Risk-Stratified Use of Topical and Infiltrative Local Anesthetics in High-Risk Dermatologic Surgery
Seyedshayan Shojaei, Kimia Heidari, Alhasan Alobaidi, Devendra K Agrawal

TL;DR
This paper provides a risk-based framework for safely using local anesthetics in high-risk dermatologic surgeries, emphasizing updated safety practices and emergency preparedness.
Contribution
A novel, integrated risk-stratified framework for using local anesthetics in high-risk dermatologic contexts is proposed.
Findings
Epinephrine use in end-arterial sites is safe with dilute concentrations and adequate perfusion.
Topical anesthetics in barrier-compromised skin increase systemic toxicity risks, especially in vulnerable populations.
Dilute tumescent infiltration is safer than high-dose topical therapy for large denuded areas.
Abstract
Local anesthetics are fundamental to dermatologic practice, yet their safety profile requires nuanced understanding in high-risk contexts including end-arterial sites, barrier-compromised skin, and scenarios predisposing to systemic toxicity. This narrative review synthesizes contemporary evidence across these three interacting domains to provide an integrated, risk-stratified framework for clinical decision-making. Regarding end-arterial territories, over two decades of clinical evidence encompassing more than 200,000 digital and acral injections has effectively dismantled the historical dogma against epinephrine use in digits, nose, ear, and penis, demonstrating an excellent safety profile when dilute concentrations are used in patients with adequate perfusion, with phentolamine providing reliable rescue for rare, prolonged vasoconstriction. In barrier-compromised skin (e.g. burns,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
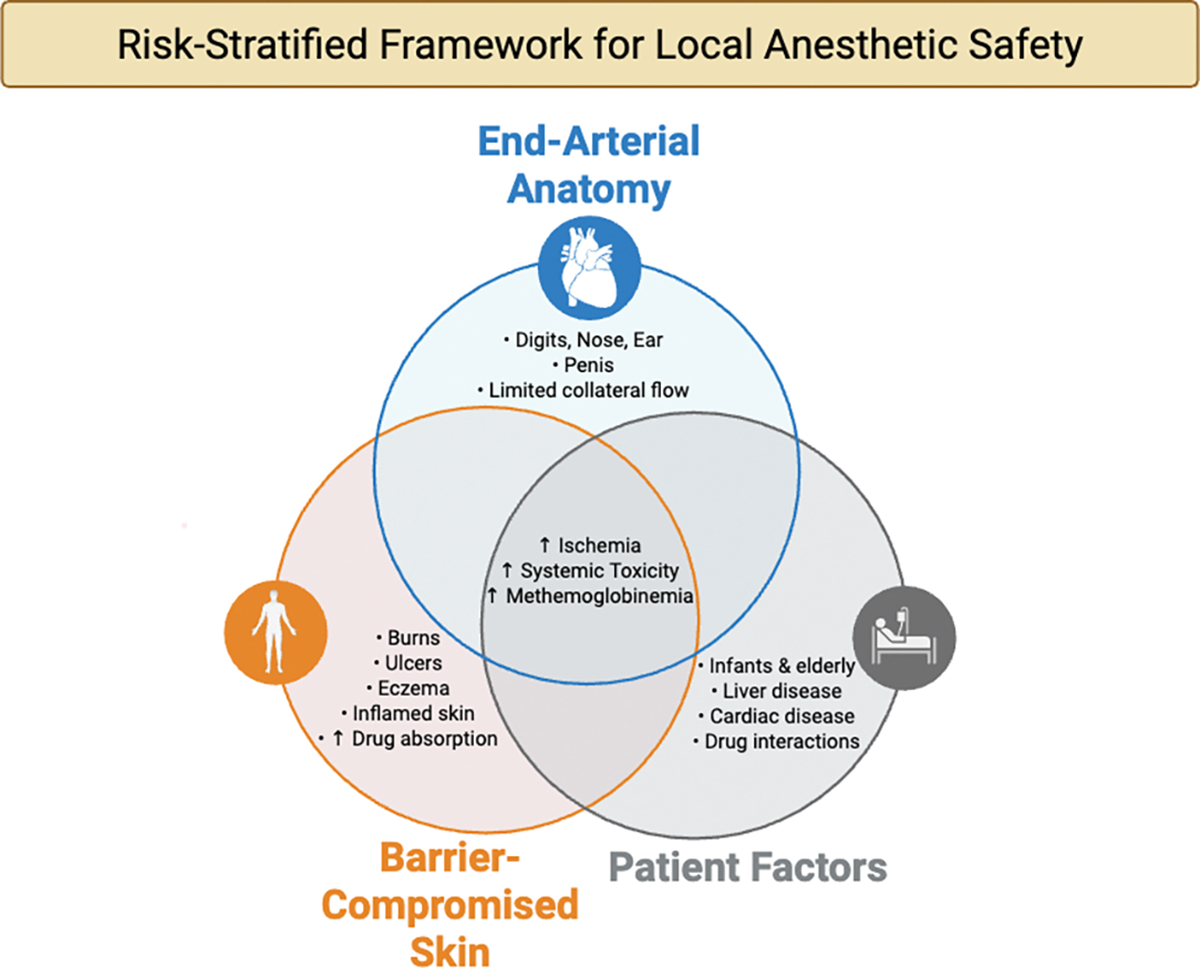 Figure 1
Figure 1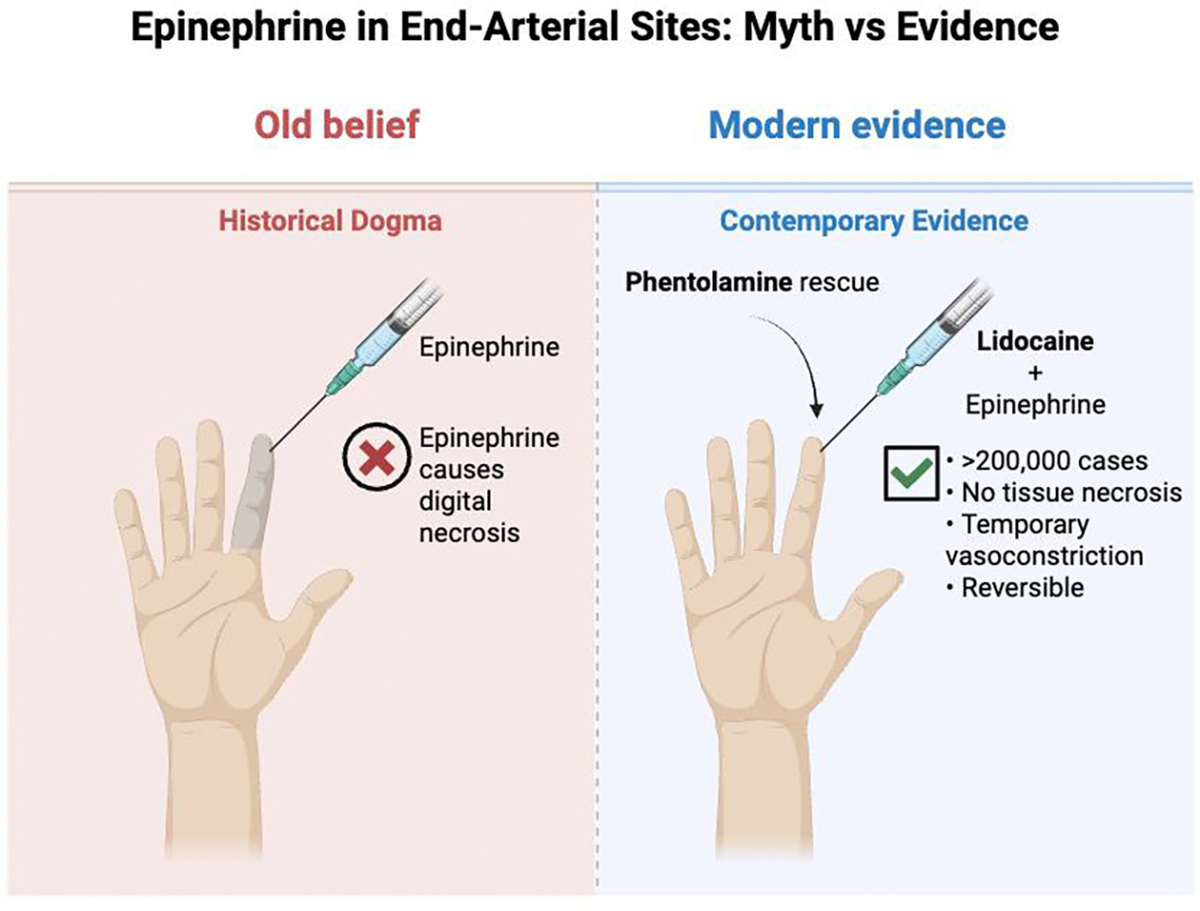 Figure 2
Figure 2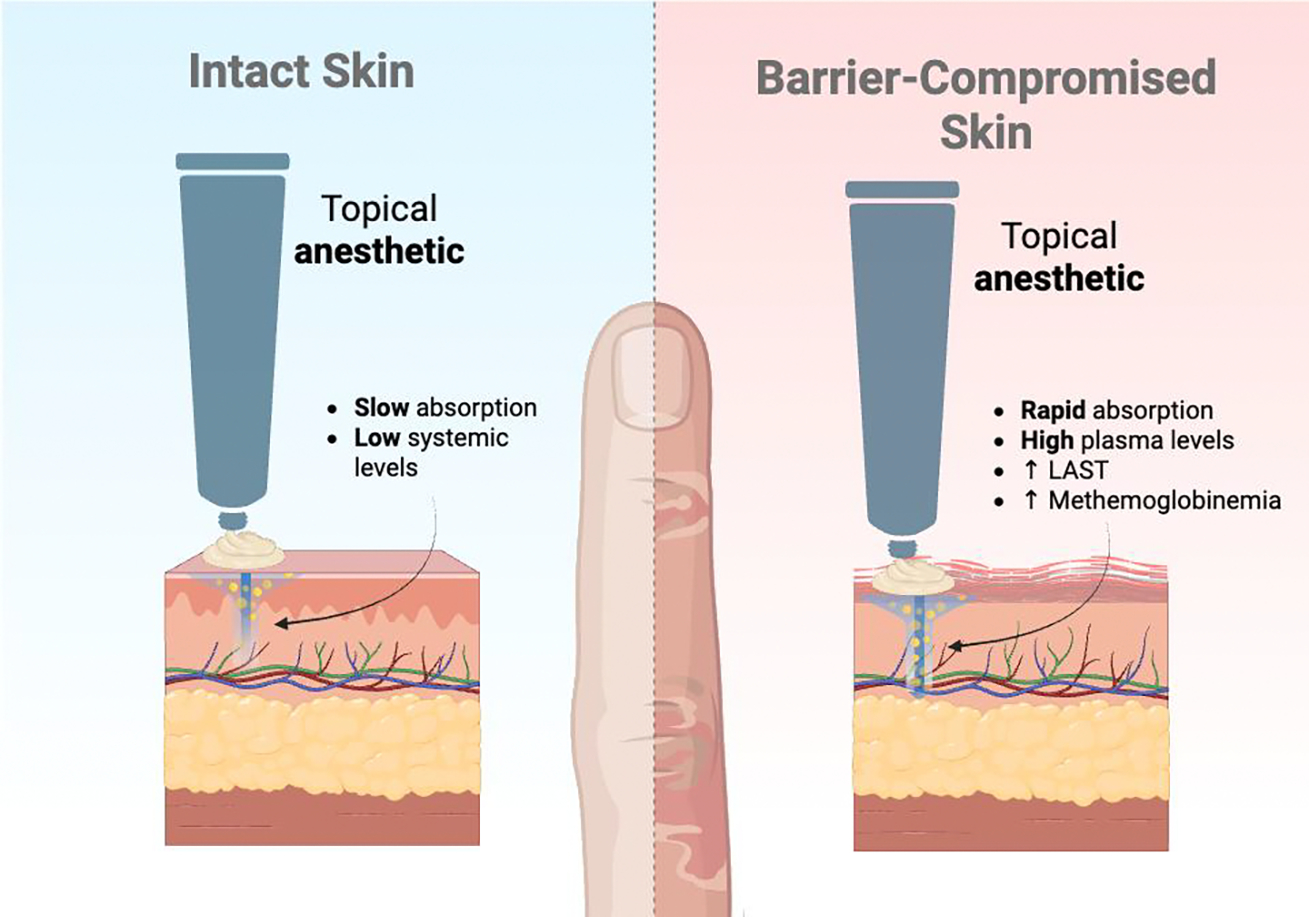 Figure 3
Figure 3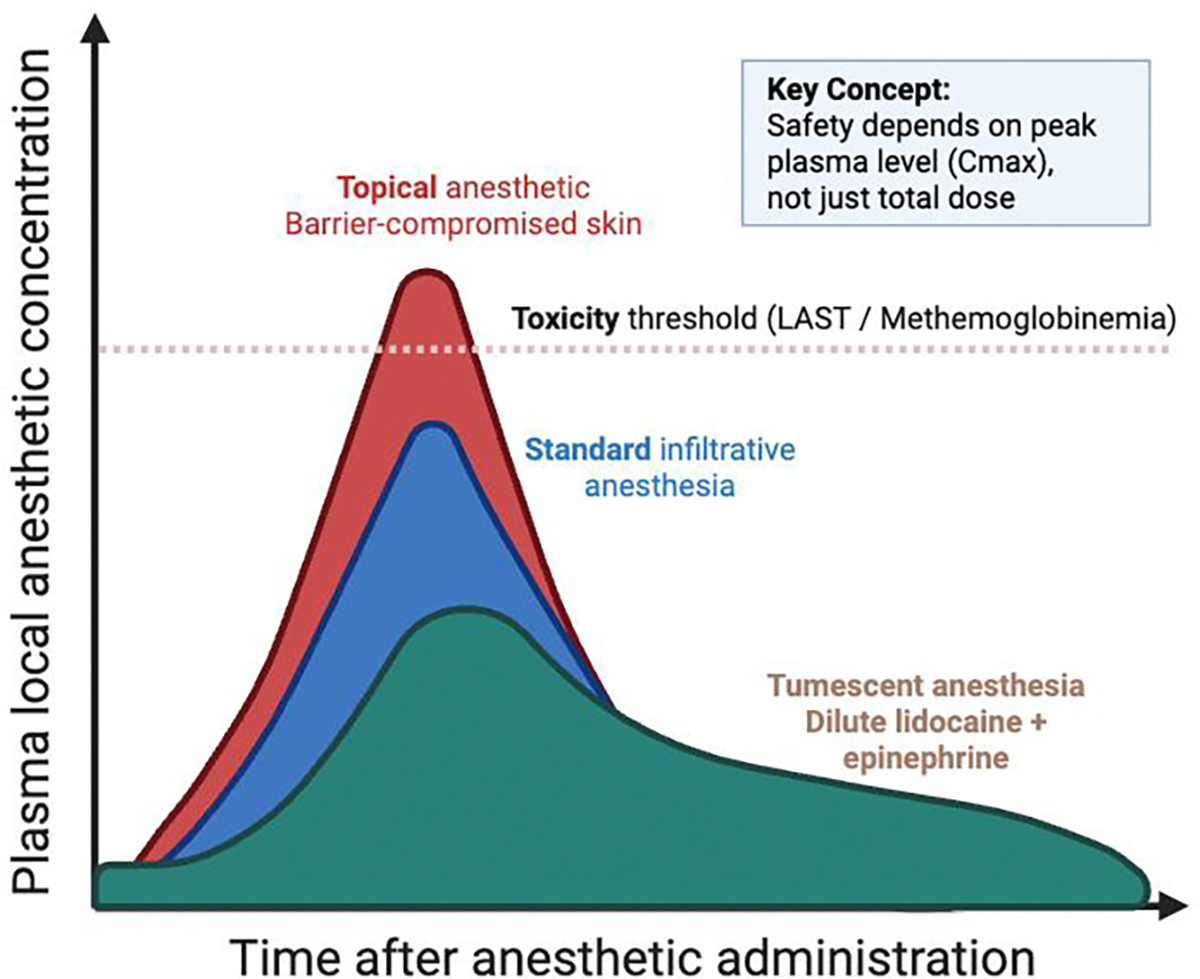 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDental Anxiety and Anesthesia Techniques · Surgical Sutures and Adhesives · Body Contouring and Surgery
Introduction
Reframing Safety: Beyond Routine Administration
1.1
For the purposes of this review, we define “high-risk dermatologic contexts” as scenarios in which small deviations in agent selection, dose, or technique can disproportionately increase the probability or severity of ischemic injury, systemic toxicity, or methemoglobinemia. These contexts arise from three interacting domains: anatomy, barrier status, and systemic milieu. Anatomically, end-arterial or functionally end-arterial territories (digital pulps, nasal tip, ear, penis) have historically been considered precarious with respect to vasoconstrictors, particularly in patients with peripheral arterial disease, Raynaud phenomenon, or thromboangiitis