Endoscopic submucosal dissection is a safe and effective method for the treatment of duodenal papillary neuroendocrine tumor involving the pancreatic duct orifice
Yi Yang, Haibin Zhang, Kang Fang, Li Zhang, Meidong Xu

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
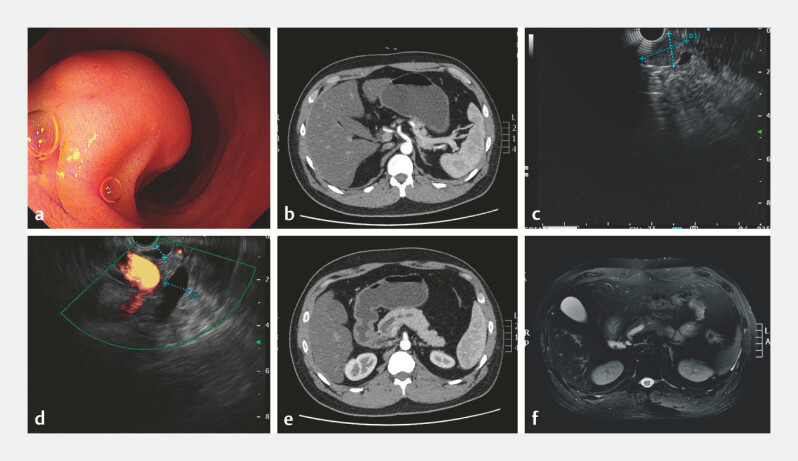 Fig. 1
Fig. 1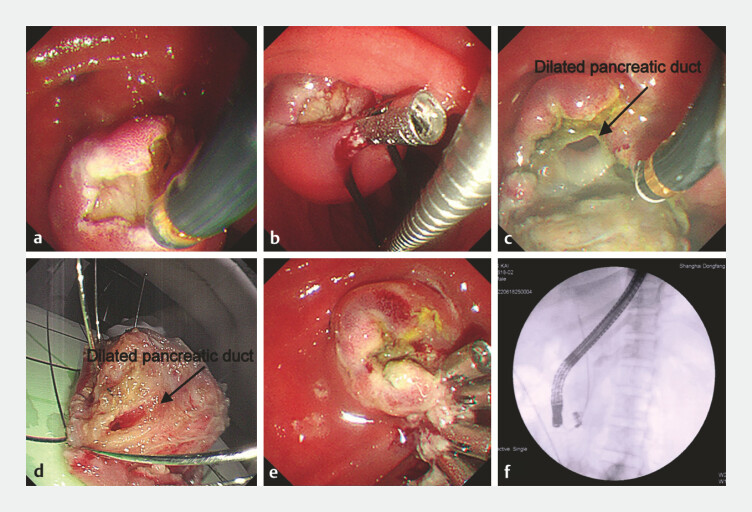 Fig. 2
Fig. 2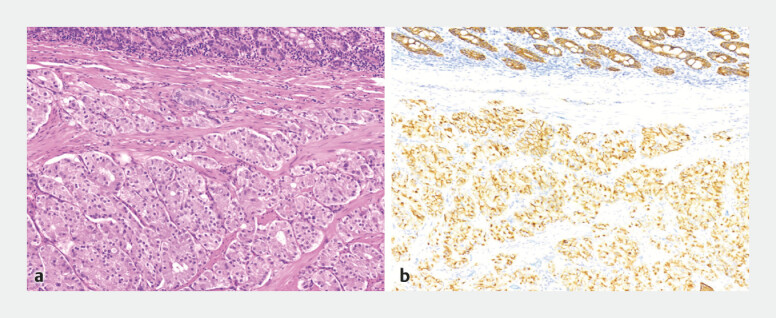 Fig. 3
Fig. 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastrointestinal Tumor Research and Treatment · Neuroendocrine Tumor Research Advances · Pancreatic and Hepatic Oncology Research
We report the case of a 32-year-old male patient with the duodenal papillary neuroendocrine tumor (NET) that was found during screening gastroscopy and computed tomography (CT; Fig. 1 a, b ). Endoscopic ultrasound (EUS) showed a hypoechoic mass of 20 mm in diameter ( Fig. 1 c ). The lesion involved the pancreatic duct orifice, with main pancreatic duct dilation (an internal diameter of about 10 mm; Fig. 1 d ). Same CT and magnetic resonance imaging revealed pancreatic duct dilation ( Fig. 1 e, f ).
