Unplanned intensive care unit admission after elective colon cancer resection: population-based registry study
Sofia Dahlberg, Tomas Vedin, Ingvar Syk, Emma Larsson, Niklas Nielsen, Henrik Bergenfeldt

TL;DR
A study in Sweden found that 5.6% of patients who had elective colon cancer surgery needed unexpected intensive care, with higher mortality and complications, especially when surgery was required again.
Contribution
This study provides population-based insights into the incidence and outcomes of unplanned ICU admissions after elective colon cancer surgery.
Findings
Unplanned ICU admission occurred in 5.6% of patients after elective colon cancer surgery.
Patients requiring surgical reintervention had worse outcomes and higher mortality rates.
Laparoscopic surgery was linked to fewer ICU admissions and lower mortality.
Abstract
The incidence, aetiology, and outcome of unplanned intensive care unit admission after elective colon cancer surgery remain unclear. This study investigated the incidence of, and factors associated with, unplanned intensive care unit admission following elective colon cancer resection in Sweden. This nationwide retrospective registry study included adult patients undergoing elective colon cancer resection with curative intent in Sweden between 2010 and 2019. Patients with distant metastases, or rectal or appendiceal tumours were excluded. Data from the Swedish Colorectal Cancer Registry and the Swedish Intensive Care Registry were analysed. Patients not requiring intensive care unit admission served as controls. Of 23 891 patients, 1343 (5.6%) required unplanned intensive care unit admission. These patients were older, had more co-morbidities, and were more likely to undergo open…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
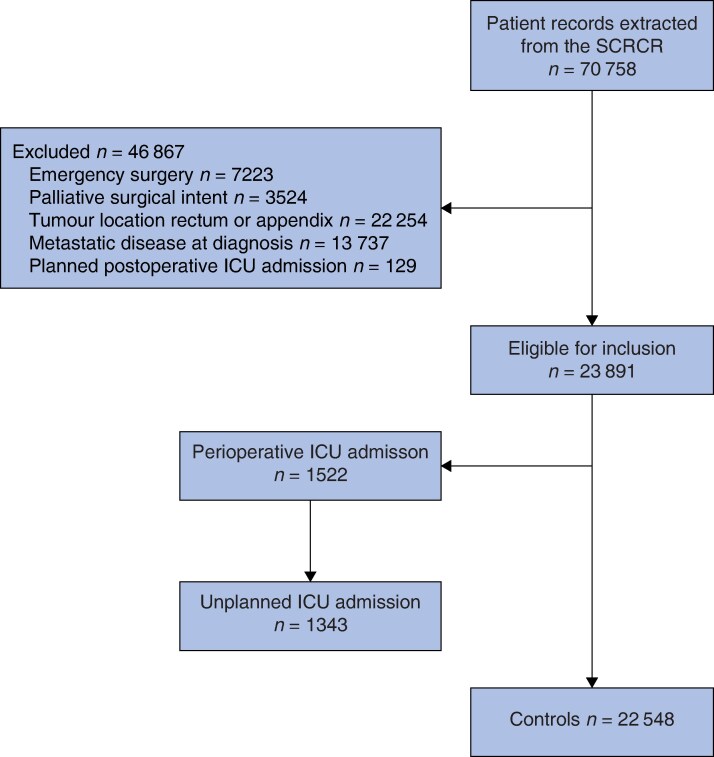 Fig. 1
Fig. 1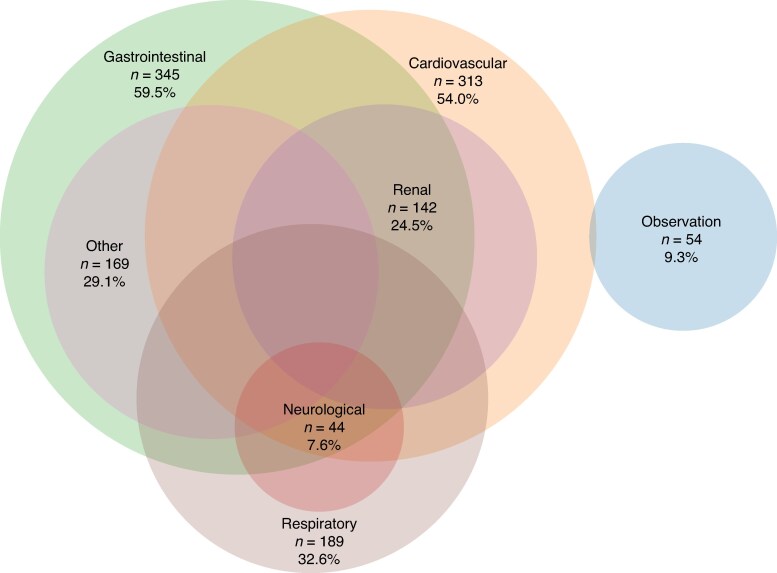 Fig. 2
Fig. 2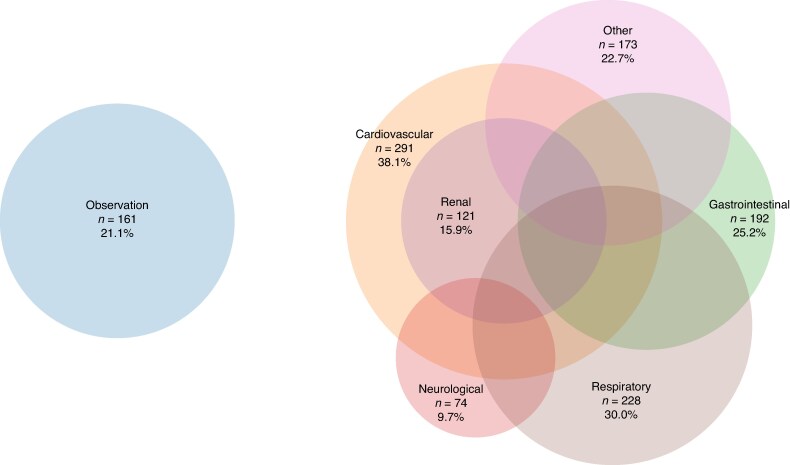 Fig. 3
Fig. 3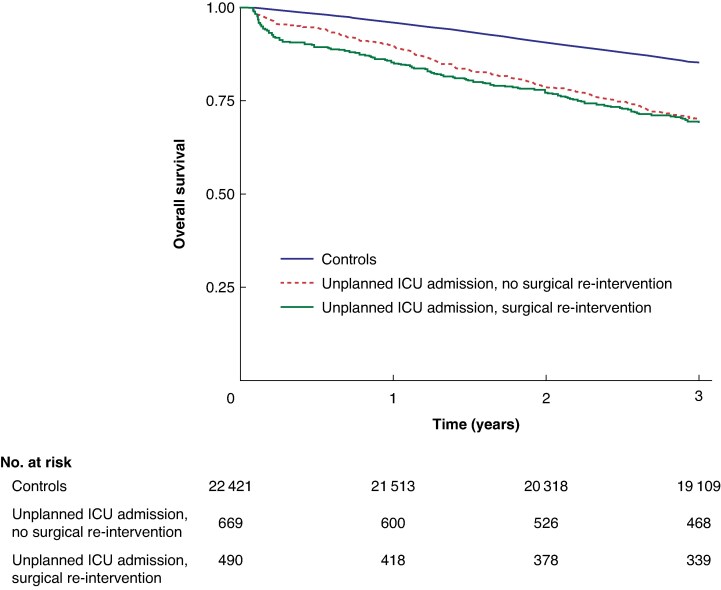 Fig. 4
Fig. 4| ICU | Controls | |
|---|---|---|
|
| ||
| Age (years), median (i.q.r.) | 77 (71–83) | 74 (66–80) |
| Missing | 0 (0%) | 0 (0%) |
| Sex | ||
| Male | 780 (58.0%) | 10 945 (48.5%) |
| Female | 563 (42.0%) | 11 603 (51.5%) |
| Missing | 0 (0%) | 0 (0%) |