obliterans [1–3]. From a barrier perspective, partial-thickness burns, chronic leg ulcers, erosive disorders, and acutely inflamed dermatoses amplify transcutaneous absorption of topicals and modify the pharmacokinetics of infiltrative agents [4,5]. Systemically, extremes of age, frailty, hepatic or cardiac impairment, and co-medications that inhibit cytochrome P450 enzymes or lower seizure threshold (e.g. β-blockers, SSRIs, TCAs, class I antiarrhythmics) further narrow the therapeutic window [6–8].
In such settings, global declarations of local anesthetic “safety” are insufficient. Instead, dermatologic practice requires a risk-stratified approach that integrates microvascular, barrier, and pharmacologic principles with the realities of office-based surgery: limited monitoring, variable emergency preparedness, and the increasing use of high-dose tumescent and topical regimens.
Objectives and Scope of This Review
1.2
This narrative review synthesizes and critically appraises the evidence base for the safety of topical and infiltrative local anesthetics in three interlocking high-risk domains central to dermatologic practice: end-arterial sites, barrier-compromised skin, and systemic toxicity. Our primary aim is to move beyond aphorism and isolated case reports toward an integrated framework that links drug structure, pharmacokinetics, vascular physiology, and clinical outcomes, and that can be translated into concrete, context-sensitive practice recommendations.
First, we examine the historical dogma and contemporary evidence for epinephrine safety in end-arterial territories. Second, we address the ‘absorption amplifier’ effect of barrier compromise, comparing topical anesthetic behavior across intact, burned, ulcerated, and inflamed skin. Third, we provide a comprehensive framework for LAST risk factors, recognition, and management.
The intended audience includes dermatologic surgeons, cutaneous oncologists, procedural and cosmetic dermatologists, pediatric dermatologists, hand and reconstructive surgeons using wide-awake local anesthesia, and allied specialties that intersect with dermatologic anesthesia. By integrating pharmacologic foundations (Section II), site-specific risk analyses (Sections III and IV), systemic toxicity frameworks (Section V), population-tailored considerations (Section VI), and procedural strategies (Section VII), we aim to provide a cohesive, practice-oriented synthesis.
The goal of this critical review article is to preserve the recognition that local anesthetics are extraordinarily safe, while making explicit the contextual limits of that safety.
Literature Search and Selection
1.3
