Rapid Normalization of Amniotic Fluid Index Following Discontinuation of Olmesartan: A Case Report
Annika Van Oosbree, Therese Larson, Hannah Conley, Matthew Bridges, Pedro Argoti, Giancarlo Mari

TL;DR
Stopping olmesartan during pregnancy led to rapid recovery of amniotic fluid and a healthy baby, suggesting that ARB-related fetal issues may be reversible.
Contribution
First reported case of reversible anhydramnios from olmesartan use in early pregnancy with a favorable neonatal outcome.
Findings
Amniotic fluid index normalized within 2 weeks after discontinuing olmesartan.
The infant was born viable with reassuring renal function and mild, improving calyceal dilation.
Timely drug withdrawal may restore amniotic fluid and prevent severe fetal complications.
Abstract
Angiotensin II receptor blockers (ARBs) are commonly used for hypertension but are contraindicated in pregnancy due to risks of oligohydramnios, renal dysgenesis, and pulmonary hypoplasia from suppression of the fetal renin–angiotensin system. Olmesartan, a frequently prescribed ARB, has a longer receptor binding half-life and higher affinity than other ARBs, producing more potent and sustained antihypertensive effects. Emerging evidence suggests that stopping ARBs during pregnancy may allow recovery of amniotic fluid and renal function. A 30-year-old primigravida with chronic hypertension presented at 24 weeks' gestation while taking olmesartan. Ultrasound revealed anhydramnios with a normal-appearing fetal genitourinary tract. Olmesartan was discontinued and replaced with labetalol. Within 2 weeks, the amniotic fluid index normalized, and subsequent ultrasounds showed sustained…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
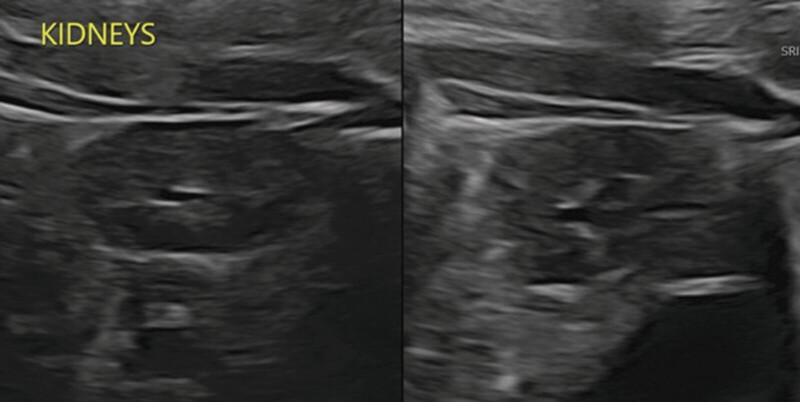 Fig. 1
Fig. 1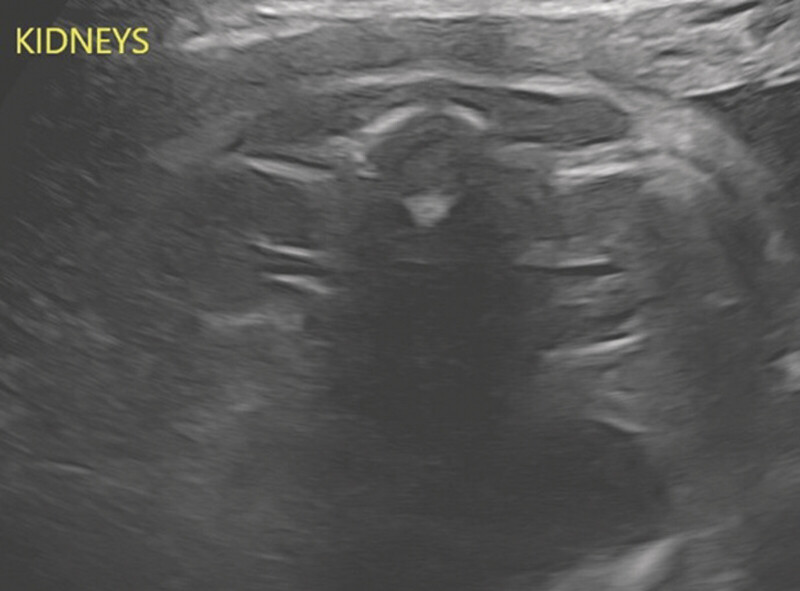 Fig. 2
Fig. 2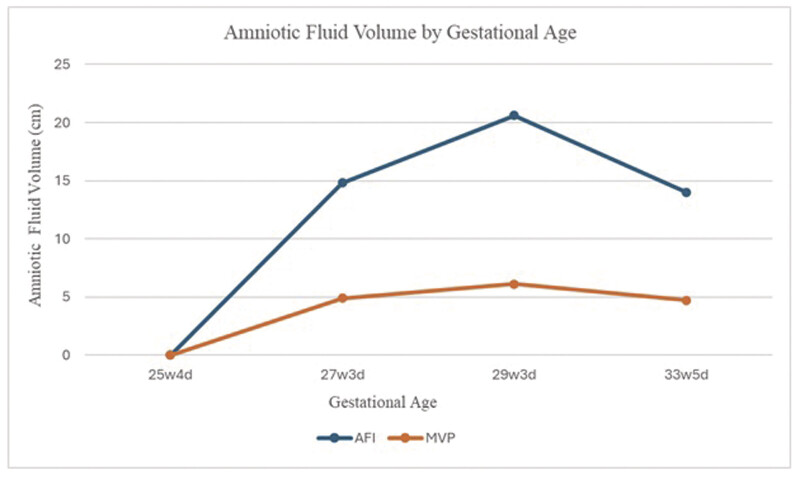 Fig. 3
Fig. 3 Fig. 4
Fig. 4| Gestational Age (wk) | BPD (mm) | HC (cm) | AC (cm) | FL (cm) | AFI (cm) | MVP (cm) | UA − S/D | Comments |
|---|---|---|---|---|---|---|---|---|
| 25 4/7 | 60.6 | 229.8 | 207.5 | 46.8 | 0 | 0 | 3.50 | Bilateral kidneys are visualized |
| 27 3/7 | NA | NA | NA | NA | 14.8 | 4.9 | NA | Bladder and stomach visualized |
| 29 3/7 | 73.8 | 277.7 | 249.9 | 56.3 | 20.6 | 6.1 | NA | NA |
| 33 5/7 | 82.5 | 296.1 | 288.1 | 63.8 | 14.0 | 4.7 | NA | NA |
| Reference | ARB used | Gestational age at presentation (or when oligohydramnios was diagnosed; wk) | Immediate fetal/neonatal outcome | Long-term outcome/follow-up |
|---|---|---|---|---|
|