| Body mass index (kg/m2), median (i.q.r.) | 26.0 (23.1–29.9) | 25.6 (23.1–28.7) |
| Missing | 58 (4.3%) | 705 (3.1%) |
| ASA fitness grade | ||
| I | 52 (3.9%) | 2746 (12.2%) |
| II | 513 (38.2%) | 12 113 (53.7%) |
| III | 659 (49.1%) | 6821 (30.3%) |
| IV | 95 (7.1%) | 474 (2.1%) |
| V | 0 (0%) | 4 (0.02%) |
| Missing | 23 (1.7%) | 390 (1.7%) |
|
| ||
| pT1–3 N0 | 757 (56.4%) | 12 496 (55.4%) |
| pT1–3 N1–2 | 326 (24.3%) | 5956 (26.4%) |
| pT4 N0–2 | 245 (18.3%) | 3781 (16.8%) |
| Missing | 14 (1.0%) | 315 (1.4%) |
|
| ||
| Surgical approach | ||
| Open | 1070 (79.7%) | 14 855 (65.9%) |
| Laparoscopic | 162 (12.1%) | 5433 (24.1%) |
| Robot-assisted | 26 (1.9%) | 831 (3.7%) |
| Laparoscopic converted to open | 79 (5.9%) | 1309 (5.8%) |
| Type of surgery | ||
| Hartmann’s operation | 40 (3.0%) | 347 (1.5%) |
| High anterior resection | 59 (4.4%) | 1093 (4.9%) |
| Ileocaecal resection | 16 (1.2%) | 95 (0.4%) |
| Right hemicolectomy | 677 (50.5%) | 12 176 (54.0%) |
| Local excision | 1 (0.07%) | 21 (0.09%) |
| Other | 11 (0.07%) | 86 (0.4%) |
| Transverse colon resection | 29 (2.1%) | 331 (1.5%) |
| Left hemicolectomy | 175 (13.0%) | 2237 (9.9%) |
| Sigmoid colon resection | 227 (16.9%) | 5185 (23.0%) |
| Missing | 1 (0.07%) | 145 (0.%) |
| Permanent ostomy | 153 (11.4%) | 1293 (5.7%) |
| Missing | 7 (0.5%) | 189 (0.8%) |
| Perioperative blood loss (ml), median (i.q.r.) | 150 (50–400) | 100 (40–200) |
| Missing | 42 (3.1%) | 791 (3.5%) |
| Duration of operation (minutes), median (i.q.r.) | 186 (141–255) | 172 (133–223) |
| Missing | 26 (1.9%) | 430 (1.9%) |
| Intraoperative perforation | 33 (2.5%) | 269 (1.2%) |
| Missing | 14 (1.0%) | 223 (01.0%) |
| Type of perforation | ||
| Iatrogenic | 11 (0.8%) | 86 (0.4%) |
| Spontaneous | 2 (0.2%) | 43 (0.2%) |
| Unspecified | 4 (0.3%) | 21 (0.09%) |
| Unplanned ICU admission |
| ||
|---|---|---|---|
| Surgical reintervention | No surgical reintervention | ||
| Age (years), median (i.q.r.) | 76 (69–82) | 78 (72–83) | < 0.001† |
|
| < 0.001 | ||
| I | 29 (5.0%) | 23 (3.0%) | |
| II | 248 (42.8%) | 266 (34.9%) | |
| III | 270 (46.6%) | 389 (51.0%) | |
| IV | 24 (4.1%) | 71 (9.3%) | |
| V | 0 (0%) | 0 (0%) | |
| Missing | 9 (1.6%) | 14 (1.8%) | |
|
| 0.001 | ||