This narrative review was informed by a targeted, non-systematic search of the biomedical literature, with PubMed as the primary database. We searched from database inception through late 2025 using combinations of MeSH terms and free-text keywords related to our three focal domains, including “local anesthetic,” “lidocaine,” “bupivacaine,” “prilocaine,” “topical anesthetic,” “tumescent anesthesia,” “epinephrine,” “digital nerve block,” “end-arterial,” “digits,” “nose,” “ear,” “penis,” “burn,” “ulcer,” “barrier-compromised skin,” “methemoglobinemia,” and “local anesthetic systemic toxicity” (LAST). Additional relevant terms (e.g. “WALANT,” “wide-awake local anesthesia,” “pediatric,” “geriatric,” “peripheral arterial disease,” “Raynaud,” “Buerger’s disease”) were added iteratively as themes emerged. We restricted inclusion to human studies and English-language publications and prioritized original clinical data which was then supplemented by high-quality narrative reviews, pharmacologic monographs (e.g. StatPearls), and key guideline or consensus pieces where available. Study selection and appraisal were pragmatic and purpose-driven rather than protocolized. No formal risk-of-bias assessment or meta-analysis was performed.
Pharmacologic foundations relevant to high-risk contexts
Local anesthetic safety in end-arterial sites, barrier-compromised skin, and large-field tumescent applications is fundamentally determined by the interplay between drug structure, pharmacokinetics, and the modifying effects of vasoconstrictors. Understanding these pharmacologic foundations is essential to rational risk assessment in settings where a small margin separates effective regional anesthesia from local anesthetic systemic toxicity (LAST), ischemia, or methemoglobinemia.
Pharmacokinetic Determinants of Safety
2.1
Lipid solubility and protein binding are the primary determinants of local anesthetic potency and duration. However, volume of distribution and elimination half-life further modulate risk. Lidocaine exhibits a relatively large volume of distribution between 0.7 and 1.5 L/kg and an elimination half-life between 1.5 and 2.0 hours in healthy adults, so transient overshoot in plasma levels is usually rapidly corrected if further absorption is curtailed [9,10]. Bupivacaine has a high degree of plasma protein binding (about 95%) and a longer elimination half-life than lidocaine: adult studies report a half-life of 2.7 hours, within a broader published range from 1.5 to 5.5 hours, so it accumulates more readily with repeated dosing or impaired clearance, and its high affinity for cardiac sodium channels means that malignant ventricular arrhythmias and cardiovascular collapse may occur at plasma concentrations only slightly above the therapeutic range [9,11,12]. Prilocaine is intermediate in half-life but carries a qualitatively distinct risk: metabolism to o-toluidine oxidizes hemoglobin to methemoglobin, producing cyanosis and tissue hypoxia at plasma levels that may still be sub-toxic for CNS and cardiovascular systems [13,14].