Briggs et al (2001)
| Valsartan | 24 | Anhydramnios, pulmonary hypoplasia, very small placenta | IUFD |
|
Pietrement et al (2003)
| Telmisartan | 33 | Oligohydramnios | Neonatal survival. Acute renal failure without resolution on day 3 of life |
|
Berkane et al (2004)
| Valsartan | 20 | None | Neonatal survival |
|
Bakkum et al (2006)
| Losartan | 27 | Oligohydramnios resolved after cessation > inferior vena cava thrombosis | Neonatal survival |
|
Bass and Faix (2006)
| Losartan | 29 | Anhydramnios, empty fetal bladder, transient renal failure | Neonatal survival. Renal tubular acidosis |
|
Simonetti et al (2006)
| Candesartan | 31 (delivered at that time) | Limb contractures, skull hypoplasia with microcephaly, underdeveloped valvarial bones, RDS, moderate oliguria | Neontal survival. Neurocognitive challenges (cognitive and linguistic), small hyperechogenic kidneys |
|
Celetano et al (2008)
| Olmesartan | 29 | Oligohydramnios and fetal renal impairment | Neonatal survival. No long-term effects |
|
Munk et al (2010)
| Candesartan | 22 | Severe oligohydramnios and fetal renal edema | Neonatal survival. Reversible fetal renal failure with recovery after cessation of candesartan |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPregnancy and preeclampsia studies · Renin-Angiotensin System Studies · Birth, Development, and Health
Introduction
Angiotensin II receptor blockers (ARBs) are first-line antihypertensive agents in the general population but are contraindicated in pregnancy due to the risk of fetal complications, including oligohydramnios, renal dysgenesis, and pulmonary hypoplasia. These effects result from suppression of the fetal renin–angiotensin system, reducing renal perfusion and urine output. 1 2 Olmesartan is a commonly-prescribed ARB that has been shown to have more robust effects on both systolic and diastolic blood pressures compared with other drugs in this class. 3 4 5 The American College of Obstetricians and Gynecologists recommends avoidance of ARBs in pregnancy due to the risk of fetal malformations and growth restriction. 6 Emerging evidence based on case reports and series demonstrates that discontinuation of ARBs in the first and second trimester of pregnancy may allow for recovery of amniotic fluid volume and renal function. We present a case of anhydramnios after first- and second-trimester olmesartan exposure that promptly resolved following drug cessation, resulting in a favorable neonatal outcome, highlighting the potential for reversibility of ARB-related fetopathy.