Preoperative relevant imaging examinations. a Endoscopic morphology of tumor of duodenal papilla. b Computed tomography (CT) showing the nodular soft tissue of 19 mm in diameter located in the duodenal papilla. c Endoscopic ultrasound (EUS) showing a hypoechoic mass of 20 mm in diameter. d EUS showing the dilated main pancreatic duct (an internal diameter of about 1cm). e A CT scan showing the dilated main pancreatic duct. f A magnetic resonance imaging (MRI) scan showing the dilated main pancreatic duct.
We decided to perform endoscopic submucosal dissection (ESD) of the lesion ( Video 1 ). After submucosal injection of glycerin fructose and indigo carmine showed adequate lifting, we made a marginal incision and gradually dissected along the base with the help of the metal clip and snare ( Fig. 2 a, b ). After transection of the pancreatic duct, intraoperative findings revealed tumor involving the pancreatic duct orifice with pancreatic duct dilation ( Fig. 2 c, d ). Electrocoagulation was used for hemostasis and the metal clips were used to close the wound surface ( Fig. 2 e ). Endoscopic retrograde cholangiopancreatography was performed to place the stents in the common bile and the pancreatic duct ( Fig. 2 f ). There were no complications during the perioperative period. The postoperative pathology confirmed the NET G1 stage ( Fig. 3 a, b ). At a 3-month follow up, gastroscopy revealed a regular scar, without macroscopic evidence of tissue residues or signs of recurrence.
Endoscopic dissection of duodenal papillary neuroendocrine tumors involving the pancreatic duct.Video 1
The process of the endoscopic submucosal dissection (ESD) of the duodenal papilla NET. a Incision along the margin of the tumor using the golden knife. b Traction assistance using the clips and snare. c Transection of the main pancreatic duct with pancreatic duct dilation. d The resected tumor with the dilated main pancreatic duct. e Closing the wound surface using metallic clips. f Placement of one stent in the common bile duct (7 F10 cm straight plastic stents) and one in the main pancreatic duct (5 F9 cm single pigtail plastic stent). NET, neuroendocrine tumor.
Postoperative pathology. a Hematoxylin–eosin (H&E)-stained and b immunohistochemical staining for CgA views of the resected specimen.
Duodenal papillary NETs are exceedingly rare, accounting for less than 2% of all ampullary tumors 1 , particularly those involving the pancreatic duct orifice. There are currently no guidelines for managing ampullary NETs 2 . Surgery, such as pancreaticoduodenectomy, is the traditional treatment for such cases 3 . We reported for the first time that ESD was performed for the duodenal papillary NET involving the main pancreatic duct orifice, which was a safe and feasible treatment with less invasive. In the future, larger clinical studies and long-term follow-up are needed to validate its safety and efficacy.
Endoscopy_UCTN_Code_TTT_1AO_2AL
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hartel M Wente MN Sido B Carcinoid of the ampulla of Vater J Gastroenterol Hepatol 20052067668110.1111/j.1440-1746.2005.03744.x 15853978 · doi ↗ · pubmed ↗
- 2Vanoli A Grami O Klersy C Ampullary Neuroendocrine Neoplasms: Identification of Prognostic Factors in a Multicentric Series of 119 Cases Endocr Pathol 20223327428810.1007/s 12022-022-09720-635553369 PMC 9135850 · doi ↗ · pubmed ↗
- 3Guo CG Ng HI Liu Y Laparoscopic endoscopic cooperative surgery for the duodenal neuroendocrine tumor: a single-center case series (How I Do It)Int J Surg 20231091835184110.1097/JS 9.000000000000044037300883 PMC 10389388 · doi ↗ · pubmed ↗