| Male | 365 (62.9%) | 414 (54.3%) | |
| Female | 215 (37.1%) | 349 (45.7%) | |
|
| |||
| Non-invasive ventilation | 114 (19.7%) | 125 (16.4%) | 0.122 |
| Invasive ventilation | 288 (49.7%) | 161 (21.1%) | < 0.001 |
| CRRT | 58 (10.0%) | 19 (2.5%) | < 0.001 |
|
| 64 (56–73) | 58 (50–66) | < 0.001† |
| Missing | 19 (0.03%) | 18 (0.02%) | |
| SAPS3 EMR (%), median (i.q.r.) | 38 (30–47) | 32 (24–40) | < 0.001† |
| Length of ICU stay (days), median (i.q.r.) | 3 (1–7) | 1 (1–2) | < 0.001† |
| Interval from primary surgery to ICU admission (days), median (i.q.r.) | 5 (2–8) | 1 (1–3) | < 0.001† |
|
| 223 (38.5%) | 244 (32.0%) | 0.009 |
| Missing | 19 (3.3%) | 18 (2.4%) | |
| Total length of stay (ICU + ward) (days), median (i.q.r.) | 22 (14–35) | 11 (7–17) | < 0.001† |
|
| |||
| 30 days | 91 (15.7%) | 96 (12.6%) | 0.104 |
| 1 year | 161 (27.8%) | 164 (21.5%) | 0.008 |
| 3 years | 240 (41.4%) | 297 (39.0%) | 0.363 |
| ICU | Controls |
| |
|---|---|---|---|
|
| 15 (8–25) | 6 (4–9) | < 0.001† |
| Missing | 16 (1.1%) | 152 (0.7%) | |
|
| 140 (10.4%) | 4638 (20.6%) | < 0.001 |
| Missing | 481 (35.8%) | 7384 (32.8%) | |
|
| |||
| 30 days | 187 (13.9%) | 131 (0.6%) | < 0.001 |
| 1 year | 325 (24.2%) | 1040 (4.6%) | < 0.001 |
| 3 years | 537 (40.0%) | 3443 (15.3%) | < 0.001 |
| Odds ratio | ||
|---|---|---|
| Univariable analysis | Multivariable analysis | |
| Age (per year) | 1.07 (1.07, 1.07) | 1.06 (1.05, 1.06) |
| Male sex | 1.13 (1.05, 1.21) | 1.19 (1.10, 1.29) |
|
| ||
| I | 1.00 (reference) | 1.00 (reference) |
| II | 1.94 (1.65, 2.27) | 1.23 (1.04, 1.46) |
| III | 4.74 (4.05, 5.54) | 2.33 (1.95, 2.77) |
| IV | 11.69 (9.36, 14.59) | 4.57 (3.57, 5.85) |
| Body mass index > 30 kg/m2 | 0.98 (0.89, 1.06) | 0.94 (0.85, 1.04) |
| Perioperative blood loss > 500 ml | 1.61 (1.47, 1.76) | 1.34 (1.20, 1.50) |
| Laparoscopic surgery | 0.63 (0.58, 0.68) | 0.79 (0.72, 0.86) |
| Perioperative perforation | 1.73 (1.33, 2.25) | 1.24 (0.92, 1.69) |
| Duration of operation (per minute) | 1.00 (0.99, 1.00) | 1.00 (0.99, 1.00) |
| Cardiovascular complication | 3.95 (3.40, 4.58) | 1.98 (1.66, 2.36) |
| Infectious complication | 2.37 (2.10, 2.67) | 1.48 (1.28, 1.71) |
| Neurological complication | 3.42 (2.26, 5.17) | 1.68 (1.045, 2.69) |
