Conversion from vertical to tangential view using the anchor traction method in colorectal endoscopic submucosal dissection
Keisaku Yamada, Masahiro Tajika, Tsutomu Tanaka, Nobuhito Ito, Akihiro Takagi, Yasumasa Niwa

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
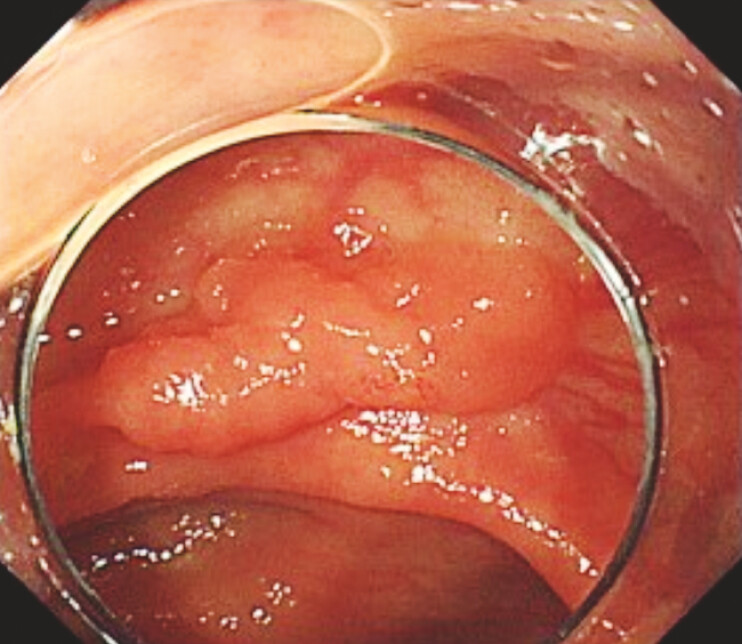 Fig. 1
Fig. 1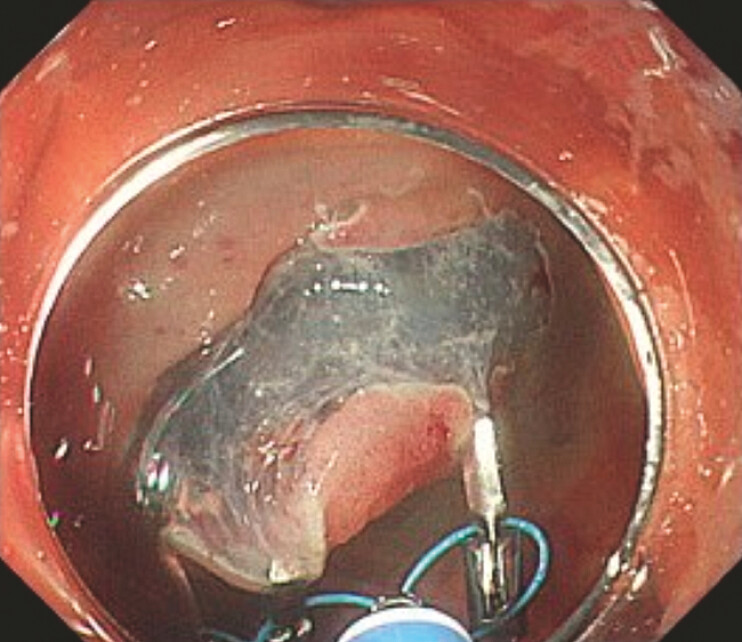 Fig. 2
Fig. 2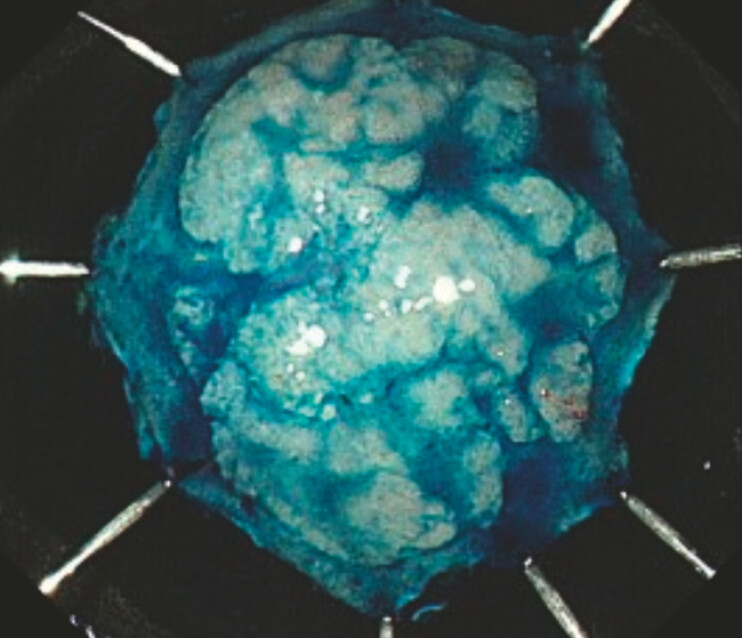 Fig. 3
Fig. 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastric Cancer Management and Outcomes · Esophageal Cancer Research and Treatment · Enhanced Recovery After Surgery
In colorectal endoscopic submucosal dissection (ESD), achieving a tangential approach to the lesion facilitates safe and effective dissection by providing a stable view of the submucosal layer. We developed a novel traction technique using a multi-loop traction device (MLTD; Boston Scientific Co., Ltd, Tokyo, Japan) that enables traction at three points, termed the “anchor traction method” 1 2 3 . Here, we report a case in which the anchor traction method enabled safe and effective dissection by converting the endoscopic view from vertical to tangential during colorectal ESD.
A 68-year-old woman presented with a 20-mm IIa lesion in the ascending colon ( Fig. 1 ) and underwent ESD ( Video 1 ). After a full circumferential incision was made, submucosal dissection was attempted; however, it was difficult to proceed because the lesion was vertically confronted with the endoscope. As submucosal dissection was technically difficult, traction was applied using the anchor traction method. The middle loop of the MLTD was attached to a reopenable clip (SureClip Eco; MicroTech, Nanjing, China), and the two additional loops were then anchored to the lesion, as previously described for the anchor traction method.
