Evolving antimicrobial resistance patterns in group B streptococci: A five-year study in a high-risk pregnancy referral center in northeastern Brazil
Jorhanna Isabelle Araújo de Brito Gomes, Suellen Bernardo de Queiroz, Carlos Gabriel Andrade Barbosa, Larissa Rodrigues Santos Silva, Patrícia Urquiza Lundgren, Eduardo Sergio Soares Sousa, Eloiza Helena Campana, Vinicius Pietta Perez

TL;DR
This study tracks changing antibiotic resistance in group B streptococci among pregnant women in Brazil over five years.
Contribution
The study provides a five-year analysis of GBS colonization and resistance patterns in a high-risk pregnancy center in Brazil.
Findings
GBS colonization rate was 12% among pregnant women tested.
Resistance to tetracycline was highest at 82.3%, with tet(M) being the most common resistance gene.
Erythromycin resistance increased over time, potentially affecting clindamycin efficacy.
Abstract
Streptococcus agalactiae (commonly referred to as group B streptococci [GBS]) is a leading cause of neonatal infection. Surveillance of colonization in pregnant women and the use of intrapartum antibiotic prophylaxis (IAP) are the primary strategies for preventing early-onset GBS disease. The increasing rate of antibiotic resistance among GBS isolates is a concern for the effectiveness of IAP. Our study aimed to evaluate the prevalence of GBS colonization and characterize antimicrobial resistance patterns over a five-year period in a high-risk pregnancy referral center in Northeastern Brazil. This study was conducted from 2020 to 2024 and included pregnant women at 35-37-week gestation. GBS isolates from anal-vaginal swabs were identified and tested for susceptibility to penicillin or ampicillin, clindamycin, erythromycin, levofloxacin, and tetracycline. Isolates stored from 2021 to…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
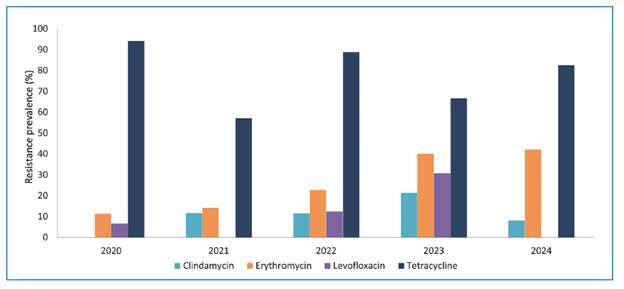 Figure 1
Figure 1- —Paraiba State Research Foundation
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeonatal and Maternal Infections · Maternal and Neonatal Healthcare · Preterm Birth and Chorioamnionitis
INTRODUCTION
Streptococcus agalactiae, commonly referred to as group B streptococci (GBS), is a commensal colonizer of the human genitourinary and gastrointestinal tracts. It is also a significant pathogen associated with neonatal diseases, including sepsis, pneumonia, and meningitis, which often result in neurodevelopmental impairment in survivors1.
Neonatal disease can manifest as early onset infection (EOI) in the first week of life and is associated with vertical transmission during childbirth. To prevent EOI, maternal screening for GBS colonization between 36 and 37 weeks of gestation with administration of intrapartum antibiotic prophylaxis (IAP) to colonized mothers is recommended. Late-onset infection (LOI) occurs between the first week and three months of age, and transmission can be associated with the maternal microbiota or environmental sources2.
Although beta-lactams remain the first-line IAP agents, variations in GBS susceptibility to these antibiotics have been reported worldwide, particularly reduced susceptibility has been sporadically reported3. Resistance to macrolides has prompted revisions to IAP protocols, and susceptibility to clindamycin, the second-line agent, must be confirmed. Furthermore, the use of fluoroquinolones to treat urinary tract infections in many regions is associated with increased resistance, and tetracycline resistance is a common characteristic of GBS strains4.
To optimize IAP protocols and guide treatment strategies, continuous surveillance of GBS antibiotic resistance is therefore essential. In northeastern Brazil, data regarding GBS epidemiology are lacking, and antenatal screening for GBS is recommended only for high-risk pregnancies in Brazil5. Our study aimed to investigate the GBS colonization rate, antimicrobial susceptibility profile, and resistance genotypes to macrolides and tetracyclines in pregnant women at a referral center in northeastern Brazil over a period of five years.
