The usefulness of the novel 0.018-inch dedicated uneven double-lumen cannula for endoscopic ultrasound-guided hepaticogastrostomy using a 22-gauge needle
Mamoru Takenaka, Hirofumi Kawamoto, Tomohiro Fukunaga, Yuka Sakano, Masayuki Kurimoto, Tae Hoon Lee, Masatoshi Kudo

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
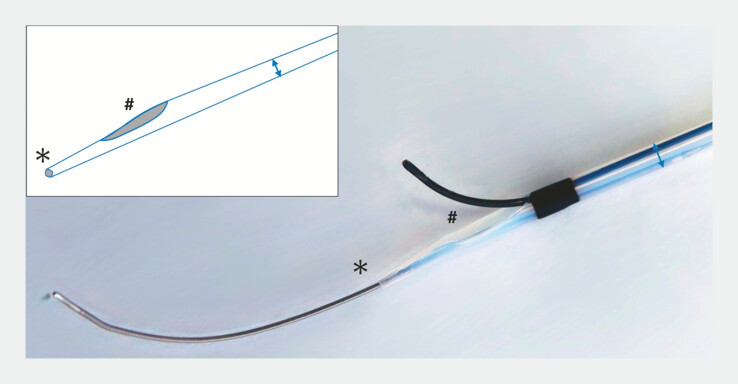 Fig. 1
Fig. 1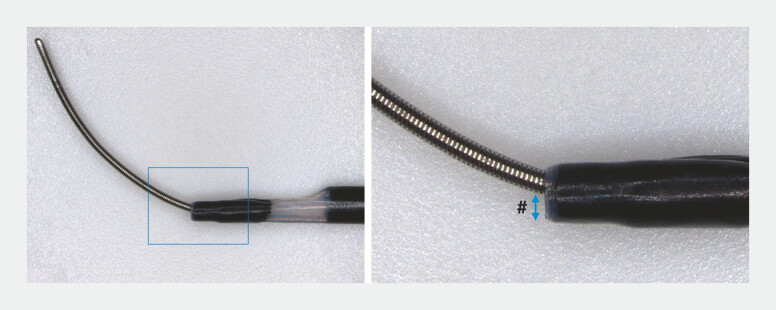 Fig. 2
Fig. 2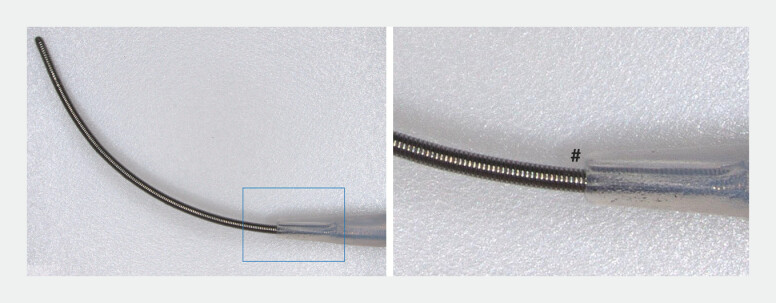 Fig. 3
Fig. 3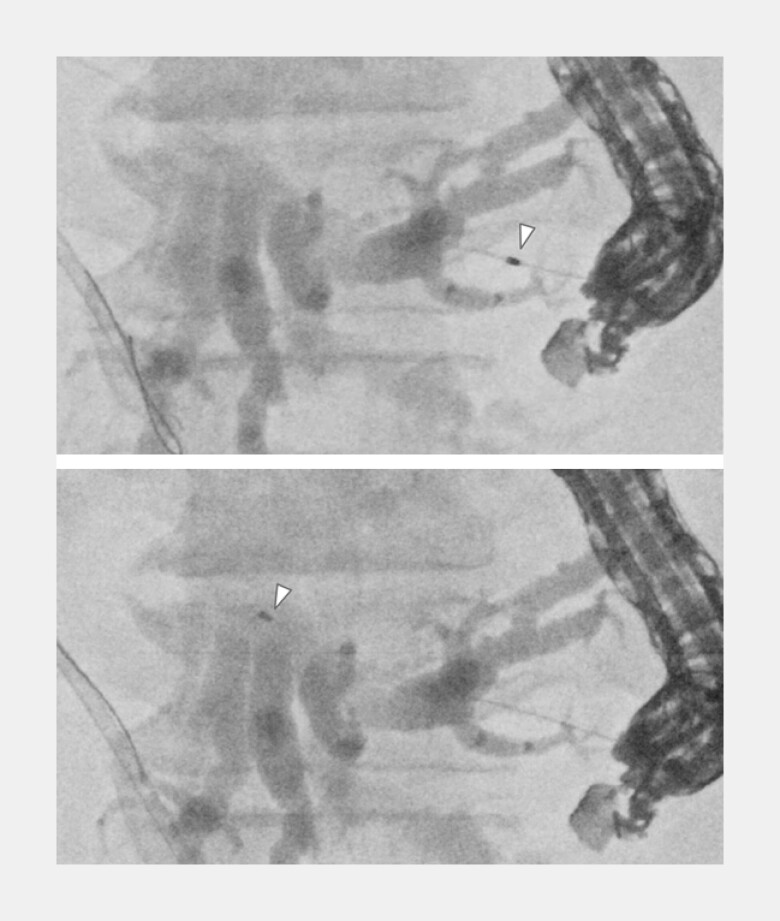 Fig. 4
Fig. 4 Fig. 5
Fig. 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGallbladder and Bile Duct Disorders · Esophageal and GI Pathology · Medical Device Sterilization and Disinfection
A 78-year-old patient with unresectable hilar cholangiocarcinoma developed malignant hilar biliary obstruction. An inside stent was first placed in the right intrahepatic bile duct, but jaundice persisted. A transpapillary approach to the left duct failed because the guidewire could not traverse the stricture; therefore, endoscopic ultrasound-guided hepaticogastrostomy (EUS-HGS) was performed. To minimize bile leakage, the bile duct was punctured using a 22-gauge EUS-fine needle aspiration needle, and a 0.018-inch guidewire was successfully advanced across the hilar stricture into the common bile duct. However, as the 0.018-inch guidewire alone had limited deliverability, establishing a double-guidewire approach was desirable thereafter.
