Contrast-enhanced endoscopic ultrasound-guided additional ethanol ablation after early detection of occult residual pancreatic insulinoma
Ryo Sugiura, Masaki Kuwatani, Kazumichi Kawakubo, Shoya Shiratori, Soichiro Oda, Katsuma Nakajima, Naoya Sakamoto

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Fig. 1
Fig. 1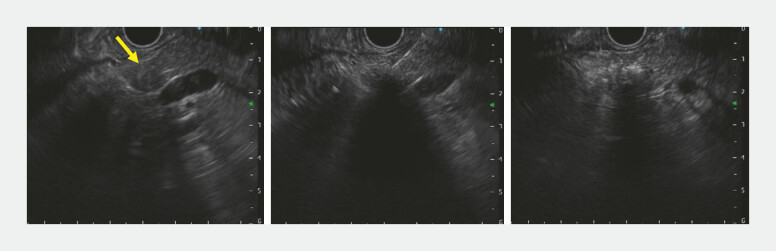 Fig. 2
Fig. 2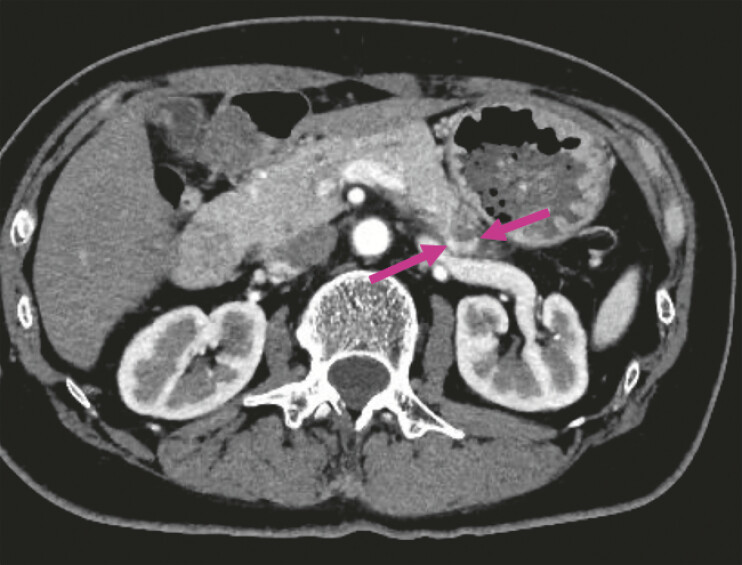 Fig. 3
Fig. 3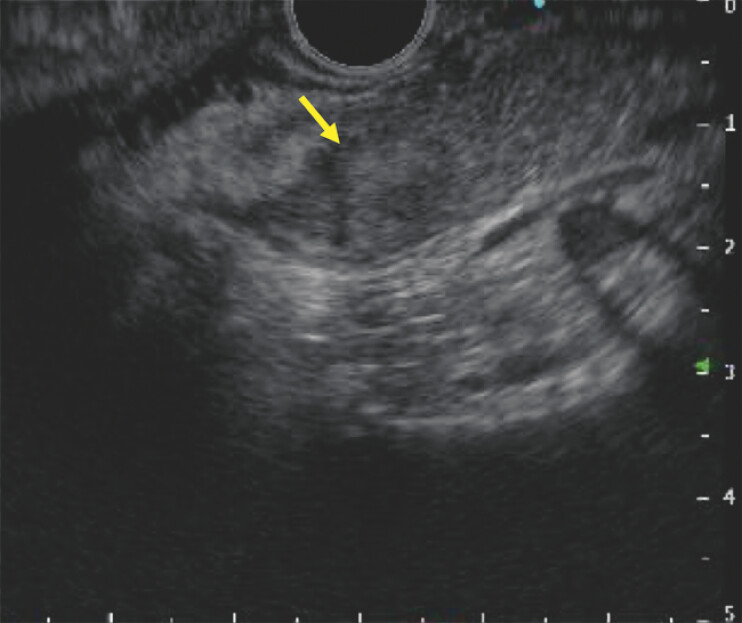 Fig. 4
Fig. 4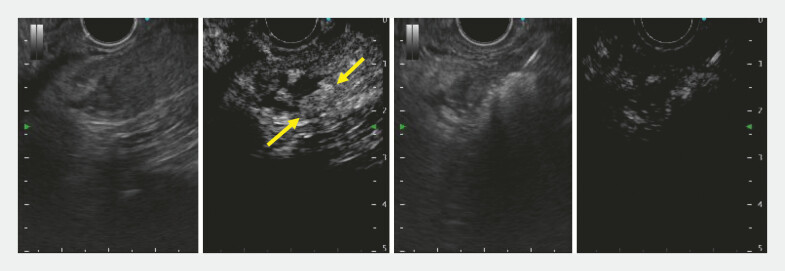 Fig. 5
Fig. 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeuroendocrine Tumor Research Advances · Pancreatic and Hepatic Oncology Research · Gastrointestinal Tumor Research and Treatment
The usefulness of endoscopic ultrasound (EUS)-guided ethanol ablation (EUS-EA) for small non-functional pancreatic neuroendocrine neoplasms and insulinomas has been reported 1 2 . Even when sufficient ablation appears achieved, additional ablation is sometimes required within 3–5 days 1 . However, additional treatment can be difficult when residual lesions are not identifiable on conventional EUS. We report a case with occult residual insulinoma after EUS-EA that was undetectable on conventional EUS but identified by contrast-enhanced EUS (CE-EUS), enabling additional ethanol ablation.
