Pulmonary Nodular Lymphoid Hyperplasia Presenting With a Reversed Halo Sign
Takafumi Yamano, Shohei Yano, Yuki Yoshida, Moon Hee Hwang

TL;DR
A rare lung condition called pulmonary nodular lymphoid hyperplasia was found to present with a reversed halo sign, a feature previously not associated with this disease.
Contribution
This is the first reported case linking pulmonary nodular lymphoid hyperplasia with the reversed halo sign on chest CT.
Findings
A case of pulmonary nodular lymphoid hyperplasia presented with a reversed halo sign on imaging.
Histological analysis confirmed a polyclonal reactive lymphoid proliferation without IgG4-positive cell increase.
The case suggests that PNLH should be considered in the differential diagnosis of the reversed halo sign.
Abstract
The reversed halo sign is observed in a broad spectrum of lung diseases, most commonly organising pneumonia, but it has not been reported in pulmonary nodular lymphoid hyperplasia. Herein, we describe the first case of pulmonary nodular lymphoid hyperplasia presenting with a reversed halo sign. We report a case of pulmonary nodular lymphoid hyperplasia (PNLH) presenting with a reversed halo sign on chest computed tomography. Video‐assisted thoracoscopic wedge resection confirmed a polyclonal reactive lymphoid proliferation without an increase in IgG4‐positive cells. This case highlights that PNLH should be considered in the differential diagnosis of the reversed halo sign and that histologic confirmation is essential.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
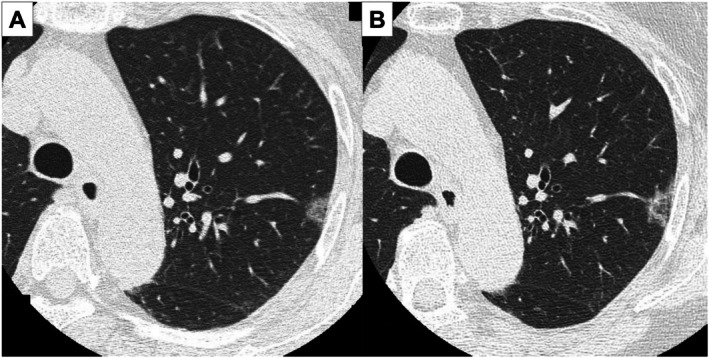 Figure 1
Figure 1 Figure 2
Figure 2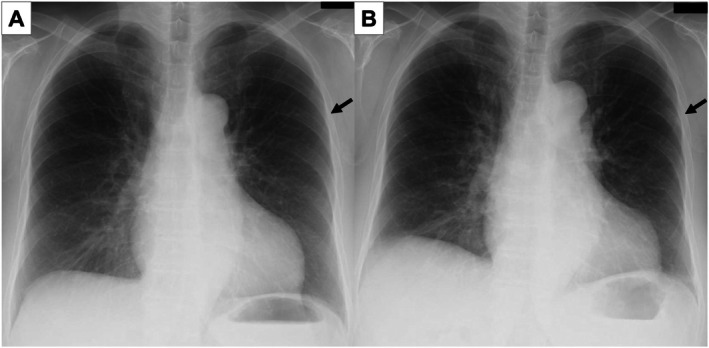 Figure 3
Figure 3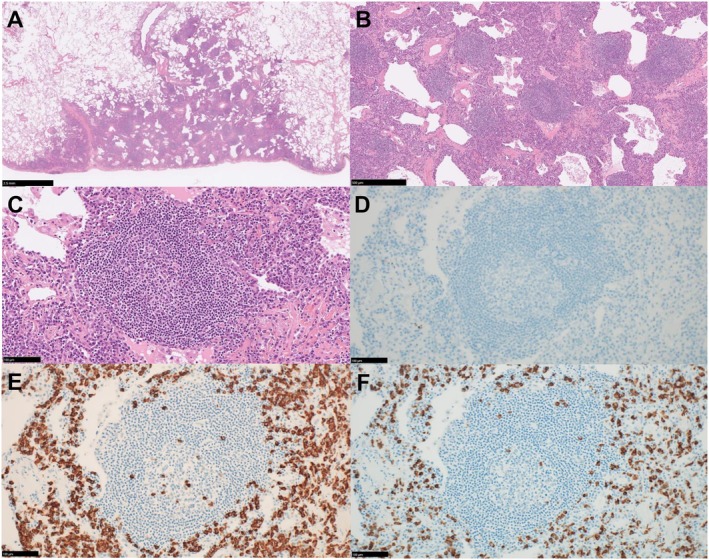 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInterstitial Lung Diseases and Idiopathic Pulmonary Fibrosis · Medical Imaging and Pathology Studies · IgG4-Related and Inflammatory Diseases
A 76‐year‐old woman, followed up for a left upper lobe ground‐glass nodule detected 7 years earlier, presented with interval enlargement following chest radiography (Figure 1). Chest computed tomography revealed an enlarged ground‐glass nodule with a reversed halo sign (Figure 2). A video‐assisted thoracoscopic wedge resection was performed. Histological analysis revealed clustered reactive lymphoid follicles with perifollicular plasmacytosis. IgG4‐positive cells were not increased (IgG4/IgG < 1%; 0–1/HPF). The κ/λ ratio was 2–3:1, indicating polyclonality and supporting a diagnosis of pulmonary nodular lymphoid hyperplasia (Figure 3). At 9 months follow‐up, there was no recurrence. The reversed halo sign, classically associated with organising pneumonia, also occurs in infections, pulmonary infarction, and granulomatous disease [1]. Pulmonary nodular lymphoid hyperplasia is a rare reactive lymphoproliferative lesion that usually presents as solitary or multiple pulmonary nodules. Pulmonary nodular lymphoid hyperplasia requires distinction from IgG4‐related disease and mucosa‐associated lymphoid tissue lymphoma [2]; immunostaining in our case excluded both. A reversed halo sign, not previously described in patients with pulmonary nodular lymphoid hyperplasia, could be explained by intralesional heterogeneity, with relatively lower central cellularity than peripheral cellularity. The differential diagnosis of reversed halo sign should include pulmonary nodular lymphoid hyperplasia, and tissue diagnosis is essential.
Author Contributions
Takafumi Yamano drafted the manuscript and collected the data. Shohei Yano, Yuki Yoshida, and Moon Hee Hwang reviewed and edited the manuscript. All authors approved the final version of the manuscript.
Funding
The authors have nothing to report.
Ethics Statement
This case report was approved by the Ethics Committee of the Osaka Red Cross Hospital (approval number: J‐0779). This study was conducted in accordance with the principles of the Declaration of Helsinki.
Consent
The authors declare that written informed patient consent was obtained for the publication of this manuscript and the accompanying images, and attest that the form used to obtain consent from the patient complies with the journal requirements, as outlined in the author guidelines.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1V. N. Maturu and R. Agarwal , “Reversed Halo Sign: A Systematic Review,” Respiratory Care 59, no. 9 (2014): 1440–1449, 10.4187/respcare.03020.24782557 · doi ↗ · pubmed ↗
- 2M. Yell and F. G. Rosado , “Pulmonary Nodular Lymphoid Hyperplasia,” Archives of Pathology & Laboratory Medicine 143, no. 9 (2019): 1149–1153, 10.5858/arpa.2018-0188-RS.30720334 · doi ↗ · pubmed ↗