Multimodality imaging of the right ventricular outflow tract haemangioma requiring pulmonary valve replacement
Rui Katano, Satonori Tsuneta, Satoru Wakasa, Atsushi Tada

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
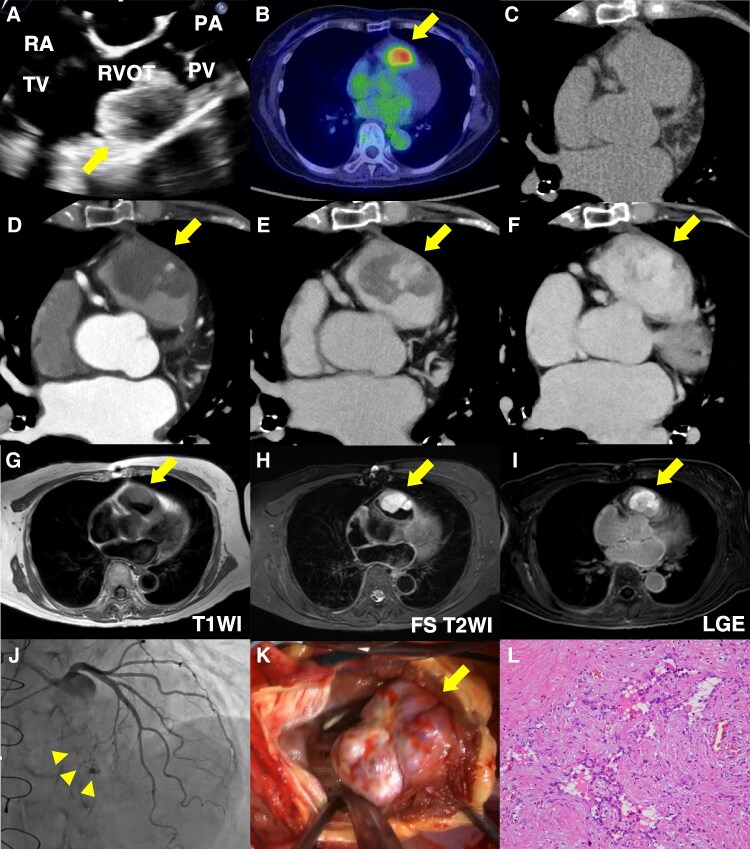 Figure 1
Figure 1- —Hokkaido Heart Association Grant for Research
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac tumors and thrombi · Congenital Heart Disease Studies · Vascular Anomalies and Treatments
Case description
A 76-year-old woman was referred for evaluation of a suspected right ventricular tumour identified on computed tomography (CT). She was asymptomatic, and tumour markers were negative. Transoesophageal echocardiography showed a broad-based, 3-cm mass in the right ventricular outflow tract (RVOT), located immediately beneath the pulmonary valve, without RVOT obstruction (Figure 1A; Supplementary material online, Video S1). ^18^F-FDG PET demonstrated localized uptake (SUVmax 3.73; Figure 1B). Non-contrast CT showed slightly low attenuation (38 Hounsfield units) (Figure 1C), and contrast-enhanced CT demonstrated nodular peripheral enhancement in the arterial phase, followed by progressive centripetal fill-in in the later phases (Figure 1D–F) and no evidence of pulmonary embolism. Cardiac MRI demonstrated low T1 signal (Figure 1G) and high fat-suppressed T2 signal (Figure 1H), with uniform delayed enhancement (Figure 1I), which, in the absence of predisposing factors, helped exclude thrombus. Coronary angiography identified feeding vessels arising from a septal branch (Figure 1J; Supplementary material online, Video S2). Pre-operative catheter-based biopsy was not performed due to risks of tumour-related bleeding or systemic embolization.
Multimodality imaging characterizes a right ventricular outflow tract tumour and suggests a benign aetiology pre-operatively (A–J). Transoesophageal echocardiography (A), 18F-FDG PET (B), computed tomography: non-contrast computed tomography (C), arterial phase (D), equilibrium phase (E), and delayed phase (F) of contrast-enhanced computed tomography, cardiac MRI: T1-weighted image (G), fat-suppressed T2-weighted image (H), late gadolinium enhancement (I), and coronary angiography (J) demonstrate a broad-based mass arising from the right ventricular outflow tract. Non-contrast computed tomography showed slightly low attenuation (38 HU), which was lower than that of the blood pool (46 HU) (C). Intra-operative photograph shows the mass adjacent to the pulmonary valve anterior leaflet annulus (K). Post-operative histopathology reveals proliferation of vascular channels, forming cavernous, slit-like, and papillary spaces, without significant cytologic or architectural atypia (L). RVOT, right ventricular outflow tract; HU, Hounsfield units; PV, pulmonary valve; TV, tricuspid valve; PA, pulmonary artery; RA, right atrium; T1WI, T1-weighted image; FS-T2WI, fat-suppressed T2-weighted image; LGE, late gadolinium enhancement.
Given the working diagnosis of a primary cardiac tumour, surgical resection was performed (Figure 1K). Owing to its proximity to the pulmonary valve annulus, en bloc excision with bioprosthetic valve replacement and RVOT reconstruction was necessary to avoid incomplete resection or significant regurgitation. Post-operative histopathology revealed proliferation of vascular channels, forming cavernous, slit-like, and papillary spaces, without significant cytologic or architectural atypia (Figure 1L). Immunostaining was positive for CD31, CD34, and ERG, but negative for AE1/AE3, EMA, and D2-40. With low Ki-67 labelling index (approximately 2%) and wild-type p53 pattern, these findings confirmed the diagnosis of haemangioma.
Pre-operative distinction between benign and malignant cardiac tumours remains challenging, particularly for right-sided masses. This case demonstrates that multimodality imaging, integrating morphological features, enhancement patterns, metabolic activity, and malignancy prediction scores,^1^ can support a benign diagnosis and inform surgical planning.
Supplementary Material
ytag123_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.