These properties translate into agent-specific toxicity profiles that are particularly relevant in high-risk dermatologic contexts. Lidocaine, because of its moderate lipid solubility and relatively low cardiotoxicity, typically manifests CNS excitation (tinnitus, peri-oral numbness, seizures) before cardiovascular collapse when LAST occurs, allowing a broader window for recognition and intervention [15]. Bupivacaine and, to a lesser extent, ropivacaine may precipitate abrupt ventricular arrhythmias or asystole with only minimal antecedent neurologic warning, making them less forgiving in office-based settings with limited resuscitative capacity [9]. Prilocaine, particularly in topical eutectic mixtures of local anesthetics (EMLA; 2.5% lidocaine / 2.5% prilocaine), can elicit clinically significant methemoglobinemia in infants, patients with G6PD deficiency, and when applied to large areas of barrier-defective skin [13,14].
Thus, the choice of agent in digits, acral sites, or on denuded dermis should be informed by more than duration alone. Highly lipophilic, long-acting agents (bupivacaine) should be reserved for limited-volume nerve blocks in monitored settings, whereas lidocaine (with or without prilocaine in topical mixtures) should be used with strict surface area and dose limits when applied to barrier-compromised skin [9].
The Epinephrine Paradox: Adjuvant and Risk Modifier
2.2
Epinephrine (adrenaline) is the prototypical vasoconstrictor adjuvant in local anesthetic solutions. By activating α₁-adrenergic receptors on arteriolar smooth muscle, it reduces local blood flow, thereby decreasing systemic uptake, prolonging nerve block duration, and improving intraoperative hemostasis [16,17]. These absorption-flattening effects are central to the safety of high-volume tumescent anesthesia and allow larger total lidocaine doses to be used with acceptably low peak plasma levels (section 5.1).
Epinephrine’s longstanding avoidance in end-arterial sites is revisited in detail in section III. This creates the central paradox: its α₁-mediated vasoconstriction is the primary safeguard against systemic toxicity in high-volume anesthesia (by slowing uptake and lowering C_max), yet this same mechanism is the source of the historical fear regarding ischemic necrosis in digits.
End-arterial sites: dismantling dogma with evidence
Local anesthetic use in end-arterial territories which includes digits, nasal tip, ear, and penis has historically been constrained by the fear that epinephrine-induced vasoconstriction could irreversibly occlude already tenuous blood flow. Contemporary pharmacologic and clinical data, however, demonstrate that this fear is largely unfounded when dilute epinephrine is used with modern amide anesthetics and meticulous technique.
Contemporary Evidence for Safety in Digits and Acral Sites
3.1
Over the past two decades, a robust body of evidence has emerged refuting the notion that dilute epinephrine in digital anesthesia causes ischemic necrosis in otherwise viable fingers or toes. A 2015 systematic review by Ilicki identified 23 studies encompassing 2,797 digital nerve blocks performed with lidocaine–epinephrine at concentrations between 1:100,000 and 1:200,000; no epinephrine-related cases of irreversible digital ischemia were identified [27]. In the Dalhousie multicenter prospective study, Lalonde and colleagues reported 3,110 consecutive elective finger and hand procedures performed with lidocaine and epinephrine, without any instances of digital infarction or need for amputation [28]. A separate prospective cohort of 1,340 digital surgeries using lidocaine 1% with epinephrine 1:100,000 likewise reported no ischemic complications or tissue necrosis [2].
Large prospective and retrospective cohorts corroborate this safety profile. Beyond the Dalhousie series, subsequent WALANT reports have described several hundred to many thousands of hand procedures performed with lidocaine and epinephrine, again without epinephrine-attributed digital tissue loss [2]. When these modern hand-surgery data are considered together with the classic podiatric series of more than 200,000 forefoot and toe operations performed using lidocaine with epinephrine at concentrations of 1:100,000 to 1:200,000, the published literature now documents well over 200,000 acral injection (including more than 200,000 from podiatric series alone plus several thousand from hand-surgery cohorts) without a single confirmed case of digital infarction attributable to epinephrine [28].
Similar safety profiles extend to other acral sites. Häfner and colleagues reported more than 10,000 ear and nasal procedures performed with epinephrine-supplemented local anesthetics at concentrations in the range of 1:100,000 to 1:200,000, without flap loss or skin necrosis attributable to vasoconstriction [29]. In a subset of these patients, perfusion measurements at the earlobe showed a 69% reduction in laser Doppler blood-flow signal and a 42% reduction in arterial inflow immediately after injection, yet blood supply remained present and no tissue necrosis occurred [29].
Physiologic studies provide mechanistic support. In a double-blind randomized trial of 20 healthy volunteers, Häfner et al. found that digital Oberst blocks using 6 mL of lidocaine 1% with epinephrine 1:200,000 reduced acral blood flux by a maximum of 55% for a mean duration of 16 minutes; perfusion measurements at 6 hours and 24 hours were indistinguishable from baseline [29]. In a separate WALANT study of 17 patients, Moog et al. injected 5 to 7 mL of articaine 1% with epinephrine 1:200,000 at the finger base and observed at least a 30% drop in capillary-venous oxygen saturation in 7 patients and short episodes of critical oxygen saturation in 4 patients, each lasting a mean of 133 seconds; oxygen saturation had returned to non-critical values in all patients by the end of the 32-minute observation period and no postoperative ischemic complications were seen [30]. Taken together, these data indicate that standard clinical doses cause a marked but short-lived reduction in digital perfusion that normal tissues tolerate without infarction.
Even in extreme “stress tests” of digital circulation such as accidental auto-injector injuries with epinephrine 1:1,000 into a single finger, permanent tissue loss has been exceedingly rare. Fitzcharles-Bowe et al. reviewed 59 reported cases of high-dose epinephrine injection into digits and found no instances of digital necrosis, including 32 patients who received no specific vasodilator treatment [3]. In a separate poison-center cohort, Muck et al. identified 365 epinephrine injections to the hand over six years; 213 involved digits and 127 of these digital injections had documented follow-up. Four patients had transient ischemic changes, all of which resolved completely, and in two of these patients symptoms resolved within 2 hours; no patient required hospitalization, hand-surgery consultation, or surgical intervention [2]. These observations imply a substantial safety margin for dilute epinephrine in digital blocks, which use much smaller epinephrine doses than auto-injectors.
Collectively, contemporary clinical and physiologic evidence demonstrates that, in healthy digits and in most patients with common comorbidities, lidocaine with epinephrine at 1:100,000–1:200,000 provides longer anesthesia and superior hemostasis without a demonstrable increase in the risk of digital necrosis [2,3].
Risk Stratification in Compromised Vasculature
3.2
Peripheral Arterial Disease and Diabetes:
3.2.1
The reassuring safety data for epinephrine-containing anesthetic in end-arterial sites largely derive from populations with normal or only mildly impaired digital perfusion. Nonetheless, limited evidence suggests that even patients with common vascular comorbidities tolerate epinephrine well when perfusion is clinically adequate. Several WALANT cohorts have explicitly included substantial proportions of patients with hypertension, diabetes, smoking history, or antiplatelet and anticoagulant therapy, yet none of these series reported digital ischemia, blistering, or necrosis attributable to epinephrine [2]. Other reports have deliberately included patients described clinically as having “poor circulation” and still found no epinephrine-related necrotic complications [2].
Notably, most large WALANT series either excluded patients with overt ischemic signs (rest pain, tissue loss, prior digital infarction) or used epinephrine cautiously or not at all in those with critical limb ischemia, Buerger’s disease, or severe scleroderma [28]. Thus, the observed absence of necrosis in “at-risk” circulation likely reflects a combination of true safety in mild–moderate peripheral arterial disease (PAD) and selection bias away from those with severely compromised flow.