| Surgical complication | 1.59 (1.46, 1.75) | 1.17 (1.021, 1.34) |
| Other complication | 1.62 (1.43, 1.83) | 1.07 (0.93, 1.24) |
| Surgical reintervention | 1.92 (1.72, 2.15) | 1.1 (0.98, 1.39) |
| Tumour stage | 1.73 (1.66, 1.80) | 1.86 (1.77, 1.95) |
| Unplanned ICU admission | 3.70 (3.30, 4.15) | 2.06 (1.78, 2.38) |
| ICU | Controls | |
|---|---|---|
|
| 1022 (76.2%) | 4864 (21.6%) |
| Missing | 10 (0.8%) | 74 (0.3%) |
|
| ||
| Infection | 328 (24.4%) | 1042 (4.6%) |
| 30-day mortality | 73 (22.3%) | 24 (2.3%) |
| Cardiovascular | 261 (19.5%) | 478 (2.1%) |
| 30-day mortality | 75 (28.7%) | 53 (11.1%) |
| Neurological | 20 (1.5%) | 74 (0.3%) |
| 30-day mortality | 4 (20.0%) | 6 (8.1%) |
| Surgical | 582 (43.4%) | 2550 (11.3%) |
| 30-day mortality | 84 (14.4%) | 32 (1.3%) |
| Other | 299 (22.3%) | 1265 (5.6%) |
| 30-day mortality | 48 (16.1%) | 16 (1.3%) |
|
| 578 (43.1%) | 1261 (5.6%) |
| 30-day mortality | 91 (6.8%) | 22 (0.1%) |
|
| ||
| Anastomotic leak | 297 (22.1%) | 469 (2.1%) |
| 30-day mortality | 43 (14.5%) | 9 (1.9%) |
| Infection | 52 (3.9%) | 99 (0.4%) |
| 30-day mortality | 14 (26.9%) | 3 (3.0%) |
| Wound dehiscence | 115 (8.6%) | 405 (1.8%) |
| 30-day mortality | 21 (18.3%) | 4 (1.0%) |
| Other | 168 (12.5%) | 340 (1.5%) |
| 30-day mortality | 31 (18.5%) | 8 (2.4%) |
| Interval between primary surgery and reintervention (days), median (i.q.r.) | 6 (3–8) | 7 (4–10) |
- —Stig and Ragna Gorthon Foundation
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSepsis Diagnosis and Treatment · Cardiac, Anesthesia and Surgical Outcomes · Enhanced Recovery After Surgery
Introduction
Surgical resection is the core of curative management for colon cancer. Morbidity and mortality rates following elective colon cancer resection have declined owing to advances in surgical technique, preoperative optimization, patient selection, and improved postoperative care^1,2^. However, a significant percentage of patients still develop complications that affect both short- and long-term survival, irrespective of tumour stage^3^. In-hospital mortality rates of 2–5% have been reported after elective colon resection^4^ and many postoperative deaths have been preceded by admission to the intensive care unit (ICU).