METHODS
Study design and samples
This observational single-center cross-sectional study was conducted between January 2020 and December 2024 at a gynecology and obstetrics referral center for high-risk pregnancies in João Pessoa, PB, northeast Brazil. Pregnant women at gestational age of 35-37 weeks who visited the high-risk antenatal care unit and underwent GBS screening were included in the study. Additionally, isolates identified as GBS and obtained from anal-vaginal swab screenings conducted during the years 2021 and 2024 were transferred into Brain Heart Infusion broth supplemented with 10% glycerol and stored at −20°C. This study was approved by the Hospital Universitário Lauro Wanderley Ethical Committee (Code Number: 3.155.051).
GBS screening, bacterial identification and susceptibility testing
Sample collection was performed using rayon swabs, which were initially inserted approximately 2 cm into the vaginal canal and then gently introduced into the anal sphincter. The swabs were stored in Stuart transport medium and subsequently transferred to tubes containing Todd-Hewitt broth, followed by incubation at 35 ± 1°C for 8 h. After incubation, tubes showing visible growth (turbidity) were inoculated onto blood agar plates and incubated at 35 ± 1°C in a CO_2_ enriched atmosphere for 24-48 h. Beta-hemolytic colonies were selected, and catalase, Christie-Atkins-Munch-Petersen (CAMP), and L-pyrrolidonyl-beta-naphtylamide (PYR) tests were performed for identification. Antimicrobial susceptibility testing was performed for penicillin or ampicillin, clindamycin, erythromycin, levofloxacin, and tetracycline using the disk diffusion method, according to the Brazilian Committee on Antimicrobial Susceptibility Testing (BrCAST) guidelines. These guidelines were based on the European Committee on Antimicrobial Susceptibility Testing (EUCAST) standards.
Detection of resistance genes by polymerase chain reaction (PCR)
PCR assays for the presence of resistance genes and detection of the cfb gene were performed on the stored isolates. One colony from each isolate (2021 and 2024) was transferred to a 10% solution of Chelex-100, vortexed vigorously, and incubated in a dry bath at 95°C for 30 min. The solution was then centrifuged at 4,000 RPM for 30 s, and the supernatant was transferred to a microtube for PCR. All amplification reactions were performed with a total volume of 20 µL using MiniAmp thermal cycler. Two microliters of DNA were added to PCR reaction mix containing 0.20 µM of each primer6 ^-^ 8 (Table 1), 0.2 mM of each dNTP, 1 U Taq polymerase, 2 mM of MgCl_2_, and reaction buffer. The cycling parameters were as follows: 95°C for 1 min, 35 cycles of 95°C for 1 min, annealing for 1 min (Table 1), extension at 72°C for 1 min, and final extension at 72°C for 5 min. The PCR product was run on 2% agarose gel in Tris Acetate EDTA (TAE) buffer, stained with a UV nucleic acid stain, and visualized with a UV trans-illuminator. The results were evaluated according to the expected amplicon sizes (Table 1).
TABLE 1:Oligonucleotide primer sequences for polymerase chain reaction (PCR) assays to detect cfb gene of Streptococcus agalactiae and resistance genes.TargetSequence (5’-3’) Size (bp)Annealing temperature (^o^C)Reference cfb TTTCACCAGCTGTATTAGAAGTA GTTCCCTGAACATTATCTTTGAT15362Kerdsin et al. 2017^6^
erm(A/TR) AACTTGTGGAAATGAGTCAACGG CAGAATCTACATTAGGCTTAGGG37560Pérez-Trallero et al. 2007^7^
erm(B) ATTGGAACAGGTAAAGGGCG GAACATCTGTGGTATGGCG44260Pérez-Trallero et al. 2007^7^
mef(A) AGTATCATTAATCACTAGTGC TTCTTCTGGTACTAAAAGTGG34550Pérez-Trallero et al. 2007^7^
tet(M) GTGGAGTACTACATTTACGAG GAAGCGGATCACTATCTGAG35950Poyart et al. 2003^8^
tet(O) GCGGAACATTGCATTTGAGGG CTCTATGGACAACCCGACAGAAG53850Poyart et al. 2003^8^
Statistical analysis
Data are expressed as absolute and relative frequencies. Chi-square or Fisher’s exact test was used to explore and compare frequencies across different study years. Additionally, binary outcomes (GBS colonization and antibiotic resistance) were subjected to logistic regression analysis to investigate linear trends over the study period. All statistical analyses were conducted using SPSS (version 20.0) for Mac OS (IBM Corporation, Armonk, NY, USA). A 95% confidence interval (CI) was calculated, and the level of significance was set at 0.05.
RESULTS
A total of 1469 anal-vaginal swabs from pregnant women were analyzed. The prevalence of anal-vaginal GBS colonization in our population was 12%, ranging from 17.8% in 2021 to 5.0% in 2023 (P < 0.001), the numbers across the five years are detailed in Table 2. The logistic regression showed a significant trend of reduced colonization over the years (odds ratio [OR] = 0.855; 95% CI = 0.763-0.958; P = 0.007).
