Reperfusion Pulmonary Hemorrhage Following Mechanical Thrombectomy for Sub-massive Pulmonary Embolism
John Bajouka, Ghaid Touza, Keyur Patel, Ziad Affas, Stephen Lynch

TL;DR
A patient developed reperfusion pulmonary hemorrhage after mechanical thrombectomy for a sub-massive pulmonary embolism, highlighting the need to recognize this rare complication.
Contribution
This case report identifies reperfusion pulmonary hemorrhage as a distinct post-thrombectomy complication that mimics other conditions.
Findings
The patient showed acute hypoxia and radiographic consolidation after successful thrombectomy.
Reperfusion pulmonary hemorrhage was diagnosed based on angiographic findings and clinical context.
Supportive care led to clinical stabilization and recovery.
Abstract
Mechanical thrombectomy is an increasingly utilized intervention for patients with intermediate-risk pulmonary embolism who demonstrate right ventricular strain. While effective at reducing clot burden and improving hemodynamic parameters, the procedure carries a risk of rare post-interventional complications. This case report describes a 75-year-old woman with a history of breast carcinoma who presented with progressive dyspnea and right lower extremity swelling following recent air travel. Diagnostic imaging revealed a sub-massive right-sided pulmonary artery occlusion and severe right ventricular dilatation with reduced systolic function. The patient underwent successful mechanical thrombectomy, resulting in the removal of large, organized thrombi and immediate improvement in pulmonary blood flow. However, the patient developed acute hypoxia shortly after the procedure. Subsequent…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
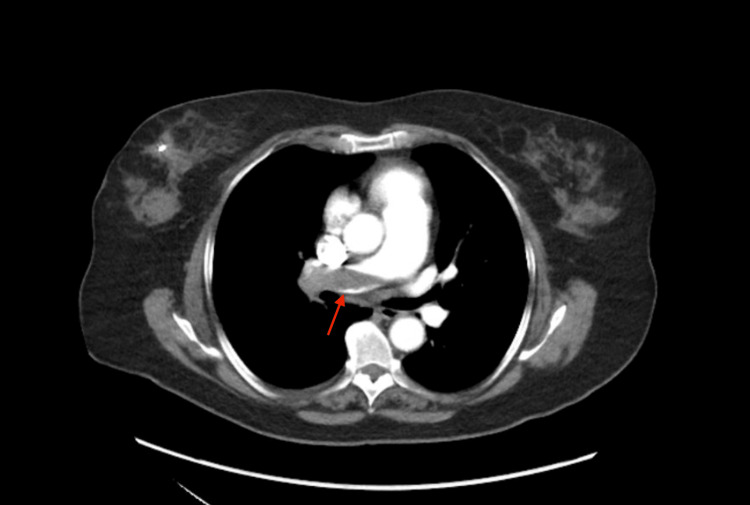 Figure 1
Figure 1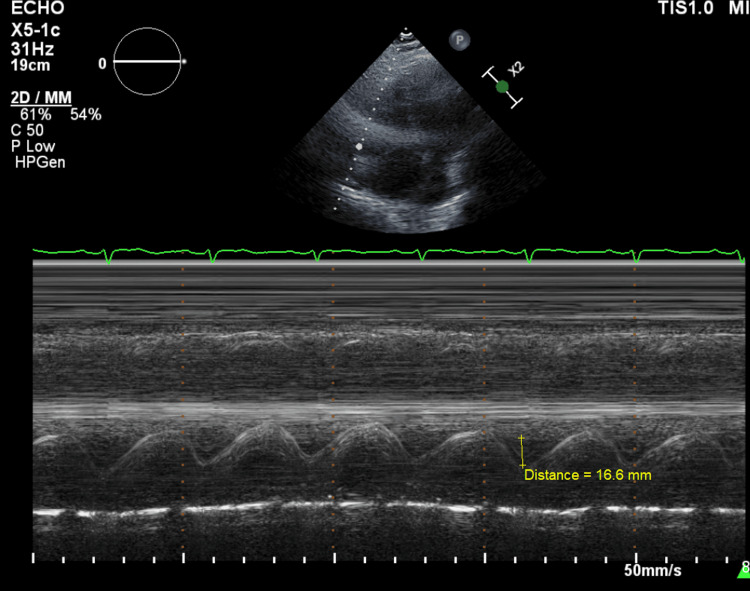 Figure 2
Figure 2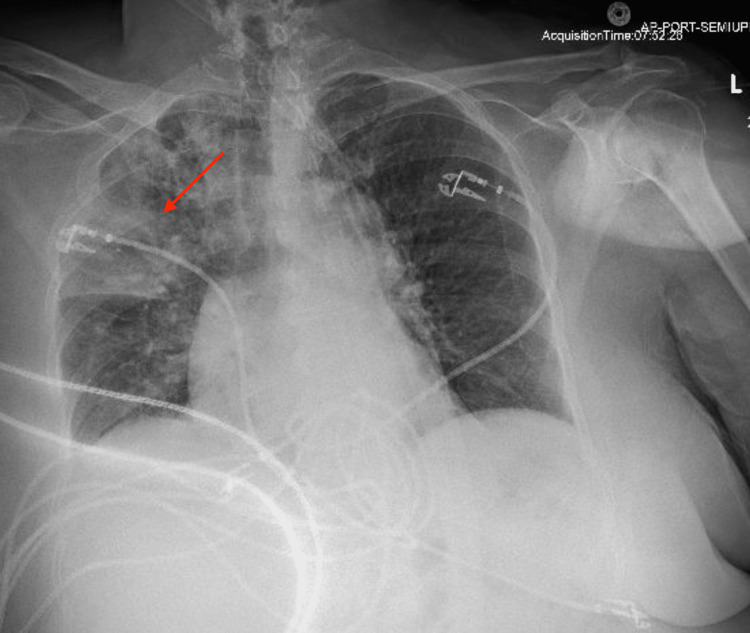 Figure 3
Figure 3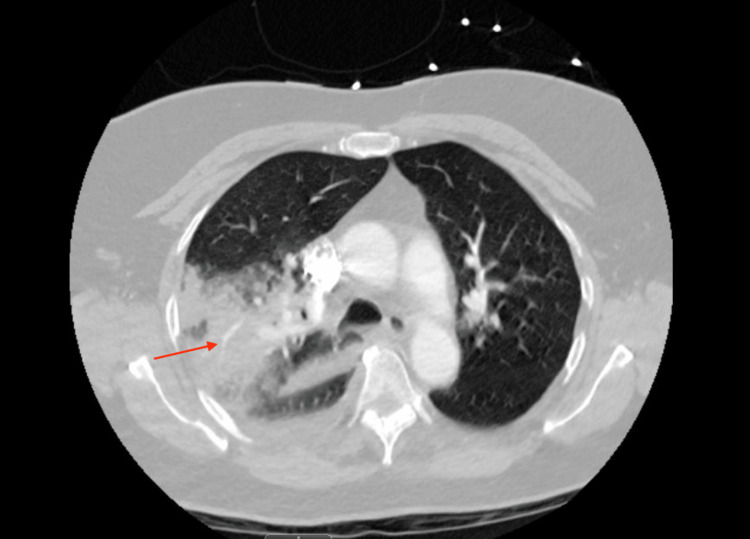 Figure 4
Figure 4| Assessment | Results | Reference Ranges |
| Blood Pressure | 146/83 mmHg | <120/80 mmHg |