Postoperative intensive care unit (ICU) admission is sometimes planned before operation, or occurs as a result of patient deterioration while in a lower-acuity setting. Unselected ICU admission after elective colon resection is generally not recommended^5,6^. However, in certain patients, such as elderly and frail people, planned overnight ICU admission may decrease the risk of postoperative adverse events, attributed to closer monitoring and earlier intervention than in a regular surgical ward^7^. Studies^8,9^ investigating the aetiology of postoperative ICU admission and its association with patient outcome after elective colon cancer resection are scarce. Commonly, ICU admission is considered a binary measure, and no distinction is made according to the precipitating cause of ICU admission. Hence, the impact of unplanned postoperative intensive care after elective colon cancer resection remains largely unknown.
The primary aim of this study was to evaluate the incidence of, and factors associated with, unplanned ICU admission following elective colon cancer surgery. The secondary aim was to analyse short- and long-term survival.
Methods
Study design
This was a retrospective, observational multicentre study based on registry data from the Swedish Colorectal Cancer Registry (SCRCR) and the Swedish Intensive Care Registry (SIR). This study was designed and conducted in accordance with the STROBE guidelines^10^. Ethical approval was obtained from the Swedish Ethical Review Authority (2021-02448).
Registries
The SCRCR comprises data on consenting patients diagnosed with colon cancer since 2007 and rectal cancer since 1995 (https://scrcr.se/). The registries cover 98–99% of all colorectal cancers in Sweden, compared with compulsory registration in the National Cancer Registry. The SCRCR is linked to the Swedish population registry, from which survival data are retrieved. The SIR was launched in 2001 and is a national quality registry of patients admitted to ICU. It has complete coverage of Swedish ICUs (https://www.icuregswe.org). Available data in the SIR include baseline demographics, variables included in the Simplified Acute Physiology Score (SAPS3), and variables relating to treatment given in the ICU.
Inclusion process
Patients undergoing elective colon cancer resection between January 2010 and December 2019 were identified from the SCRCR and included in the study. Included patients were matched with the SIR to identify postoperative ICU admissions. Exclusion criteria were non-surgical management of the primary tumour, palliative surgical intent, synchronous metastases (M1) at diagnosis, tumour location in the rectum or appendix, and planned ICU admission. Planned ICU admissions are defined by the SIR as admissions that are known by the ICU for ≥ 12 h. In this study, admissions were considered to have been planned before operation if they were registered as a planned admission and occurred on the day of surgery.
Study protocol
The postoperative period was defined as a 2-week interval from the day of surgery throughout the second postoperative week. Patients requiring postoperative ICU admission constituted the ICU group, and those who received treatment in a regular surgical ward only served as the control group. The ICU group was further stratified into admissions depending on whether surgical reintervention was needed or not. Surgical reintervention is defined by the SCRCR as any unplanned postoperative laparotomy, surgical procedures in the operating room or in the ICU, or percutaneous radiological interventions, corresponding to Clavien–Dindo grade IIIa–b. The rationale for this distinction is that complications requiring surgical intervention are usually more serious than those handled without surgical intervention, and usually make the patient more ill, and more likely to require intensive care.
Data analysed
The following SCRCR data were extracted: age, sex, American Society of Anesthesiologists (ASA) fitness grade, surgical approach (open versus minimally invasive), anatomical resection, perioperative blood loss, intraoperative bowel perforation, duration of operation, ostomy decision, complications, and complications requiring reintervention. The SCRCR classifies complications as cardiovascular, infectious, neurological, surgical or other.
Details regarding the ICU admission were retrieved from the SIR, comprising length of ICU stay, reasons for ICU admission, whether the admission was planned or unplanned, non-invasive ventilation, invasive ventilation, continuous renal replacement therapy (CRRT), vasoactive support, SAPS3, and estimated mortality risk (EMR). Possible reasons for admission are cardiovascular, gastrointestinal, respiratory, renal, neurological, other, and observation.
SAPS3 is a risk stratification score used to predict death in patients admitted to the ICU. It is based on three areas: patient co-morbidities, such as chronic conditions and diseases; data regarding the ICU admission, such as reason for admission and surgical status; and the patient’s physiological derangement within 1 hour before to 1 hour after ICU admission^11^.
Statistical analysis
Data with a normal distribution are presented as mean(standard deviation) whereas skewed continuous and ordinal data are presented as median (interquartile range). Categorical data are presented as numbers with percentages. Student’s t test was used for hypothesis testing of normally distributed data, Wilcoxon rank-sum test for skewed and ordinal data, and χ^2^ test for categorical variables. Normality was assessed using the Kolmogorov–Smirnov test.