TABLE 2:Prevalence of Streptococcus agalactiae colonization in 1,469 high-risk pregnant women (35-37-week gestation) in João Pessoa, PB, Brazil (2020-2024).YearColonized Non-colonized Total n%n% 20203714.222485.826120216117.828282.23432022269.724290.32682023155.028895.030320243812.925687.1294
Of the 177 isolates obtained from colonized pregnant women, all were susceptible to beta-lactams (penicillin and/or ampicillin). Resistance rates to clindamycin, erythromycin, levofloxacin, and tetracyclines are shown in Figure 1. The overall resistance rate against tetracyclines was 82.3% (51/62): 94.1% (16/17) in 2020, 57.1% (4/7) in 2021, 88.9% (8/9) in 2022, 66.7% (4/6) in 2023, and 82.6% (19/23) in 2024 (P = 0.202). The overall resistance rate against erythromycin was 23.6% (39/165): 11.4% (4/35) in 2020, 14.2% (10/60) in 2021, 22.7% (5/22) in 2022, 40% (4/10) in 2023, and 42.1% (16/38) in 2024 (P = 0.010). Clindamycin resistance rate was 9.3% overall (16/172): 0% (0/35) in 2020, 11.7% (7/60) in 2021, 11.5% (3/26) in 2022, 21.4% (3/14) in 2023, and 8.1% (3/37) in 2024 (P = 0.085). The overall resistance rate against levofloxacin was 5.4% (6/111): 6.7% (1/15) in 2020, 0% (0/49) in 2021, 12.5% (1/8) in 2022, 30.8% (4/13) in 2023, and 0% (0/26) in 2024 (P < 0.001). Ten isolates, 6.1% (10/165), presented susceptibility only with increased exposure to erythromycin: 2.9% (1/35) in 2020 and 15% (9/60) in 2021.
FIGURE 1:Antibiotic resistance rates and trends among Streptococcus agalactiae isolates from high-risk pregnant women (35-37-week gestation) in João Pessoa, PB, Brazil (2020-2024).
A significant increase in erythromycin resistance between 2020 to 2024 was observed (OR = 1.556; 95% CI = 1.211-2.000; P = 0.001). However, logistic regression analysis showed no statistically significant increase in resistance over the five-year period to clindamycin (OR = 1.212; 95% CI = 0.854-1.720; P = 0.282), levofloxacin (OR = 1.261; 95% CI = 0.717-2.217; P = 0.422), and tetracycline (OR = 0.883; 95% CI = 0.591-1.319; P = 0.543).
To determine the resistance genotypes against macrolides and tetracyclines during the study period, anal-vaginal isolates from two years (2021 and 2024) were selected to evaluate the presence of mef(A), erm(A/TR), erm(B), tet(M), and tet(O) genes. Of the 61 and 38 isolates collected in 2021 and 2024, respectively, 36 and 21 isolates were stored and analyzed using PCR. The prevalence rates were as follows: for mef(A) 19.3% (19.4% in 2021 and 19.0% in 2024), for erm(B) 8.8% (8.3% in 2021 and 9.5% in 2024), for erm(A/TR) 3.5% (2.8% in 2021 and 4.8% in 2024), for tet(M) 82.4% (80.5% in 2021 and 85.7% in 2024), and for tet(O) 5.3% (5.5% in 2021 and 4.8% in 2024). Table 3 presents the percentages for each genotype among the strains.
TABLE 3:Genotypes of resistant Streptococcus agalactiae obtained from high-risk pregnant women (35-37-week gestation) in João Pessoa, PB, Brazil.Antibiotic2021 2024 Total n%n%n% Macrolides
mef(A) 7^a^ 70.0^a^ 466.71168.6^a^
erm(A/TR) 110.01^b^ 16.7^b^ 212.5^b^
erm(B) 3^a^ 30.0^a^ 2^b^ 33.3^b^ 531.3^ab^
Tetracyclines
tet(M) 2893.31894.74693.9 tet(O) 26.715.336.1 ^a^ isolate HU75 harbored mef and erm(B). ^b^ isolate HU206 carried erm(B) and erm(A/TR).