From a pragmatic standpoint, the absence of documented epinephrine-related necrosis in diabetics and patients with non-critical PAD suggests that routine exclusion of epinephrine in all such patients is unnecessarily conservative. However, when objective measures such as ankle–brachial index (ABI <0.4), monophasic toe pressures, tissue loss, or prior digital amputations indicate severely impaired perfusion, the marginal benefit of epinephrine (longer anesthesia, better hemostasis) may be outweighed by the theoretical risk of tipping precarious microcirculation into infarction. In these individuals, plain lidocaine or proximal nerve blocks without epinephrine remain reasonable alternatives.
Vasospastic Disorders (Raynaud phenomenon, Buerger’s Disease):
3.2.2
Patients with primary Raynaud phenomenon, secondary Raynaud’s due to connective tissue disease, or thromboangiitis obliterans (Buerger’s disease) represent a distinct category in whom α-adrenergic vasoconstriction may elicit exaggerated and prolonged digital vasospasm. Case reports describe unusually severe ischemic responses: for example, a patient with Raynaud’s who developed marked digital pallor, pain, and superficial blistering after a standard epinephrine-containing injection, with eventual but delayed reperfusion [1]. Historical cases of digital necrosis in scleroderma or mixed connective tissue disease have also been reported, though confounding factors such as infection and baseline microvascular obliteration complicate causal attribution [2].
Pathophysiologically, Raynaud’s digits exhibit hypersensitivity of α_2-adrenergic receptors on digital arteries and arterioles, leading to disproportionate vasoconstriction in response to cold or catecholamines; Buerger’s disease is characterized by segmental inflammatory thrombosis of small and medium arteries and veins. Superimposing pharmacologic vasoconstriction on such structurally or functionally compromised vessels could, in theory, produce critical ischemia even with doses safe in normal digits. This theoretical vulnerability, coupled with case-level signals, has led most WALANT proponents to list active severe Raynaud’s and Buerger’s disease among the few relative contraindications to epinephrine in digital blocks [28].
In the absence of robust prospective data, a conservative posture remains prudent: avoid epinephrine in patients with clinically evident vasospastic episodes, rest pain, or trophic changes, and favor plain lidocaine or more proximal blocks in these individuals.
Proposed Risk Assessment Framework:
3.2.3
Given the heterogeneity of vascular reserve among patients, a binary “epi or no epi” rule is inadequate. Instead, a structured risk assessment may be more appropriate. Clinically relevant elements include patient-level factors such as documented PAD (ABI and toe pressures), diabetes duration and complications, smoking history, prior digital ulcers or amputations, Raynaud’s attacks, and systemic vasculitis, as well as procedure-level factors such as the planned anatomic site, depth of dissection, anticipated bleeding, and the total volume and concentration of epinephrine.
A practical framework might categorize patients into low, intermediate, and high vascular risk. Low-risk patients have normal pulses, no history of ischemic events, and no systemic vasculopathy; in them, standard concentrations of lidocaine with epinephrine (1:100,000–1:200,000) can be used freely in digits, nose, ear, and penis, with phentolamine available for rare prolonged blanching. Intermediate-risk patients include diabetics with intact but diminished pulses or smokers with mild PAD but no rest pain or tissue loss; in this group, epinephrine use remains reasonable but should be limited to the minimum effective concentration and volume, with careful monitoring of digital coloration and capillary refill post-injection and a low threshold for phentolamine reversal if reperfusion is delayed. High-risk patients such as those with critical limb ischemia (typically ABI ≤0.4 and/or toe pressures <30 mmHg), active ulceration or gangrene, prior digital infarction, severe vasospastic disorders, or inflammatory vasculitis, should generally avoid epinephrine in end-arterial injections; anesthesia should instead be achieved with plain lidocaine, proximal nerve blocks away from critically ischemic segments, or regional techniques under monitored conditions.
Such a qualitative algorithm, while not yet prospectively validated, concretizes the logic already applied in expert WALANT series, which systematically excluded patients with “significant pre-existing hand or finger ischemia” from epinephrine use [28]. Future work incorporating objective vascular measurements (ABI, toe pressures, nailfold capillaroscopy) and prospective outcomes could refine this into a validated digital perfusion risk score.
Phentolamine Rescue: The Safety Net
3.3
Phentolamine, a non-selective α-adrenergic antagonist, provides an effective pharmacologic antidote to epinephrine-induced vasoconstriction. By competitively displacing epinephrine at α₁-receptors, it induces rapid arteriolar dilation and restoration of blood flow [28]. In the context of digital anesthesia, phentolamine rescue should be considered whenever blanching, pain, or impaired capillary refill persists beyond the expected window of epinephrine effect, or at any earlier point if there are clinical signs of progressive digital ischemia, particularly in high-risk patients. Key clinical and physiologic data supporting the safety of epinephrine in end-arterial sites are summarized in table 2.
A commonly recommended protocol involves reconstituting phentolamine to 1 mg/mL and infiltrating 1–5 mg subcutaneously in and around the ischemic area, using multiple small injections circumferentially proximal to and within the original anesthetic field [28]. In an experimental human study, Nodwell and Lalonde showed that injecting 1 mg of phentolamine in 1 mL of saline at the site of vasoconstriction shortened the time for epinephrine-induced digital blanching to resolve from a mean of 5 hours 19 minutes with placebo to 1 hour 25 minutes with phentolamine [3]. Case reports of accidental high-concentration epinephrine auto-injector injuries describe rapid restoration of digital perfusion after local phentolamine injection, with preservation of tissue and no subsequent necrosis in the reported cases [2,3].
Timing is paramount. Experimental and clinical data indicate that digital tissues can tolerate only a limited period of severe ischemia before the risk of irreversible damage rises [31]. In a recent report of digital ischemia after an adrenaline-based block, delayed recognition and late administration of phentolamine were followed by only partial recovery of perfusion and distal tissue loss, suggesting that an earlier intervention might have prevented necrosis [32]. On this basis, several authors advocate administering phentolamine once it is clear that perfusion is not beginning to recover such as when normal coloration and capillary refill have not started to improve by 60 minutes in a previously healthy digit or sooner in patients with compromised vascular reserve.
Phentolamine itself is hemodynamically active; systemic absorption can cause transient hypotension and tachycardia, though these are usually mild at doses used for digital rescue [28]. Having phentolamine stocked and staff trained in its use therefore substantially enhances the safety net for using epinephrine in end-arterial sites. It converts a theoretical one-way door of vasoconstriction into a reversible pharmacologic state, further supporting the argument that with appropriate infrastructure, epinephrine in digits and other acral sites is not only safe but controllable.
Barrier-Compromised Skin: The Absorption Amplifier
Clinical Consequences of Excessive Absorption
4.1
Systemic Local Anesthetic Toxicity (CNS/Cardiovascular):
4.1.1
The amplified absorption from barrier-compromised skin translates into an increased risk of frank local anesthetic systemic toxicity (LAST). Case reports span pediatric and adult populations and frequently involve either diseased skin, extensive application, occlusion, or high-concentration compounded formulations. In a four-year-old child with atopic dermatitis and molluscum contagiosum, EMLA was applied under occlusion to numerous lesions; within a short period the child developed seizures and cyanosis, with documented methemoglobinemia and clinical features consistent with combined prilocaine-induced oxidant stress and systemic lidocaine toxicity [34]. A recent adult case involved a 71-year-old man with a chronic venous leg ulcer who received EMLA over the ulcer bed; within 45 minutes he became somnolent and cyanotic, with a methemoglobin level of 15.1% and central nervous system depression that resolved only after removal of the cream and supportive oxygen therapy [13].
