A multimodal endoscopic approach to early cardiac cancer in gastritis cystica profunda
Yujie Zhu, Ning Wang, Lingyun Wang

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
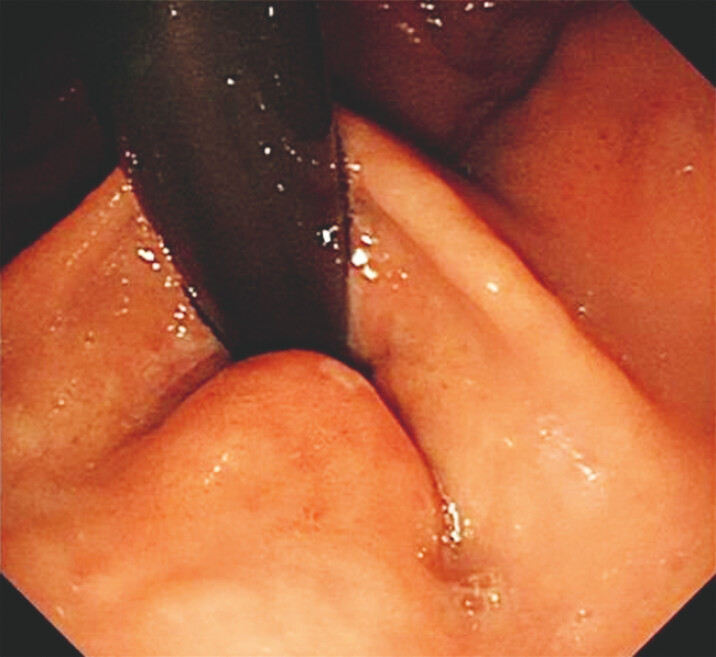 Fig. 1
Fig. 1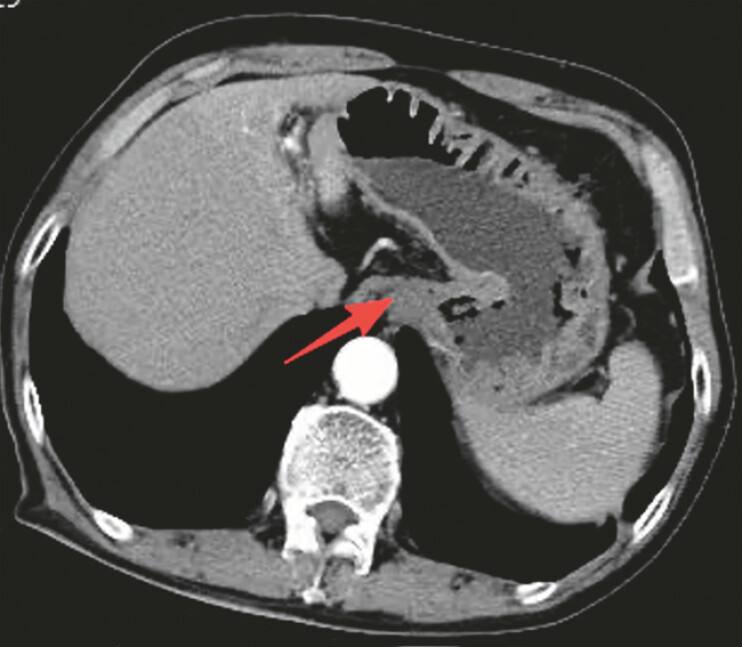 Fig. 2
Fig. 2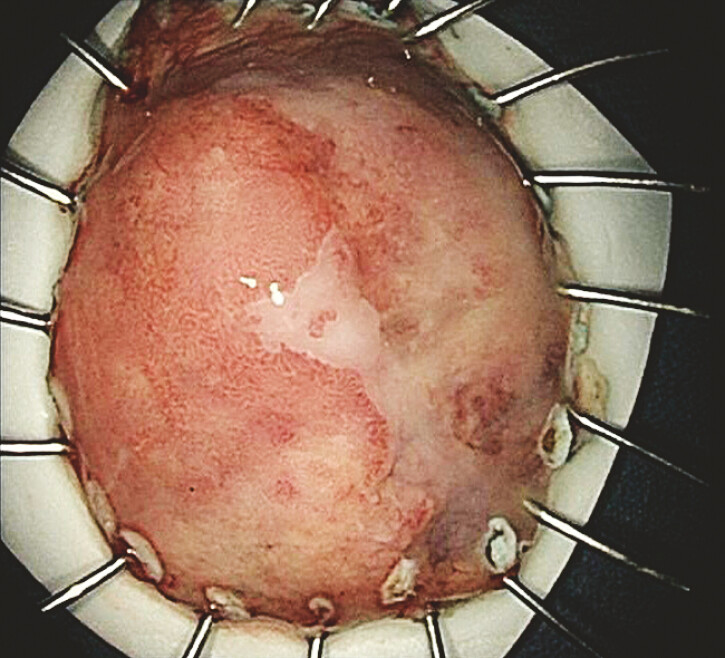 Fig. 3
Fig. 3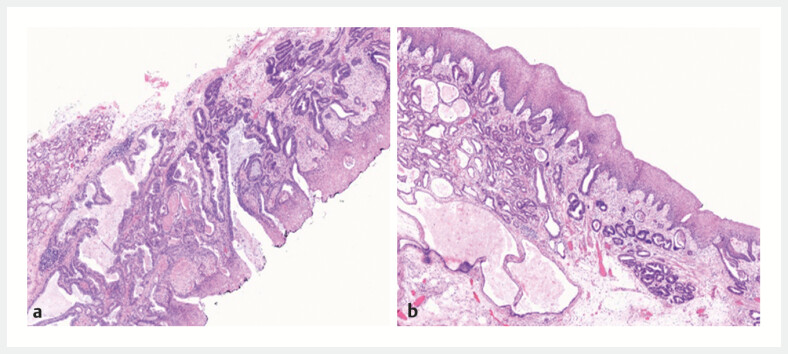 Fig. 4
Fig. 4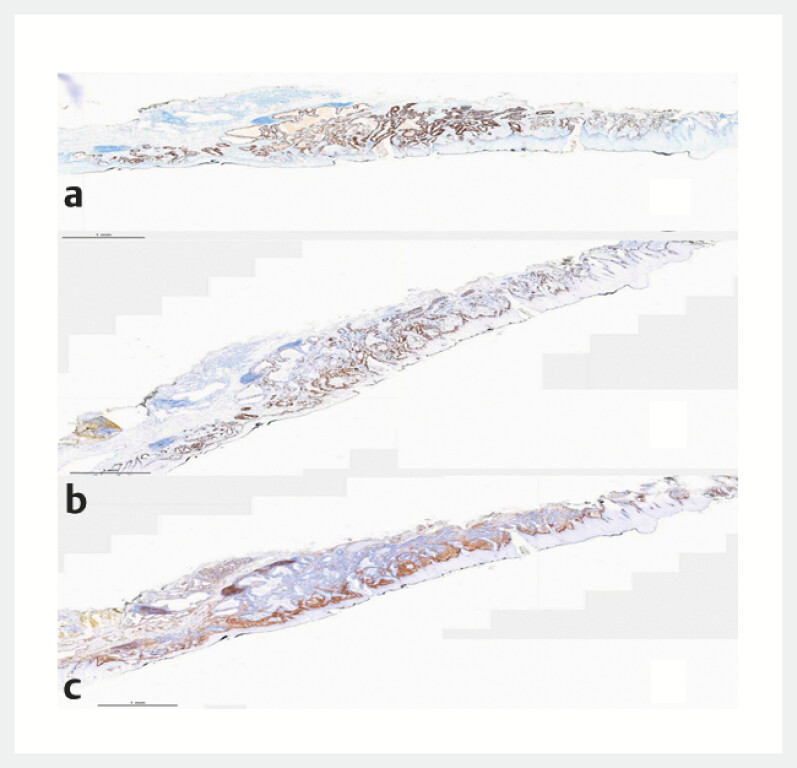 Fig. 5
Fig. 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHelicobacter pylori-related gastroenterology studies · Esophageal Cancer Research and Treatment · Metastasis and carcinoma case studies
A 68-year-old male patient presented with dysphagia. ( Fig. 1 ). Biopsy pathology indicated “high-grade dysplasia with malignant transformation.” Computed tomographic images showed thickening of the cardia wall, mild non-uniform enhancement on contrast-enhanced scanning, poor filling of the remaining stomach, and thickened walls ( Fig. 2 ). To further evaluate the nature and depth of the lesion, the patient underwent endoscopic ultrasonography (EUS), which revealed “multiple anechoic structures at the lesion site, confined to the submucosa, with unclear boundaries between the mucosal and muscular layers, partial section 8.5 mm × 10.6 mm, and a high likelihood of deep cystic gastritis (GCP; Video 1 ).” This first identified the soil for malignant transformation. An endoscopic submucosal dissection (ESD) procedure was performed for perfect specimen removal ( Fig. 3 ). Postoperative histological sections clearly showed the coexistence of