DISCUSSION
Our five-year observational study provides valuable data on the prevalence and antimicrobial resistance of GBS among pregnant women in João Pessoa, Brazil. Maternal colonization rates vary regionally; a meta-analysis estimated a global prevalence of 18%, ranging from 11% to 35%, and a prevalence of 15.7% in South America9. The overall colonization rate of 12% in our population aligns with previous studies in Brazil, which reported a prevalence of 4.2-28.4% in the last decade, mainly in southern and southeastern Brazil10. We observed significant year-to-year variation, with rates peaking at 17.8% and declining to 5%, which was also observed in a single-center study in Rio de Janeiro, Brazil, from 13.8% in 2019 to 5.3% in 2020, suggesting that behavioral and healthcare changes during the COVID-19 pandemic (March 2020 to May 2023) may have affected colonization rates5. Notably, in our population, the peak prevalence was observed in 2021, followed by a significant reduction in 2023, potentially reflecting behavioral changes in the local population during the post-pandemic period.
Culture methods for GBS screening present low sensitivity, estimated at 54-70%, which is mainly due to non-hemolytic strains that cannot be identified using blood agar. The use of chromogenic agar and Nucleic Acid Amplification Tests (NAATs) has increased GBS detection from 18.8% to 24.4% and from 15% to 31.5%, respectively11 ^-^ 12. In Brazil, owing to the need for specialized infrastructure and high costs, the use of NAATs and chromogenic agar for GBS screening is restricted, which is likely related to the reduced prevalence observed in the low- and middle-income regions of Brazil when compared with data from southern and southeastern Brazil.
All isolates in our study were susceptible to beta-lactam antibiotics, underscoring the continued efficacy of penicillin and ampicillin for empirical IAP. However, erythromycin is no longer recommended for IAP13. This is due to the increasing resistance of GBS to macrolides, mediated by the efflux pump encoded by mef(A) gene or erythromycin methylases (erm genes).
We also observed a consistent and statistically significant increase in erythromycin resistance, from 11.4% in 2020 to 42.1% in 2024. A recent report from southeastern Brazil revealed a trend of macrolide resistance (from 17% to 37%) during the pandemic period. This increase in prevalence was mostly associated with mef(A) gene dissemination (from 66.7% to 80.0%) and may be related to the indiscriminate use of azithromycin during the pandemic14. However, we did not observe any changes in the prevalence of resistance genes among isolates from 2021 to 2024, and mef(A) was the most frequent resistance gene during both the periods (70% versus 66.7%), followed by erm(B) and erm(A/TR).
The mef(A) gene is related to the M phenotype (resistance only to macrolides) and has only slight effect on GBS disease. However, erm genes confer the MLSb phenotype (combined resistance to macrolides-lincosamides-streptogramin) and mediate resistance to clindamycin, a suitable second-line IAP and an important therapy for invasive GBS disease. Resistance to clindamycin is also associated with an infrequent L phenotype (resistance only to lincosamides), driven by lnuB, lsaC, and lsaE genes3.
Our data show a concerning clindamycin resistance from 0% in 2020 to a peak of 21.4% in 2023, and an overall resistance rate of 9.3%. Conversely, no significant increase in clindamycin resistance was observed during the study period. In Brazil, clindamycin resistance over the last ten years (2-6.9%)4 ^,^ 5 ^,^ 14 ^-^ 15 has remained below the global estimate of 29.3% reported in a recent meta-analysis16. Furthermore, studies have reported a decreasing trend or stabilization of resistance to clindamycin in Brazil throughout the pandemic period5 ^,^ 14. Across the five years of our study, 93.7% of clindamycin-resistant isolates presented the MLSb phenotype related to the erm genes, and the L phenotype was observed only in one isolate in 2023. Indeed, a previous study using whole-genome sequencing in our setting did not report the L phenotype; however, it revealed the presence of lnuB and lsaE in two GBS strains harboring a fragment sequence related to a plasmid from Enterococcus faecium 4. In summary, our data suggest that the increasing prevalence of erythromycin-resistant strains, some of which harbor erm genes, could be the primary cause of clindamycin resistance in our population, and further studies should evaluate this important issue.
Fluoroquinolones, such as levofloxacin, are not indicated for IAP; however, they are frequently prescribed for urinary tract infections. Levofloxacin is included in the World Health Organization’s watch group because of its high resistance potential, driven primarily by the accumulation of point mutations in gyr(A) and par(C) genes. Levofloxacin-resistant GBS remains relatively uncommon, with estimated resistance rates of 8.6%16 and up to 5% in Brazil15, which is consistent with the rate of 5.4% observed in our study. Nonetheless, we noted significant year-to-year variations. In two years (2021 and 2024), no resistant isolates were detected; however, a peak was observed in 2023. Given that fluoroquinolone resistance progresses from low to high level through stepwise accumulation of mutations17, the observed pattern is likely linked to prior fluoroquinolone exposure in patients, which could promote the stepwise development of resistance to levofloxacin.
