Andersohn et al. using the CPRD data found an OR of 1.29 (CI 1.02–1.63) for MI with current use of rofecoxib compared to non‐use [28]. While their effect estimate aligns with our NCC findings (aIR 1.18), the slight difference might be explained by varying eligibility criteria applied (age, history of MI, etc.), outcome definitions (MI vs. MACE), and reference groups (non‐use instead of past use). Noteworthy, Andersohn et al. looked into drug‐class safety profiling across several COX‐2 inhibitors and non‐selective NSAIDs, while our intention was to use the ‘rofecoxib case‐study’ to assess how a RWD study can perform for early signal detection. While we found comparable associations with high‐ (aIR 1.17) and low‐ doses (aIR 1.19), both lying very close to our main result (aIR 1.18), Andersohn et al. and Graham et al. found a pronounced dose–response relationship [21, 28].
Regarding methods for safety monitoring of newly marketed drugs, two recent studies investigated the potential role of RWD and pharmacoepidemiologic methodologies using rofecoxib and cardiovascular events as an example. Patadia and colleagues, implemented a hypothesis‐free signal detection method to explore the association comparing seven European healthcare databases (EU‐ADR project) with WHO‐VigiBase [29]. Using the longitudinal gamma Poisson shrinker method, they detected the MI signal of rofecoxib 4 years earlier than SRS. Their findings highlight the limitation of SRS in detecting common adverse effects and the role of RWD in safety monitoring. Moreover, a recent case‐time control and cohort study within Danish healthcare registers found that the association between rofecoxib and MI could have been identified as early as 1.5 years with a case‐time control design and 3.5 years with a cohort design [30]. The results of this study and ours are aligned in the sense of suggesting that a case‐only design might be superior than a traditional one (i.e., cohort or case–control) for drug safety monitoring purposes. Using only those subset of patients who experienced the ADR of interest, the case‐only designs are quick, efficient (especially for an acute outcome and transient exposure), and can reliably contain the residual confounding and selection bias by comparisons to past history of same patients [31]. The early detection of ADRs through RWD could have significant clinical implications, in terms of awareness, and potentially preventing those through earlier intervention or discontinuation. Also, regulatory bodies can benefit by having swifter responses to emerging safety concerns of new medications [10, 17].
The current study had several strengths. The use of CPRD GOLD provided a large, representative sample of rofecoxib users with comprehensive clinical information. The use of two study designs offered insights into methodological considerations for safety surveillance. Despite matching and statistical adjustment in the NCC, and inherent adjustment of time‐invarying confounders in the CCO design, residual confounders could have affected the observed associations. Both the exposure and outcome of interest of this study are suitable candidates for a CCO design [20]. Rofecoxib was an analgesic, so patients typically took it only when they experienced pain. Also, MI and stroke were acute outcomes with a sudden onset. The only exception here was heart failure. To prevent a potential reverse causality [32], and buffering issues with adherence and delays with dispensing time, we defined the current use and risk windows as 3‐months rather than 1‐month. Moreover, through CPRD we could include important lifestyle parameters such as smoking, BMI, and alcohol abuse as risk factors for cardiovascular morbidity.
However, several limitations warrant discussion. Despite CPRD's validated recording of cardiovascular outcomes, potential misclassification of heart failure might have affected our estimates. Unlike well‐recorded MI and stroke [15], the number of heart failure events might have not been adequately captured in the primary care database which might underestimate the association. Moreover, the assumption of low‐dose use for ‘as needed’ prescriptions could have introduced exposure misclassification. The weaker associations observed with shorter risk windows might reflect both exposure misclassification and immeasurable time bias due to lack of drug use data during hospitalisations [33]. Furthermore, CPRD lacks information on over‐the‐counter medications (e.g., aspirin and other NSAIDs). As we included other NSAIDs use as a covariate in our final model, an incomplete capture of its actual use might have led to some unmeasured confounding, but there is no evidence that this was different among cases and controls. Finally, case‐crossover design is sensitive to prescribing trends: rising use inflates the risk estimate, whereas the drop after the 2002 label change might have pushed it towards the null [2].