Topical overuse on procedurally ablated skin can be equally hazardous. A report of fractional laser resurfacing described systemic lidocaine toxicity after the application of a 30% lidocaine gel to the treated area, with ensuing neurologic symptoms requiring emergent care [35]. The most dramatic illustration of this risk came in 2005, when two young women died after using high-strength, compounded lidocaine/tetracaine gels on their legs under plastic occlusion before laser hair removal [6,25]. Both developed seizures and cardiac arrest en route to treatment facilities. The subsequent FDA advisory explicitly linked the fatalities to the combination of large surface area, high concentration, barrier disruption from shaving, and occlusion, all of which accelerated systemic uptake [25].
These cases underscore that the canonical CNS prodrome of LAST (peri-oral numbness, tinnitus, lightheadedness, confusion) may be brief or even unrecognized when high systemic levels are achieved rapidly from compromised skin, particularly outside monitored settings [6,9]. For dermatologic practice, they mandate that topical regimens on barrier-compromised skin be considered pharmacologically equivalent to substantial systemic dosing and be prescribed and monitored with the same vigilance as infiltrative anesthesia.
Methemoglobinemia
4.1.2
On compromised skin, rapid systemic delivery of prilocaine and benzocaine increases the risk of methemoglobinemia, particularly in infants and oxidant-vulnerable adults. Key risk factors in barrier-compromised contexts include high total dose, large surface area of denuded skin, mucosal application, and host vulnerability (age <6 months, G6PD deficiency, concurrent oxidant medications). Full pathophysiology, recognition, and management with methylene blue are detailed in section 5.3 [34,36].
Evidence-Based Application Algorithms by Disease State
4.2
Translating pharmacokinetic and toxicologic data into practical guidance requires disease-specific algorithms that explicitly adjust for barrier status.
In atopic dermatitis, the combination of increased permeability and inflamed microvasculature dictates conservative topical regimens. Data published by Juhlin demonstrate that on eczematous skin, EMLA achieves adequate anesthesia with contact times as short as 5–15 minutes [37]. For adults and older children with localized lesions, a thin layer of EMLA or 4–5% lidocaine cream limited to the minimal necessary area and removed after 15–30 minutes is usually sufficient, obviating the standard 60-minute exposure used on intact skin [9,37]. Occlusion should be avoided whenever the epidermis is visibly inflamed or fissured. In young children, particularly those under three years, lidocaine-only preparations in small quantities are preferable to prilocaine-containing EMLA to mitigate methemoglobin risk [13,14].
For chronic venous or pressure ulcers, the leg-ulcer pharmacokinetic studies define relatively generous but still safe limits within the PK range shown in table 3 [5,38]. In frail elderly or patients with significant hepatic impairment, lower doses with longer intervals are prudent.
Partial-thickness burns require the most caution. For analgesia during burn dressing changes, topical anesthetics should be restricted to discrete, limited areas and contact times kept to 30–45 minutes. When larger segments require debridement or grafting, staged procedures and dilute tumescent or regional infiltration offer a safer profile than attempting to anesthetize the entire field with topical agents [39,40].
For inflammatory dermatoses overall (psoriasis, lichen planus, erosive disorders), a pragmatic rule is to limit both dose per unit area and contact time to no more than half of the amounts used in intact-skin protocols, avoid occlusion over any visibly eroded surface, and favor lidocaine-only formulations in children, patients with G6PD deficiency, or those requiring repeated treatments [9,13,14].
Age-Stratified Safety Considerations
4.3
Age modifies the impact of barrier compromise on systemic exposure: infants/young children, and frail older adults, have much narrower therapeutic windows. Infants have a higher surface-area-to-body-weight ratio, immature hepatic metabolism, and reduced methemoglobin-reducing capacity [6,13,14]. Frail older adults often have reduced hepatic blood flow and polypharmacy that slows clearance.
In practice, this means that pediatric and geriatric dosing on barrier-compromised skin should be substantially more conservative than in healthy adults. Detailed age-specific recommendations including tight labeled pediatric limits and dose reductions in frail elders are provided in section VI and tables 3 and 4.
Topical vs. Tumescent Infiltration: Optimal Strategy for Large Areas
4.4
For large areas of barrier-compromised skin such as extensive partial-thickness burns, large ulcers, or wide erosive fields, the clinician must decide between escalating topical therapy and transitioning to dilute infiltrative techniques. Pharmacokinetic principles strongly favor tumescent or field infiltration for such indications.
Tumescent anesthesia employs very dilute lidocaine (typically 0.05–0.1%) with epinephrine, infiltrated in substantial volumes into subcutaneous tissue until tumescence is achieved [17]. The combination of extreme dilution and epinephrine-mediated vasoconstriction produces slow, delayed systemic uptake: in tumescent liposuction with a mean lidocaine dose of 33.2 mg/kg, mean peak serum lidocaine concentration is 2.3 μg/mL (standard deviation 0.63 μg/mL), occurring 5–17 hours after infiltration, and all observed values remain below 6 μg/mL, the commonly used threshold for mild systemic toxicity [26,41]. In burn surgery, analogous tumescent protocols using 0.1% lidocaine with epinephrine for debridement and grafting of extensive burned areas have been reported as simple, effective, and safe, with no clinically significant systemic toxicity and excellent analgesia and hemostasis [39,40].
In contrast, applying even moderate-concentration topical anesthetic over a large, denuded surface creates a rapid, uncontrolled absorptive interface. As the burn-ointment case illustrates, 5% lidocaine on 28% body surface area can produce near-toxic peaks within hours [4], whereas an equivalent or higher total dose delivered tumescently yields a much flatter concentration–time curve with a lower C_max and wider safety margin [17,26,41].
From a practical standpoint, topical anesthesia is best reserved for small, discrete compromised areas (for example ≤25–50 cm^2^) and as an adjunct to reduce injection pain. For large contiguous areas of partial-thickness injury or ulceration for example, treatment fields larger than 100 cm^2^, which far exceeds the maximum labeled intact-skin area of 20 cm^2^ for 2 g of EMLA in infants 3–12 months or when multiple sessions on the same field are planned, staged dilute infiltration or tumescent anesthesia is generally a safer and more controllable strategy than escalating topical doses. Epinephrine in the tumescent solution not only slows systemic lidocaine uptake but also provides superior hemostasis, which is particularly advantageous in debridement and grafting of vascular wound beds [17,42].
A rational decision framework thus weighs surface area, depth of injury, need for hemostasis, patient comorbidities, and the cumulative anesthetic burden. Small islands of erosive disease or isolated ulcers can be managed with carefully dosed topical agents. Larger, contiguous areas of barrier loss, particularly in adults with reasonable cardiopulmonary reserve, are better served by dilute lidocaine with epinephrine delivered via tumescent or field infiltration, with dose calculations anchored to tumescent safety data and the availability of monitoring and lipid rescue for rare systemic events [17,26,41].
Local Anesthetic Systemic Toxicity (Last): From Rare To Manageable
Risk Factors for Systemic Toxicity
5.1
Dose and Concentration Variables:
5.1.1
Systemic toxicity is fundamentally dose-dependent, modulated by concentration, route, and rate of administration. Expert consensus and anesthesia literature provide maximum recommended mg/kg doses for infiltrative use of common agents (Table 5). For dermatologic practice, the key principle is that these limits represent upper bounds under ideal conditions; in frail, pediatric, or comorbid patients, and when multiple modalities (topical, infiltrative, tumescent) are combined, substantially lower thresholds are appropriate.