A 57-year-old woman was referred for an insulinoma causing recurrent hypoglycemia. Contrast-enhanced computed tomography (CE-CT) showed a 10-mm tumor in the pancreatic tail with early enhancement ( Fig. 1 ). EUS-EA was performed. The tumor was punctured with a 25-gauge needle filled with undiluted ethanol (99.5% v/v) without a stylet, and 1.7 mL was injected until the lesion became hyperechoic ( Fig. 2 ). The needle was left in place for 1 minute and withdrawn. CE-CT 3 days later demonstrated an early-enhancing area at the lesion margin, suggestive of residual tumor ( Fig. 3 ). As the patient continued occasional hypoglycemia, additional EUS-EA was planned. Conventional EUS showed a heterogeneous echo pattern, making localization difficult ( Fig. 4 ). After intravenous perflubutane injection, the ablated area showed no enhancement, whereas the residual tumor became clearly visible on CE-EUS, allowing additional ethanol ablation with 1.0 mL ( Video 1 ; Fig. 5 ). CE-CT 3 months later revealed no residual tumor, and no further hypoglycemic episodes were observed.
Contrast-enhanced computed tomography demonstrated a 10-mm tumor (arrow) in the pancreatic tail with early enhancement.
(Left) EUS showed a nearly round pancreatic tumor (arrow). (Middle) EUS-guided ethanol ablation was performed. (Right) The tumor showed uniform hyperechoic changes after EUS-guided ethanol ablation. EUS, endoscopic ultrasound.
An early-enhancing area (arrow) at the lesion margin on contrast-enhanced computed tomography performed 3 days after the procedure.
EUS demonstrated a heterogeneous echo pattern in the tumor area (arrow) after the initial procedure, making localization of residual tumor difficult. EUS, endoscopic ultrasound.
Contrast-enhanced endoscopic ultrasound-guided additional ethanol ablation performed after detection of an occult residual pancreatic tumor.Video 1
(Left) Contrast-enhanced endoscopic ultrasound visualized the residual tumor (arrow). (Right) Additional endoscopic ultrasound-guided ethanol ablation was performed on the residual tumor.
Several reports have demonstrated the utility of CE-EUS for early evaluation of residual tumor after EUS-guided radiofrequency ablation of pancreatic neoplasms 3 4 , whereas, to our knowledge, no such reports exist for EUS-EA. Therefore, CE-EUS should be considered when residual tumor after EUS-EA is difficult to delineate. Treatment options for insulinomas include surgery, medical therapy, or minimally invasive approaches such as EUS-EA, which can be considered a less invasive alternative for selected small insulinomas.
Endoscopy_UCTN_Code_TTT_1AS_2AD Endoscopy_UCTN_Code_TTT_1AS_2AI
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Matsumoto K Kato H Itoi T Efficacy and safety of endoscopic ultrasonography-guided ethanol injections of small pancreatic neuroendocrine neoplasms: a prospective multicenter study Endoscopy 20255732132910.1055/a-2452-460739454635 PMC 11997695 · doi ↗ · pubmed ↗
- 2Yan Z Zhu C Wu XA single-center experience on endoscopic ultrasonography-guided ethanol ablation of insulinomas Pancreatology 2023239810410.1016/j.pan.2022.12.00736577553 · doi ↗ · pubmed ↗
- 3Choi JH Seo DW Song TJ Utility of contrast-enhanced harmonic endoscopic ultrasound for the guidance and monitoring of endoscopic radiofrequency ablation Gut Liver 20201482683210.5009/gnl 1912332000466 PMC 7667920 · doi ↗ · pubmed ↗
- 4Barthet M Giovannini M Gasmi M Long-term outcome after EUS-guided radiofrequency ablation: Prospective results in pancreatic neuroendocrine tumors and pancreatic cystic neoplasms Endosc Int Open 20219 E 1178 E 118510.1055/a-1479-219934447860 PMC 8383082 · doi ↗ · pubmed ↗