Case Presentation
A 30-year-old G1 at 24 ^3/7^ weeks with chronic hypertension (CHTN) presented with severe-range blood pressures concerning for a CHTN exacerbation versus superimposed preeclampsia. She had been on olmesartan and triamterene/HCTZ prior to pregnancy recognition. She reported compliance with this medication regimen. Ultrasound showed anhydramnios with a normal-appearing fetal genitourinary system ( Fig. 1 ); rupture of membranes was ruled out with an amniotic fluid dye test. Intravenous antihypertensives were used acutely, and she was transitioned to labetalol 400 mg three times per day. She was ultimately diagnosed with CHTN exacerbation and discharged.
Normal-appearing fetal kidneys.
She was monitored outpatient with serial ultrasounds. A week later, the ultrasound showed normal amniotic fluid volume. Two weeks after discontinuation, the amniotic fluid index (AFI) was improved to 14.0. Subsequent ultrasounds at 29 ^3/7^ weeks gestational age and 33 ^5/7^ weeks gestational age also showed improvement in AFI (20.6 and 14.0, respectively; see Table 1 and Fig. 2 ). Fetal anatomy was completed and was unremarkable.
Amniotic fluid volume by gestational age.
At 33 ^4/7^ weeks of gestational age, she was diagnosed with superimposed preeclampsia with severe features. Induction of labor was initiated at 34 weeks, and she vaginally delivered a viable male infant weighing 2,390 g with APGARs of 6 and 7 at 1 and 5 minutes, respectively. His creatinine was 0.7 at birth and remained 0.7 to 0.8 throughout his admission. The infant's NICU course was complicated only by a renal ultrasound showing mild left-sided central calyceal dilation ( Fig. 3 ). He was ultimately discharged on day 17 of life. He is being followed up for the left-sided central calyceal dilation, which is improving ( Fig. 4 ).
Renal ultrasound at 1 day old.
Renal ultrasound at approximately 6 months old.
Discussion
Fetopathy related to renin–angiotensin system inhibitors, including angiotensin-converting enzyme inhibitors and ARBs, is well recognized, particularly with second- and third-trimester exposure. The classical findings include oligohydramnios, fetal growth restriction, calvarial hypoplasia, renal tubular dysgenesis, and pulmonary hypoplasia. 6 Renal abnormalities are frequently reported, most commonly renal tubular dysgenesis of the proximal tubule. Other findings include glomerular cysts, vascular thickening, and interstitial fibrosis, which may present on prenatal ultrasound as enlarged, hyperechogenic kidneys. 7 8 The pathophysiology is thought to arise from suppression of the fetal renin–angiotensin system, leading to impaired renal perfusion, reduced fetal urine output, and consequently, oligohydramnios development.
Although these complications have historically been associated with poor prognosis, several reports demonstrate reversibility after discontinuation of the offending agent. Chisholm et al described anhydramnios at 27 weeks in a patient on benazepril that normalized within 12 days. 9 Muller and James reported oligohydramnios with cranial abnormalities after benazepril exposure until 24 weeks, which resolved after withdrawal, though complicated by growth restriction. 10 Wei et al noted normalization of amniotic fluid within 8 days of stopping losartan at 32 weeks, with normal neonatal renal findings. 11 Similarly, Munk et al described improvement in amniotic fluid and postnatal resolution of renal changes following candesartan discontinuation. 12 Cases with good prognoses involving candesartan, telmisartan, losartan, and olmsartan 13 14 15 16 17 ; on the other hand, poor prognoses have been reported involving candesartan and valsartan 18 19 ( Table 2 ).