Concentration strongly influences both injection pain and systemic risk. Higher concentrations (e.g. 2% lidocaine) provide no additional depth of block over 0.5–1% for most cutaneous procedures but increase the per-milliliter drug load. Recent dermatologic trials show that 0.25–0.5% lidocaine with epinephrine provides non-inferior analgesia for Mohs surgery and excisions compared with 1–2% solutions, while 1:2 and 1:6 dilutions of 2% lidocaine with epinephrine reduce the per-milliliter lidocaine content by 66.7% and 85.7%, respectively, and significantly lower injection pain scores [49,50]. Using the lowest effective concentration is therefore a straightforward, evidence-based strategy to widen the safety margin.
As shown in pharmacokinetic work on tumescent anesthesia (section 7.1), maximum safe dose is tightly linked to concentration and absorption rate.
Site of Administration:
5.1.2
Anatomic site influences systemic uptake through differences in vascularity and barrier integrity. Highly perfused areas such as the face, scalp, genitalia, and mucous membranes absorb local anesthetics more rapidly than the trunk or extremity skin, increasing peak plasma concentrations for a given dose [9]. Topical anesthetics on mucosa or denuded dermis behave pharmacokinetically more like parenteral administration [25].
By contrast, subcutaneous or intradermal infiltration into intact skin yields comparatively slow absorption, especially when epinephrine is included [16]. As detailed in Section IV, barrier-compromised skin can convert percutaneous absorption from a diffusion-limited to a perfusion-limited process, markedly increasing systemic exposure to topical agents.
Patient-Specific Vulnerabilities:
5.1.3
Host factors can narrow the margin between therapeutic and toxic plasma levels. Extremes of age are particularly important. Neonates and young infants have immature hepatic cytochrome systems, reduced α-1-acid glycoprotein levels, and a higher unbound fraction of amide anesthetics, lowering the threshold for CNS and cardiovascular toxicity [13,14]. Their higher surface-area-to-weight ratio also amplifies systemic uptake from topicals [6].
Elderly and frail patients often have reduced cardiac output, diminished hepatic blood flow, and polypharmacy, all of which may slow anesthetic clearance and reduce physiologic reserve in the face of hypotension or arrhythmias [6]. In such individuals, conservative dosing (for example, a 20% reduction from standard adult maximum doses), use of dilute solutions, and avoidance of rapid, large boluses are prudent [6].
Hepatic dysfunction directly impairs metabolism of amide anesthetics (lidocaine, bupivacaine, mepivacaine, prilocaine), prolonging half-life and increasing AUC at any given dose [6]. Severe cardiac disease reduces hepatic perfusion and therefore clearance; concomitant heart failure also diminishes tolerance for negative inotropy or arrhythmias. Patients with advanced renal disease are less susceptible to unchanged drug accumulation but may accumulate active metabolites (e.g. prilocaine’s o-toluidine), heightening the risk of methemoglobinemia [13,14].
Finally, patients with pre-existing neurologic disease, seizure disorders, or medications that lower seizure threshold (e.g. SSRIs, TCAs) may manifest CNS toxicity at lower plasma concentrations [9,26,41].
The Cumulative Dose Problem
5.2
In contemporary dermatologic practice, patients increasingly undergo multiple procedures, including ablative laser resurfacing, serial photodynamic treatments, staged excisions, and combined aesthetic interventions, within compressed timeframes. Each encounter may involve topical anesthetics, infiltrative lidocaine, nerve blocks, or tumescent solutions. Although any single exposure may remain comfortably within recommended limits, cumulative doses across modalities and sessions can approach or exceed thresholds for toxicity if not consciously tracked.
Lidocaine has a plasma elimination half-life of 90–120 minutes in healthy adults, but with tumescent infiltration, peak serum lidocaine concentrations typically occur 8–14 hours after injection, within a reported range of 5–17 hours and clinically significant absorption and analgesia can persist for up to 18 hours [26,51]. Consequently, lidocaine administered in the morning may still contribute appreciably to plasma levels during an afternoon or evening procedure, particularly in patients with reduced clearance. Similar principles apply to prilocaine, where repeated topical applications in close succession can allow accumulation of oxidizing metabolites and progressive methemoglobinemia [13,14].
Case analyses from tumescent liposuction have shown that patients receiving cumulative doses near the upper recommended range may develop mild neurologic symptoms which includes drowsiness, confusion, perioral numbness at peak levels many hours post-procedure, especially when concomitant medications impair metabolism [26,41]. Although these events generally remain subclinical and self-limited, they underscore the potential for delayed toxicity when multiple large-dose exposures are temporally clustered.
Busy practices should therefore adopt explicit policies that treat all local anesthetic administered within a 24-hour interval as a single cumulative dose for safety calculations [26,41,51]. Electronic medical record prompts or dedicated dosing sheets can facilitate real-time summation of infiltrative, topical, and tumescent lidocaine (and other amide anesthetics), ensuring that the aggregate milligram load per kilogram remains within context-appropriate limits. Where same-day multiple procedures are unavoidable, clinicians should favor more dilute solutions, restrict topical surface area, and avoid stacking high-dose modalities (for example, combining high-dose EMLA on compromised skin with high-dose tumescent lidocaine).
Methemoglobinemia: A Distinct Toxicity Pathway
5.3
Methemoglobinemia represents a mechanistically distinct form of toxicity in which oxidizing local anesthetic metabolites convert ferrous (Fe^2+^) hemoglobin to the ferric (Fe^3+^) state, forming methemoglobin (MetHb) and impairing oxygen carriage and release [52]. Prilocaine and benzocaine are the principal culprits in dermatologic practice; lidocaine and articaine can contribute at high doses or in susceptible hosts but are far less potent oxidants [13,14].
Prilocaine’s metabolite o-toluidine is a well-recognized inducer of methemoglobinemia, particularly when cumulative doses exceed 2–2.5 mg/kg in infants or 600 mg in adults [44]. As a component of EMLA (2.5% prilocaine + 2.5% lidocaine), prilocaine has been implicated in cases of significant MetHb formation when applied to extensive eczematous skin, chronic ulcers, or under occlusion, especially in young children [13,34]. Benzocaine, widely used as a topical mucosal spray, has caused fulminant methemoglobinemia in infants and adults after relatively small exposures, reflecting its high oxidative potency and rapid mucosal absorption [36].
Risk factors include high total dose, young age (particularly <6 months, when NADH-methemoglobin reductase is immature), glucose-6-phosphate dehydrogenase (G6PD) deficiency, concurrent oxidant drugs (e.g. dapsone, nitrates, sulfonamides), anemia, and application to highly vascular or barrier-deficient surfaces [36,52]. In a series analyzing prilocaine-induced methemoglobinemia, higher prilocaine dose and younger age were the most significant predictors of elevated MetHb levels [53].
Clinically, patients present with slate-gray or cyanotic discoloration, disproportionate to measured arterial oxygen tension; pulse oximetry often plateaus around 80–85% despite supplemental oxygen, while PaO₂ remains normal [52]. Symptoms range from mild dyspnea and headache to confusion, tachycardia, and, at MetHb levels exceeding 30–40%, seizures, arrhythmias, and cardiovascular collapse may occur (methylene blue is typically indicated at MetHb ≥20% or with significant symptoms at lower levels).