Univariable and multivariable logistic regression analyses were used to identify factors associated with unplanned ICU admission and death. The regression variables were selected based on clinical judgement and results from previous studies^9,12^. Survival was estimated using the Kaplan–Meier method, and the log rank test was used to assess differences between groups.
The significance level was set to 0.05. Data were processed using Stata^®^ BE version 18 (StataCorp, College Station, TX, USA).
Results
Study population characteristics
In total, 70 758 patient records were extracted from the SCRCR, of which 23 891 fulfilled the inclusion criteria and were included in the study. A total of 1343 patients (5.6%) had unplanned postoperative ICU admissions and constituted the ICU group. The remaining 22 548 patients not admitted to ICU comprised the control group (Fig. 1).
Study flow chartSCRCR, Swedish Colorectal Cancer Registry; ICU, intensive care unit.
Patient and perioperative characteristics
Clinical and demographic characteristics of the ICU group and controls are summarized in Table 1. Patients requiring intensive care were predominantly men (58 versus 48.5%) and were older (77 versus 74 years) with higher ASA grades than controls. Among 569 patients with an ASA grade of IV, 17% had unplanned postoperative ICU admissions. Tumour stage and the range of operations were broadly similar, although the ICU group was less likely to be operated with a minimally invasive technique (12.1 versus 24.1%), and a larger proportion received permanent ostomies. Differences in operating time and blood loss were moderate.
ICU admission
Reasons for ICU admission are shown in Figs 2 and 3. The reasons for admission were multifactorial and the majority of patients had multiple organ systems affected.
Reasons for unplanned postoperative ICU admission in surgical reintervention groupICU, intensive care unit.
Reasons for unplanned postoperative ICU admission in group with no surgical reinterventionICU, intensive care unit.
Patients in the surgical reintervention group were younger and had lower ASA grades (Table 2). They were admitted later in relation to their primary surgery, and needed more invasive ventilation and CRRT compared with non-surgical admissions. Patients in the surgical reintervention group had a higher SAPS3 score and EMR at admission. Both ICU and hospital stay were longer for patients in the surgical reintervention group compared with the group without surgical reintervention (Table 2).
Factors associated with unplanned postoperative ICU admission
In multivariable logistic regression analysis, factors associated with unplanned ICU admission included surgical reintervention (odds ratio (OR) 8.07, 95% confidence interval (c.i.) 6.58 to 9.89), cardiovascular complications (OR 6.60, 5.39 to 8.08), ASA grade IV (OR 4.74, 3.14 to 7.16), and infectious complications (OR 3.51, 2.95 to 4.18). Laparoscopic surgery was associated with a lower rate of ICU admission (OR 0.59, 0.50 to 0.69) (Table S1).
Survival analysis
Unplanned ICU admission was associated with poorer short- and long-term survival compared with those in controls. The 30-day mortality rate was 13.9% (187 deaths) for the ICU group compared with 0.6% (131) for controls (P < 0.001). This trend was consistent over time, with unadjusted 1-year mortality rates of 24.2 versus 4.6%, and 3-year mortality rates of 40.0 versus 15.3%, respectively (P < 0.001) (Table 3). In multivariable analysis, unplanned ICU admission and cardiovascular complications were among the factors associated with 30-day mortality (Table S2). These variables were also associated with 3-year mortality, although ASA grade IV had the strongest association (Table 4).
No statistically significant difference was noted in 30-day mortality depending on the need for surgical reintervention (15.7 versus 12.3%; P = 0.104). However, the 1-year mortality rate was higher in the surgical reintervention group (27.8 versus 21.5%; P = 0.008) whereas 3-year mortality rates were similar in the two groups (41.4 versus 39.0%; P = 0.363) (Table 2). A Kaplan–Meier curve detailing 3-year mortality is shown in Fig. 4.
Three-year survival following elective surgery for patients with stage I–III colon cancer, stratified by need for postoperative ICU carePatients with < 30 days’ survival or follow-up were excluded from the analysis. ICU, intensive care unit.
Complications
Complications were more common in the ICU group, irrespective of complication type, and subsequently the hospital stay was longer (15 versus 6 days). In the ICU group, 76.2% had a specified complication registered in the SCRCR compared with 21.6% in the control group. The proportion of surgical complications in need of reintervention was higher in the ICU group than in the control group. Surgical complications were the most common type of complication and anastomotic leakage the most common single cause for surgical reintervention (Table 5).