The lesion was a 20mm IIa lesion at the ascending colon.
An useful method for lesions that are vertically confronted with the endoscope.Video 1
The use of the anchor traction method converted the lesion’s orientation to a tangential angle ( Fig. 2 ), resulting in easier and safer submucosal dissection, and the en bloc resection was completed ( Fig. 3 ). In this method, three-point traction with a shorter traction length enables strong traction of the entire lesion and transforms the endoscopic approach from a vertical to a tangential view. This technique is particularly useful for lesions that are vertically confronted with the endoscope.
The anchor traction method converted the lesion’s orientation to a tangential angle, resulting in easier and safer submucosal dissection.
Pathological analysis revealed that the lesion was a 22 × 15 mm high grade dysplasia with negative margins.
Endoscopy_UCTN_Code_TTT_1AQ_2AD_3AD
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Yamada K Tajika M Tanaka TA novel traction method using a multi-loop traction device in colorectal endoscopic submucosal dissection: Anchor traction method Endoscopy 202456 E 780E 78110.1055/a-2408-978739299280 PMC 11412764 · doi ↗ · pubmed ↗
- 2Yamada K Tajika M Tanaka T"Double anchor traction method" for large colorectal lesion in colorectal endoscopic submucosal dissection Endoscopy 202557 E 1001 E 100210.1055/a-2689-361740907557 PMC 12410999 · doi ↗ · pubmed ↗
- 3Yamada K Tajika M Tanaka T Modified anchor traction method allows safe colorectal endoscopic submucosal dissection: the T-shaped traction method Endoscopy 202557 E 64E 6510.1055/a-2512-429739875132 PMC 11774657 · doi ↗ · pubmed ↗