Resistance to tetracyclines is estimated to be 80.1%16, primarily mediated by the tet(M) gene and less frequently by tet(O). Although tetracyclines are not used to treat GBS infections, some studies suggest that the acquisition of tet(M) contributes to the stepwise selection and dissemination of virulent GBS lineages18. Data from our five-year study consistently revealed a high tetracycline resistance rate of 82.3%, driven primarily by the presence of tet(M) (93.9%), followed by tet(O) (6.1%).
Despite the significant findings obtained from this single-center study of a high-risk pregnancy population in northeast Brazil, there are limitations in drawing certain conclusions. As mentioned previously, the culture method employed showed low sensitivity, thereby limiting isolate recovery. Additionally, owing to convenience sampling for genotyping, only few anovaginal isolates were obtained in 2020, 2022, and 2023. Consequently, these isolates were not included in the study, resulting in a limited evaluation of their molecular epidemiology. Additionally, there were no patient data correlating with prior use of antibiotics.
In conclusion, our findings underscore the dynamics of GBS colonization among high-risk pregnant women in northeast Brazil, showing a reduced colonization rate in the local population during the post-pandemic period. Although penicillin and ampicillin remain effective for IAP, continuous surveillance of antibiotic resistance in GBS is essential to guide IAP and treatment strategies. Furthermore, the observed increasing macrolide resistance pattern in our setting over the past five years could potentially compromise clindamycin efficacy, particularly through its association with the presence of erm genes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kohli-Lynch M Russell NJ Seale AC Dangor Z Tann CJ Baker CJ Neurodevelopmental Impairment in Children After Group B Streptococcal Disease Worldwide: Systematic Review and Meta-analyses Clin Infect Dis 2017652 S 190S 1992911733110.1093/cid/cix 663PMC 5848372 · doi ↗ · pubmed ↗
- 2Pereira MDCA Hilário FF Campana EH Sousa ESS Perez VP Distribution of group B streptococci serotypes on women nasopharynx Braz J Infect Dis 20242861044691044693957704110.1016/j.bjid.2024.104469 PMC 11616486 · doi ↗ · pubmed ↗
- 3Metcalf BJ Chochua S Gertz RE Hawkins PA Ricaldi J Li Z Short-read whole genome sequencing for determination of antimicrobial resistance mechanisms and capsular serotypes of current invasive Streptococcus agalactiae recovered in the USA Clinical Microbiology and Infection 2017238574.e 7-574.e 1410.1016/j.cmi.2017.02.02128257899 · doi ↗ · pubmed ↗
- 4Perez VP Torini LR Manieri FZ de Queiroz SB Gomes JIAB Santos L Filho Genomic Diversity, Virulome, and Resistome of Streptococcus agalactiae in Northeastern Brazil: Are Multi-Host Adapted Strains Rising?Pathogens 20251432922924013777710.3390/pathogens 14030292 PMC 11945199 · doi ↗ · pubmed ↗
- 5Costa NS Rio-Tinto A Pinto IBF Alvim DC Rocha AA Oliveira LMA Changes in Group B Streptococcus Colonization among Pregnant Women before and after the Onset of the COVID-19 Pandemic in Brazil Pathogens 202227101104110410.3390/pathogens 11101104 PMC 960965136297161 · doi ↗ · pubmed ↗
- 6Kerdsin A Hatrongjit R Hamada S Akeda Y Gottschalk M Development of a multiplex PCR for identification of β-hemolytic streptococci relevant to human infections and serotype distribution of invasive Streptococcus agalactiae in Thailand Mol Cell Probes 20173610142866661910.1016/j.mcp.2017.06.007 · doi ↗ · pubmed ↗
- 7Pérez-Trallero E Montes M Orden B Tamayo E García-Arenzana JM Marimón JM Phenotypic and Genotypic Characterization of Streptococcus pyogenes Isolates Displaying the MLSB Phenotype of Macrolide Resistance in Spain, 1999 to 2005 Antimicrob Agents Chemother 2007514122812331724214210.1128/AAC.01054-06PMC 1855467 · doi ↗ · pubmed ↗
- 8Poyart C Jardy L Quesne G Berche P Trieu-Cuot P Genetic basis of antibiotic resistance in Streptococcus agalactiae strains isolated in a French hospital Antimicrob Agents Chemother 20034727947971254369510.1128/AAC.47.2.794-797.2003 PMC 151750 · doi ↗ · pubmed ↗