The pattern of complications registered in the SCRCR differed somewhat depending on whether any surgical reintervention was required or not. The surgical reintervention group had a higher proportion of complications related to the surgery itself (86 versus 11%). Conversely, the rate of cardiovascular complications was higher in the group with no surgical reintervention (23 versus 14%). Similar distributions were observed for neurological, infectious, and other complications.
Discussion
This registry-based study analysed the incidence, aetiology, and outcome in patients who had an unplanned ICU admission following elective colon cancer resection. The most important findings were that unplanned ICU admission was associated with increased short- and long-term mortality compared with rates in controls, and that patients admitted to ICU owing to surgical complications requiring reintervention were diagnosed later in the postoperative course than those who did not need surgical intervention, and required longer ICU and in-hospital stays. Although those requiring surgical reintervention were younger and had less co-morbidity, they had similar or higher short- and long-term mortality rates compared with those who did not have surgical reintervention.
The proportion of unplanned ICU admissions was 5.6%, with an associated 30-day mortality rate of 13.9%. This is in line with the wide range in previous studies^8,12–16^, which reported postoperative ICU admission rates ranging from 3 to 25% with in-hospital mortality rates of 11–28% depending on patient selection. Common risk factors include pre-existing cardiopulmonary disease, ASA grade III or higher, male sex, and older age, and were confirmed in the present study. In contrast to the present work, most previous studies did not discern between planned and unplanned ICU admissions, observation-only versus invasive measures, or the precipitating cause of critical illness.
Some studies have suggested that intraoperative microcirculation may be predictive of postoperative complications such as myocardial infarction^17^, renal failure^18^, and anastomotic leaks^19,20^. It is plausible that suboptimal haemodynamics in the early postoperative period might increase the risk of complications that become clinically evident days later. Another important factor is perioperative fluid management, and promoting a normovolaemic state to reduce the risk of cardiopulmonary complications, postoperative ileus, and oedema-related anastomotic complications^21^. Postoperative observation in a high-dependency unit or ICU could mitigate this by closer monitoring, earlier intervention, and a wider range of therapeutic options to optimize fluid homeostasis and end-organ perfusion. This strategy is supported by previous studies^7,22^ suggesting that planned ICU admission after colorectal cancer surgery might be beneficial in at-risk populations.
It is hypothetical whether any of the unplanned ICU admissions in this study could have been avoided by a higher level of care immediately after surgery and, as resources are finite, the challenge of patient selection remains.
Patients requiring surgical reintervention had similar or higher mortality rates than those admitted to ICU for other reasons, despite being younger and healthier, measured by ASA grade. These patients were admitted to the ICU later in the postoperative period and were in worse condition as measured by SAPS3 on arrival in the ICU, and required invasive ventilation, vasopressors, and renal replacement therapy more frequently.
Previous data support different temporal distributions between surgical and non-surgical postoperative complications. It has been noted that non-surgical complications tend to occur and be treated on postoperative days 1–3^23,24^, whereas surgical complications are diagnosed after a median of 7 days^25^. The question arises whether this is the natural course or whether there is a delay in the diagnosis and treatment of surgical complications, as these patients seemed to be worse off upon ICU arrival and had substantially longer recovery times. This finding further stresses the need for improving routines to discover complications at an early stage, and considerable efforts have been made to find sensitive predictors^26–32^. Reoperation within 2 days of suspicion of complication has been shown to decrease the need for intensive care, shorten hospital stay, and also to be associated with a higher chance of laparoscopic reintervention and fewer postoperative computed tomograms^33^. Unfortunately, none of the registries in this study hold data enabling analysis of whether the surgical complications were simply more severe or whether there was an element of failure to rescue involved. However, the excessive increase in mortality demonstrated in this study warrants further research to better understand what could be attributed to the postoperative level of care, and to what extent surgeon-, patient-, and tumour-related factors affect patient outcome.
It is worth noting that the ICU group received adjuvant treatment less frequently than controls, which naturally would affect their long-term outcome; however, this information was missing in about one-third of patients, thus limiting the interpretation of this variable. Several studies^34,35^ have shown that postoperative complications negatively affect both long-term survival and disease-free survival in patients with colon cancer. Comparisons between studies are hampered by methodological heterogeneity, but proposed mechanisms include increased risk of cancer recurrence, the influence of underlying co-morbidities, and immunological alterations triggered by severe illness. Overall, these findings highlight the substantial survival benefits associated with preventing serious postoperative complications.