| Heart Rate | 96 bpm | 60–100 bpm |
| Oxygen Requirement | 2 Liters per Minute per Nasal Cannula | Room Air (0 L/min) |
| Arterial Blood Gas | ||
| pH | 7.51 | 7.35–7.45 |
| Partial Pressure of Oxygen (PO2) | 75 mmHg | 75–100 mmHg |
| Bicarbonate (HCO3) | 26.3 mEq/L | 22–26 mEq/L |
| Cardiac Biomarkers | ||
| High-Sensitivity Troponin (Initial) | 21 ng/L | 0–14 ng/L |
| High-Sensitivity Troponin (Repeat) | 19 ng/L | 0–14 ng/L |
| Pro-B-Type Natriuretic Peptide | 1163 pg/mL | <125 pg/mL |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVenous Thromboembolism Diagnosis and Management · Mechanical Circulatory Support Devices · Vascular Anomalies and Treatments
Introduction
Pulmonary embolism (PE) remains a significant cause of cardiovascular morbidity and mortality, particularly in older adults. While anticoagulation is the standard of care for low-risk cases, mechanical thrombectomy (MT) has emerged as a vital interventional option for patients with submassive PE who exhibit signs of right ventricular (RV) strain or clinical deterioration. The prevalence of submassive PE is notable for its potential to progress rapidly to hemodynamic collapse, necessitating treatments that can quickly alleviate RV pressure overload [1]. Despite its efficacy, the widespread adoption of MT still faces the risk of rare but serious periprocedural complications. Known post-intervention complications include vascular injury, arrhythmia, and hemothorax. One of the most diagnostically challenging complications is reperfusion pulmonary hemorrhage, a phenomenon that can be radiographically indistinguishable from procedural bleeding. Identifying this condition early is essential to avoid unnecessary interventions, such as reversal of life-saving anticoagulation. This case report describes a classic presentation of reperfusion injury following mechanical thrombectomy for a large right-sided PE. Emphasizing this case is critical for clinicians to better recognize and manage the unique radiographic and clinical signature of abrupt flow restoration.