The uneven double-lumen cannula (UDLC) has two lumens (0.025 and 0.035 inches), with the orifice of each lumen being uneven, thereby creating a channel within the tip 1 2 3 4 . A newly developed 0.018-inch dedicated UDLC (0.018-UDLC; PIOLAX, Tokyo, Japan) is a modification in which the distal tip lumen has been downsized to 0.018-inch compatibility ( Fig. 1 ). The conventional 0.025-UDLC leaves a gap between the lumen and a 0.018-inch guidewire, reducing pushability and penetration capability ( Fig. 2 ), whereas the 0.018-UDLC minimizes this gap, improving tract penetration ( Fig. 3 ).
A newly developed 0.018-inch dedicated uneven double-lumen cannula (UDLC) (0.018-UDLC; PIOLAX, Tokyo, Japan) has two lumens (0.018 and 0.035 inch), with the orifice of each lumen being uneven, thereby creating a channel within the tip.
The conventional 0.025-UDLC leaves a gap (#) between the lumen and a 0.018-inch guidewire, reducing pushability and penetration capability. UDLC, uneven double-lumen cannula.
The 0.018-UDLC minimizes the gap (#) between the lumen and a 0.018-inch guidewire, improving tract penetration. UDLC, uneven double-lumen cannula.
Through the 0.018-inch guidewire, the 0.018-UDLC successfully penetrated both the gastric and bile duct walls, and the puncture tract was dilated ( Fig. 4 ). Cholangiography was performed via the proximal lumen, and a 0.025-inch guidewire from the proximal lumen was advanced beyond the stricture to achieve a double-guidewire situation with a 0.018-inch guidewire from the distal lumen 5 ( Fig. 5 ).
Through the 0.018-inch guidewire, the 0.018-UDLC (arrowhead) successfully penetrated both the gastric and bile duct walls, and the puncture tract was dilated. UDLC, uneven double-lumen cannula.
Cholangiography was performed via the proximal lumen (yellow circle area), and a 0.025-inch guidewire from the proximal lumen (#) was advanced beyond the stricture to achieve a double-guidewire situation with a 0.018-inch guidewire from the distal lumen ().*
Subsequently, a 0.025-inch dedicated laser-cut self-expandable metal stent designed for EUS-HGS (Covered Bile Rush Advance; PIOLAX, Tokyo, Japan) was successfully deployed over the 0.025-inch guidewire ( Video 1 ).
The utility of a novel 0.018-inch dedicated, uneven double-lumen cannula for EUS-HGS in malignant hilar biliary obstruction. This newly developed 0.018-UDLC enables tract dilation, cholangiography, and double-guidewire creation using a single device, representing a practical innovation that may enhance future EUS-HGS procedures. EUS-HGS, endoscopic ultrasound-guided hepaticogastrostomy.Video 1
This newly developed 0.018-UDLC enables tract dilation, cholangiography, and double-guidewire creation using a single device, thereby enhancing the potential for interventional EUS procedures using a 22-gauge needle.
Endoscopy_UCTN_Code_TTT_1AS_2AH
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Takenaka M Yamazaki T Otsuka Y Successful use of two guidewires with different properties using a double-lumen catheter for postoperative biliary stricture Endoscopy 202254 E 190E 19233979863 10.1055/a-1478-3248 · doi ↗ · pubmed ↗
- 2Ogura T Masuda D Imoto A Double-guidewire technique using a novel ERCP cannula for hepatic hilar obstruction Endoscopy 201446 E 56E 5710.1055/s-0033-135916624523182 · doi ↗ · pubmed ↗
- 3Nakai Y Oyama H Kanai S Double Guidewire Technique Using an Uneven Double Lumen Catheter for Endoscopic Ultrasound-Guided Interventions Dig Dis Sci 2021661540154710.1007/s 10620-020-06345-932436121 · doi ↗ · pubmed ↗
- 4Ishiwatari H Satoh T Sato J Double-guidewire technique facilitates endoscopic ultrasound-guided biliary drainage for hilar biliary obstruction Endoscopy 201951 E 321E 32210.1055/a-0915-191731163486 · doi ↗ · pubmed ↗
- 5Shiomi H Masuda A Kodama Y Novel approach for successful endoscopic ultrasound-guided hepaticogastrostomy using a double-guidewire technique Dig Endosc 201931 e 50e 5110.1111/den.1332830589461 · doi ↗ · pubmed ↗