submucosal infiltrating adenocarcinoma ( Fig. 4 a ) and benign cystic glands of gastritis cystica profunda (GCP; Fig. 4 b ). This further validated the EUS diagnosis. Immunohistochemical results showed P53 expression in a mutated pattern ( Fig. 5 a ). The Ki67 proliferation index was approximately 40% ( Fig. 5 b ), and desmin staining clearly demonstrated invasion into the muscularis mucosae and vasculature ( Fig. 5 c ).
A raised area of about 1.5 cm in diameter on the lesser curvature of the cardia, congested, with surface ulceration.
Thickening of the cardia wall, mild non-uniform enhancement on contrast-enhanced scanning, poor filling of the remaining stomach, and thickened walls.
Multiple anechoic structures at the lesion site, confined to the submucosa, with unclear boundaries between the mucosal and muscular layers, partial section 8.5 mm × 10.6 mm, and a high likelihood of deep cystic gastritis (GCP).Video 1
Complete resection specimen, size of about 4.5 × 3.5 × 0.2 cm, surface of a rise, size of about 2.5 × 2 × 0.8 cm, according to the surrounding cut edge of 0.4–1.4cm.
a Paraglandular adenomatous hyperplasia (magnification × 40). b Deep cystic gastritis of the local mucosa (magnification × 40).
a P53 expression in a mutated pattern, supporting the diagnosis of highly dysplastic hyperplasia. b The Ki67 proliferation index was approximately 40%. c Desmin staining clearly demonstrated invasion into the muscularis mucosae and vasculature.