Case presentation
A 75-year-old woman with a history of stage 2 right breast carcinoma, hypertension, and recent air travel to Texas presented with progressive exertional dyspnea over one week, worsening over the preceding days. She reported right lower extremity swelling extending from the foot to the groin one week prior, which resolved spontaneously. She denied prior venous thromboembolism, congestive heart failure, or family history of thrombosis. Additional symptoms included nonproductive cough, congestion, and right lower rib discomfort. She denied fevers, chills, chest pain, hemoptysis, nausea, vomiting, diarrhea, abdominal pain, dysuria, or calf tenderness. Initially, the patient was hypoxic but hemodynamically stable, requiring two liters of nasal cannula. High-sensitivity troponin resulted at 21 with a repeat of 19; pro-BNP was 1163 pg/mL (Table 1).
The admitting electrocardiogram showed normal sinus rhythm with no signs of right ventricular strain. Computed tomography (CT) angiography to assess for PE showed total occlusion of the right pulmonary artery (Figure 1). Echocardiography demonstrated a dilated RV with reduced systolic function (Figure 2). Given the large clot burden and impaired RV function, the patient was started on a heparin infusion and taken for mechanical thrombectomy. The right anterior basal pulmonary artery, right middle lobar pulmonary artery, and the right main pulmonary artery were evacuated of thrombus with angiographic improvement in flow.
Initial CT Angiography Demonstrating Pulmonary EmbolismA large pulmonary embolus in the right pulmonary artery is seen.
M-Mode Echocardiography from an Apical Four-Chamber View Measurement of tricuspid annular plane systolic excursion (TAPSE) demonstrating a value of 16.6mm indicating right ventricular dysfunction.
Shortly following the mechanical thrombectomy, the patient’s respiratory status declined. Despite being maintained on five liters via nasal cannula, she became increasingly hypoxic, with her oxygen saturation dropping to 89%. This rapid desaturation necessitated an urgent escalation of respiratory support. The patient was transitioned to a high-flow nasal cannula, eventually requiring a flow rate of 35 liters per minute to maintain adequate oxygenation. A chest X-ray was obtained, which showed opacification of the right upper lobe, which was concerning for pulmonary hemorrhage (Figure 3). A repeat CT angiography of the chest demonstrated an extensive right upper lobe consolidation, patchy densities in the middle and lower lobes, small reactive pleural effusion with no contrast extravasation to suggest vascular injury (Figure 4). Due to intact vasculature, the patient was diagnosed with reperfusion injury.
Post-thrombectomy Chest X-rayA large right upper lobe consolidation is demonstrated.
Repeat CT Angiography Post-thrombectomy Interval evacuation of right main and lobar pulmonary arterial emboli. Extensive consolidation within the right upper lobe with restored contrast opacification demonstrating patent blood flow.
The patient remained clinically stable. Her hypoxia improved with no evidence of hemoptysis. No further complications were observed. She was monitored, transitioned to oral apixaban, and safely discharged home.
Discussion
This case illustrates a classic presentation of reperfusion injury following mechanical thrombectomy for an extensive PE. The patient’s clinical course, marked by acute hypoxia and radiographic opacification immediately following successful clot evacuation, highlights a rare but significant complication of advanced PE interventions that clinicians must be prepared to manage.