A larger review examined 83 fetuses exposed to ARBs in the second or third trimester, finding oligohydramnios in 58 cases. Of these, 19 demonstrated resolution following drug withdrawal, with outcomes ranging from perinatal death to complete recovery. Resolution generally occurred within 1 to 6 weeks, suggesting that the degree of injury may depend on both the timing and duration of exposure. 1
Olmesartan, like other ARBs, selectively antagonizes the angiotensin II type 1 (AT1) receptor, leading to vasodilation and reduced aldosterone secretion. However, it differs from many ARBs in its pharmacology and metabolism. It has one of the longest receptor binding half-lives among ARBs, leading to more sustained AT1 receptor blockade and potent, consistent blood pressure control. Olmesartan also shows higher receptor affinity compared with several other ARBs, which may explain its comparatively stronger antihypertensive effects at standard doses. 20 These properties make its pharmacodynamics somewhat distinct, although clinically it shares the class's same fetal risks. Both AT1 and AT2 receptors play a role in intrauterine development, though the AT2 receptor is predominant in fetal tissues, playing a role in organogenesis, vascular development, regulation of blood flow, and growth. 21 The AT1 receptor is more prevalent in the placenta, while the AT2 receptor is absent in some portions of the placenta. 22
The present case, to our knowledge, is the first-described case of olmesartan exposure during the first and second trimesters with discontinuation resulting in prompt, complete resolution of AFI. This is particularly significant given its higher AT1 receptor affinity than other ARBs. Not only did the AFI resolve, but the neonate's postnatal course was notable only for mild calyceal dilation, which improved on follow-up. Creatinine remained normal throughout his NICU course. This case highlights that early discontinuation of ARBs—specifically olmesartan, which is more potent than others—can lead to complete recovery of AFI and subsequent favorable neonatal outcomes. Given this case and the other previously-reported cases suggesting reversibility of anhydramnios in ARB exposure, we suggest recommending observation via serial ultrasounds rather than outright termination of pregnancy in the setting of first- and second-trimester ARB exposure.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Shimada C Akaishi R Cho K Outcomes of 83 fetuses exposed to angiotensin receptor blockers during the second or third trimesters: a literature review Hypertens Res 2015380530831325693853 10.1038/hr.2015.12 · doi ↗ · pubmed ↗
- 2Forhead A J Whybrew K Hughes P Broughton Pipkin F Sutherland M Fowden A L Comparison of angiotensin II type 1 receptor blockade and angiotensin-converting enzyme inhibition in pregnant sheep during late gestation Br J Pharmacol 1996119023934018886426 10.1111/j.1476-5381.1996.tb 15999.x PMC 1915859 · doi ↗ · pubmed ↗
- 3Stumpe K O Olmesartan compared with other angiotensin II receptor antagonists: head-to-head trials Clin Ther 200426(suppl A):A 33A 3715291378 10.1016/s 0149-2918(04)90144-0 · doi ↗ · pubmed ↗
- 4Smith D H Comparison of angiotensin II type 1 receptor antagonists in the treatment of essential hypertension Drugs 200868091207122518547132 10.2165/00003495-200868090-00003 · doi ↗ · pubmed ↗
- 5Zannad F Fay R Blood pressure-lowering efficacy of olmesartan relative to other angiotensin II receptor antagonists: an overview of randomized controlled studies Fundam Clin Pharmacol 2007210218119017391291 10.1111/j.1472-8206.2007.00464.x · doi ↗ · pubmed ↗
- 6American College of Obstetricians and Gynecologists' Committee on Practice Bulletins—Obstetrics ACOG practice bulletin no. 203: chronic hypertension in pregnancy Obstet Gynecol 201913301 e 26e 5030575676 10.1097/AOG.0000000000003020 · doi ↗ · pubmed ↗
- 7Plazanet C Arrondel C Chavant F Gubler M C Fetal renin-angiotensin-system blockade syndrome: renal lesions Pediatr Nephrol 201429071221123024477978 10.1007/s 00467-013-2749-4 · doi ↗ · pubmed ↗
- 8Saar T Levitt L Amsalem H Reversible fetal renal impairment following angiotensin receptor blocking treatment during third trimester of pregnancy: case report and review of the literature Case Rep Obstet Gynecol 201620162.382031 E 610.1155/2016/2382031 PMC 503187427672462 · doi ↗ · pubmed ↗