Laparoscopic surgery was associated with fewer unplanned ICU admissions and a lower 3-year mortality rate even after adjusting for key confounders. However, this finding must be interpreted cautiously as the results likely reflect a strong selection bias, as patients selected for laparoscopy may have had less complex disease and lower perioperative risk. Despite adjustment for factors such as ASA grade and tumour stage, residual confounding cannot be excluded. Nevertheless, the data align with previous studies suggesting that laparoscopy may reduce severe postoperative complications by limiting surgical trauma^36–38^, which in turn could contribute to improved long-term survival^39^.
Taken together, the results point to the need for identifying improved routines to detect and treat complications early on and, not least, implement measures that decrease the risk of complications, such as minimally invasive approaches, goal-oriented fluid regimens, and maybe also planned ICU care in selected patients.
The major strength of this study is the combination of two nationwide registries allowing surgically oriented data to be analysed together with comprehensive records from the ICU. This enables a more detailed account of the true incidence, aetiology, and outcome in patients admitted to the ICU following elective colon resection. In contrast to most previously published data, this study provides information on whether the ICU admission was planned or unplanned, what kind of invasive measures were needed, and an indication of the physiological state of the patient on arrival in the ICU. Furthermore, it is population-based, relatively large, and has longer follow-up than comparable studies.
This study has several limitations. Although data were registered prospectively, the retrospective study design carries inherent risks of missing or misclassified information. The multicentre setting, although a strength, may also have introduced heterogeneity, as ICU admission criteria may vary between hospitals. Some centres may also use high-dependency or enhanced observation units that are not captured in the registries, potentially biasing the results. Data on adjuvant treatment were largely missing, limiting conclusions regarding its impact on long-term survival. Preoperative status was assessed only by age and ASA grade, the latter being a subjective measure, although it has been validated as a predictor of surgical morbidity and mortality in several studies^40^. No nutritional markers (for example albumin, prealbumin) or detailed co-morbidity data (such as diabetes, chronic obstructive pulmonary disease, cardiovascular disease) were available. Finally, unlike some comparable registries, the SCRCR does not record respiratory complications, despite these being a frequent cause of postoperative deterioration and ICU admission in both this and other cohorts.
Supplementary Material
zraf178_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Iversen LH, Ingeholm P, Gögenur I, Laurberg S. Major reduction in 30-day mortality after elective colorectal cancer surgery: a nationwide population-based study in Denmark 2001–2011. Ann Surg Oncol 2014;21:2267–227324585408 10.1245/s 10434-014-3596-7 · doi ↗ · pubmed ↗
- 2Brenner H, Bouvier AM, Foschi R, Hackl M, Larsen IK, Lemmens V et al Progress in colorectal cancer survival in Europe from the late 1980 s to the early 21st century: the EUROCARE study. Int J Cancer 2012;131:1649–165821607946 10.1002/ijc.26192 · doi ↗ · pubmed ↗
- 3Odermatt M, Miskovic D, Flashman K, Khan J, Senapati A, O’Leary D et al Major postoperative complications following elective resection for colorectal cancer decrease long-term survival but not the time to recurrence. Colorectal Dis 2015;17:141–14925156234 10.1111/codi.12757 · doi ↗ · pubmed ↗
- 4Drolet S, Mac Lean AR, Myers RP, Shaheen AA, Dixon E, Buie WD. Elective resection of colon cancer by high-volume surgeons is associated with decreased morbidity and mortality. J Gastrointest Surg 2011;15:541–55021279550 10.1007/s 11605-011-1433-x · doi ↗ · pubmed ↗
- 5Kahan BC, Koulenti D, Arvaniti K, Beavis V, Campbell D, Chan M et al Critical care admission following elective surgery was not associated with survival benefit: prospective analysis of data from 27 countries. Intensive Care Med 2017;43:971–97928439646 10.1007/s 00134-016-4633-8 · doi ↗ · pubmed ↗
- 6Vourc’h M, Asehnoune K. Postoperative admission in surgical ICU, less is more? Anaesth Crit Care Pain Med 2019;38:217–21930951884 10.1016/j.accpm.2019.03.006 · doi ↗ · pubmed ↗
- 7Fahim M, Visser RA, Dijksman LM, Biesma DH, Noordzij PG, Smits AB. Routine postoperative intensive care unit admission after colorectal cancer surgery for the elderly patient reduces postoperative morbidity and mortality. Colorectal Dis 2020;22:408–41531696590 10.1111/codi.14902 · doi ↗ · pubmed ↗
- 8Dale CD, Mc Loone P, Sloan B, Kinsella J, Morrison D, Puxty K et al Critical care provision after colorectal cancer surgery. BMC Anesthesiol 2016;16:9427733119 10.1186/s 12871-016-0243-9PMC 5059906 · doi ↗ · pubmed ↗