The pathophysiology of reperfusion injury in the pulmonary vasculature is complex. The primary mechanism involves the sudden restoration of high-pressure flow to chronically hypoperfused lung parenchyma, leading to capillary rupture from abrupt pressure shifts. Furthermore, the rapid reintroduction of oxygenated blood triggers an inflammatory endothelial injury [2]. This process releases reactive oxygen species, including superoxide, hydrogen peroxide, and peroxynitrite, damaging cellular proteins, lipids, and DNA through oxidative stress, triggering lipid peroxidation and opening of the mitochondrial permeability transition pore and pro-inflammatory, increasing microvascular permeability and leading to fluid and red blood cells accumulation into the alveolar space [3].
A nuanced diagnostic challenge highlighted by this case is the interpretation of post-procedural imaging regarding the evacuation of the clot. While mechanical thrombectomy aims for complete debulking, it is common for residual mural thrombus to remain adherent to the vessel walls [4]. Interestingly, repeat angiography or CT may still show "filling defects" that do not represent a failure of the procedure, but rather the altered flow dynamics around residual fragments. Conversely, the restoration of blood flow to a previously occluded segment can sometimes be visualized as "hyperemia" or increased contrast enhancement in the distal parenchyma, which may be mistaken for active hemorrhage if not correlated with the patient's hemodynamic stability. Procedural trauma typically presents with immediate hemodynamic instability, brisk hemoptysis, and clear contrast extravasation on angiography [5]. In contrast, this patient remained hemodynamically stable, had no hemoptysis, and repeat CT angiography confirmed intact vasculature despite the new parenchymal opacities.
Risk factors identified in this patient included a large clot burden, a significant period of ischemia in the right lung, and the rapid nature of mechanical flow restoration. Current guidelines from the American Heart Association emphasize that patient selection for catheter-based interventions should balance the risk of PE-related mortality against procedural complications [6]. Management is primarily supportive, focused on supplemental oxygen and monitoring. While severe cases may necessitate airway protection or temporary anticoagulation reversal, this case reinforces that early recognition through imaging allows for the safe continuation of life-saving anticoagulation while the inflammatory response resolves. Inhaled nitric oxide or prostacyclin may improve ventilation-perfusion matching, and extracorporeal life support may be required when less aggressive interventions fail [7].
Conclusions
Mechanical thrombectomy remains an effective therapy for sub-massive PE. However, clinicians should recognize reperfusion pulmonary hemorrhage as a rare but potential complication, particularly in cases involving large clot burden and abrupt flow restoration. Early imaging, supportive care, and careful review of procedural angiography are essential for distinguishing reperfusion injury from procedural trauma.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Pulmonary embolism and right ventricular dysfunction: mechanism and management Cureus Ajah ON 016202410.7759/cureus.70561 PMC 1144330339355468 · doi ↗ · pubmed ↗
- 2Reperfusion injury and reactive oxygen species: the evolution of a concept Redox Biol Granger DN Kvietys PR 524551620152648480210.1016/j.redox.2015.08.020PMC 4625011 · doi ↗ · pubmed ↗
- 3Inflammatory response and pneumocyte apoptosis during lung ischemia-reperfusion injury in an experimental pulmonary thromboembolism model J Thromb Thrombolysis Deng C Zhai Z Wu D 42534020152567704310.1007/s 11239-015-1182-x PMC 4445764 · doi ↗ · pubmed ↗
- 4Residual pulmonary vascular obstruction following mechanical thrombectomy for submassive pulmonary embolism: a single-center analysis J Soc Cardiovasc Angiogr Interv Stegman B Kumar A Dahle T Schmidt W Dutcher J Glenz T Appelbaum D 101260320243913221610.1016/j.jscai.2023.101260 PMC 11307796 · doi ↗ · pubmed ↗
- 5Iatrogenic pulmonary artery rupture Curr Opin Anaesthesiol Bussières JS 48522020071721116710.1097/ACO.0b 013e 32801158 a 9 · doi ↗ · pubmed ↗
- 6Interventional therapies for acute pulmonary embolism: current status and principles for the development of novel evidence: a scientific statement from the American Heart Association Circulation Giri J Sista AK Weinberg I 0801140201910.1161/CIR.000000000000070731585051 · doi ↗ · pubmed ↗
- 7Innovation in catheter-directed therapy for intermediate-high-risk and high-risk pulmonary embolism JACC Cardiovasc Interv Zuin M Lang I Chopard R Sharp AS Byrne RA Rigatelli G Piazza G 225922731720243941538510.1016/j.jcin.2024.07.033 · doi ↗ · pubmed ↗