Conclusion
5
This study demonstrated that cardiovascular adverse effects of rofecoxib could have been detected within 2 years of market entry using RWD and appropriate pharmacoepidemiologic methodologies, considerably earlier than traditional pharmacovigilance systems or post‐authorisation clinical trials. Particularly, the use of case‐only designs, such as CCO, showed promise for early signal detection. These findings advocate for the systematic integration of RWD analysis into routine drug safety monitoring systems for quicker signal detection and more timely regulatory action.
Author Contributions
D.M., P.C.S. and S.A. had full access to all the data in the study and take responsibility for the integrity of data and accuracy of data analysis. All authors were responsible for the concept and design of the study. P.C.S. conducted data acquisition. P.C.S., D.M., S.A. and S.B. were in charge of data analysis. All authors were involved in the interpretation of results. D.M. wrote the first draft of the manuscript, and all authors critically revised the manuscript for important intellectual content. P.C.S. and S.A. were responsible for administrative, technical or material support. S.A. and O.H.K. have supervised the lead author (D.M.) in conducting this study.
Funding
The authors have nothing to report.
Disclosure
The authors have nothing to report.
Ethics Statement
This study was reviewed and approved by Research Data Governance (RDG) Process (reference 23_003111), which is responsible for reviewing protocols for scientific quality. This study is based in part on data from the Clinical Practice Research Datalink obtained under licence from the UK Medicines and Healthcare products Regulatory Agency. The data is provided by patients and collected by the NHS as part of their care and support. The interpretation and conclusions contained in this study are those of the authors alone.
Consent
The authors have nothing to report.
Conflicts of Interest
The authors declare no conflicts of interest.
Supporting information
Table S1: Subgroup analysis in the nested case‐control design of the association between rofecoxib and major cardiovascular adverse events in the UK.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Merck , Merck Announces Voluntary Worldwide Withdrawal of VIOXX (Merck, 2004).
- 2E. J. Topol , “Failing the Public Health—Rofecoxib, Merck, and the FDA,” New England Journal of Medicine 351, no. 17 (2004): 1707–1709, 10.1056/nejmp 048286.15470193 · doi ↗ · pubmed ↗
- 3R. S. Bresalier , R. S. Sandler , H. Quan , et al., “Cardiovascular Events Associated With Rofecoxib in a Colorectal Adenoma Chemoprevention Trial,” New England Journal of Medicine 352, no. 11 (2005): 1092–1102, 10.1056/NEJMOA 050493.15713943 · doi ↗ · pubmed ↗
- 4J. A. Baron , R. S. Sandler , R. S. Bresalier , et al., “Cardiovascular Events Associated With Rofecoxib: Final Analysis of the APPRO Ve Trial,” Lancet (London, England) 372, no. 9651 (2008): 1756–1764, 10.1016/S 0140-6736(08)61490-7.18922570 · doi ↗ · pubmed ↗
- 5J. Lexchin , “How Safe Are New Drugs? Market Withdrawal of Drugs Approved in Canada Between 1990 and 2009,” Open Medicine 8, no. 1 (2014): e 14.25009681 PMC 4085091 · pubmed ↗
- 6Y. Moride , F. Haramburu , A. A. Requejo , and B. Bégaud , “Under‐Reporting of Adverse Drug Reactions in General Practice,” British Journal of Clinical Pharmacology 43, no. 2 (1997): 177–181, 10.1046/j.1365-2125.1997.05417.x.9131950 PMC 2042725 · doi ↗ · pubmed ↗
- 7R. Sharrar and G. Dieck , “Monitoring Product Safety in the Postmarketing Environment,” Therapeutic Advances in Drug Safety 4, no. 5 (2013): 211–219.25114782 10.1177/2042098613490780 PMC 4125313 · doi ↗ · pubmed ↗
- 8F. Haguinet , A. Bate , and J. U. Stegmann , “The Futility of Adverse Drug Event Reporting Systems for Monitoring Known Safety Issues: A Case Study of Myocardial Infarction With Rofecoxib and Other Drugs,” Pharmacoepidemiology and Drug Safety 33, no. 1 (2024): e 5719, 10.1002/PDS.5719.37867313 · doi ↗ · pubmed ↗