GCP is characterized by the ectopic extension of gastric mucosal glands into the submucosa, accompanied by cystic dilation. The lesion most commonly occurs in the gastric cardia and subcardinal regions, predominantly affecting elderly men. 1 Although GCP itself is often considered benign, accumulating evidence indicates a close association between GCP and early gastric cancer, particularly high-grade intraepithelial neoplasia 2 3 . This case corroborates the existing literature consensus that GCP represents a significant precancerous condition and suggests its potential for malignant transformation 4 5 . This video demonstrates a comprehensive multimodal strategy, combining endoscopic ultrasound (EUS), cross-sectional imaging, and histopathology with immunohistochemistry (IHC) to guide the endoscopic resection of an early cardiac carcinoma arising from GCP.
Endoscopy_UCTN_Code_CCL_1AB_2AC_3AB
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Yuxin J Clinical characteristics of deep cystic gastritis: a summary analysis with 9 case reports Dalian Dalian Medical University 2022
- 2Ting Z Jianbo Z Fangfang ZA case of gastric cancer complicated with deep-seated cystic gastritis J Wenzhou Med Univ 202252325327
- 3Hui F Pengyue Z Yongping C Clinical analysis of 64 cases of deep-seated cystic gastritis complicated with early gastric cancer Anhui Med J 20234410861090
- 4Fuping G Junrong Y Jin W Clinical and pathological characteristics of 13 cases of deep-seated cystic gastritis complicated with early gastric cancer Anhui Med J 202226528530
- 5Niu N Endoscopic and pathological features of deep-seated cystic gastritis complicated with early gastric cancer J Clin Oncol 20232810461049