Diagnosis is confirmed by co-oximetry, which directly quantifies methemoglobin fraction. Management hinges on immediate removal of the offending agent and, in symptomatic patients or those with MetHb ≥20%, administration of intravenous methylene blue at 1–2 mg/kg over 5 minutes (up to a total of 7 mg/kg), which accelerates reduction of methemoglobin via the NADPH-dependent pathway [13,14]. In G6PD deficiency, methylene blue may be ineffective or even harmful; in such cases, exchange transfusion or hyperbaric oxygen may be required [52]. Prevention in dermatologic practice rests on dose limitation of prilocaine-containing and benzocaine products, strict adherence to age-specific guidelines, and avoidance in known G6PD-deficient or very young infants [13,14].
Prevention Strategies
5.4
Robust prevention remains the most effective intervention against LAST and related toxicities. The cornerstones are accurate dose calculation, prudent technique, judicious use of vasoconstrictors, and appropriate monitoring.
Weight-based dosing should be routine for children, small adults, and any patient in whom large fields will be anesthetized. Clinicians must be comfortable converting concentration (% w/v) to milligrams per milliliter and summing all sources of drug including topical, infiltrative, nerve block, and tumescent components over a defined interval [6,26,41].
During infiltration and nerve blocks, small-volume, incremental injection with frequent aspiration is critical to avoid inadvertent intravascular administration, especially in highly vascular regions (face, scalp) and near named vessels [19]. Buffering lidocaine with sodium bicarbonate reduces injection pain without altering systemic absorption in a clinically meaningful way [54]. Slower, less painful injections may indirectly reduce vasovagal reactions and sudden patient movement that could precipitate vascular puncture.
The inclusion of epinephrine, when not contraindicated, significantly decreases systemic uptake and prolongs block duration, enabling lower total doses for equivalent procedural coverage [16,17]. Concerns about epinephrine in end-arterial sites have been largely allayed in healthy patients, but in severely vasculopathic digits or limbs, its use should remain conservative or be avoided [2,3]. Clinicians must account for drug-drug interactions detailed in Table 4.
Monitoring intensity should be tailored to anticipated systemic exposure. Minor excisions under small-volume infiltration may require only intermittent observation. In contrast, large-field tumescent anesthesia or multiple simultaneous procedures warrant baseline and periodic blood pressure, heart rate, and pulse oximetry measurements, and some experts advocate continuous monitoring akin to moderate sedation standards [6,17]. Particular vigilance is warranted in pediatric, geriatric, and medically complex patients.
Recognition and Emergency Management of LAST
5.5
Early Recognition: The Critical Window:
5.5.1
Timely recognition of evolving LAST is paramount; most patients exhibit a prodrome prior to seizures or cardiovascular collapse. Any sudden onset of tinnitus, circumoral numbness, metallic taste, agitation, or visual disturbance during or shortly after anesthetic administration should trigger immediate cessation of injection and focused assessment [19].
The differential diagnosis includes vasovagal syncope (pallor, bradycardia, hypotension, nausea, often triggered by needles or blood), panic or anxiety reactions (tachycardia, hyperventilation, paresthesia without objective neurologic signs), and allergic phenomena (urticaria, bronchospasm, hypotension) [55,56]. In contrast to LAST, vasovagal episodes rarely produce tinnitus, metallic taste, or focal neurologic symptoms and are promptly reversible with Trendelenburg positioning and reassurance. True IgE-mediated allergy to amide local anesthetics is exceptionally rare; most “allergic” reactions are vasovagal or pharmacologic epinephrine effects [6].
Recognition of a possible toxic prodrome should prompt stopping further anesthetic, summoning assistance, applying high-flow oxygen, establishing IV access, and preparing benzodiazepines and lipid emulsion in case of progression [19].
The Lipid Emulsion Revolution:
5.5.2
The introduction of intravenous lipid emulsion therapy has transformed the prognosis of severe LAST. Initially empirically observed in animal models and then in dramatic case reports of bupivacaine-induced cardiac arrest, 20% lipid emulsion is now a central component of resuscitation algorithms [19,48].
The predominant mechanistic hypothesis is the “lipid sink” or “lipid shuttle”: the intravascular lipid phase sequesters lipophilic local anesthetic molecules away from cardiac and neuronal membranes, reducing their effective tissue concentration and facilitating redistribution to metabolically active organs such as the liver [19]. Additional proposed mechanisms include direct positive inotropy and improved mitochondrial function.
Current American Society of Regional Anesthesia and Pain Medicine (ASRA)-endorsed dosing for severe LAST in adults recommends an initial bolus of 1.5 mL/kg of 20% lipid emulsion over 1 minute, followed by a continuous infusion at 0.25 mL/kg/min, with repeat bolus and increased infusion rate (up to 0.5 mL/kg/min) if hemodynamic instability persists, to a typical upper limit of 10–12 mL/kg total [19]. Numerous case series and registry data document successful reversal of otherwise refractory cardiac arrest and rapid neurologic recovery when lipid is administered early [48].
Given its life-saving potential, 20% lipid emulsion should be immediately available in any dermatologic or aesthetic practice that performs high-dose local anesthesia, tumescent procedures, or deep regional blocks [51].
Stepwise Management Algorithm:
5.5.3
The management of LAST rests on three pillars: airway and ventilation, seizure control, and cardiovascular support, integrated with lipid therapy and modified ACLS protocols [19,56].
Airway management is primary. Hypoxia and acidosis potentiate cardiotoxicity and lower seizure threshold; immediate administration of 100% oxygen and assisted ventilation with bag–valve–mask are essential, with early consideration of endotracheal intubation if consciousness is impaired [19].
Seizures should be treated promptly with benzodiazepines (e.g. midazolam 0.05–0.1 mg/kg IV, diazepam 0.1 mg/kg) or, if unavailable, small doses of propofol in hemodynamically stable patients [19]. Large boluses of propofol are discouraged in hemodynamically fragile patients due to its myocardial depressant effects.
For cardiovascular collapse, standard ACLS algorithms apply but with critical modifications. Epinephrine, if needed, should be used in reduced doses (e.g. 10–100 μg boluses rather than 1 mg) to avoid exacerbating arrhythmias or increasing myocardial oxygen demand [19]. Vasopressin, additional bolus lidocaine, and other class I anti-arrhythmics are contraindicated, as they may worsen sodium-channel blockade [48]. High-quality chest compressions should continue as lipid emulsion is administered; prolonged resuscitation efforts are justified because successful neurologic recovery after extended cardiac arrest has been documented when lipid therapy is employed [19].
In less dramatic presentations e.g. isolated seizures without hemodynamic compromise, supportive care and lipid may still be indicated if the total dose or agent (e.g. bupivacaine) portends a risk of delayed cardiac decompensation. Close monitoring for several hours is mandatory, as recurrent events can occur as tissue-bound anesthetic redistributes.
Office Preparedness: The LAST Kit:
5.5.4
Preparedness in the dermatologic office environment is central to translating these principles into outcomes. A dedicated “LAST kit” should be assembled and maintained, typically including 20% lipid emulsion (at least 500 mL), appropriately sized IV cannulas and tubing, benzodiazepines, airway adjuncts (oropharyngeal airways, bag–valve–mask), supplemental oxygen delivery systems, a defibrillator, and a printed or laminated stepwise management algorithm with dosing tables [51,56]. For practices that perform end-arterial blocks, inclusion of phentolamine for digital ischemia reversal is also advisable [2,3].
Lipid emulsion should be stored according to manufacturer recommendations, readily accessible in procedural areas, and monitored for expiration; replacing a 500 mL bag at least every 24 months, or earlier if the labeled expiry date is sooner, is inexpensive relative to the potential benefit [57].
Equally important is staff training. Periodic simulation-based drills, in which teams rehearse recognizing prodromal LAST, initiating airway support, and preparing lipid, significantly reduce time-to-treatment and improve adherence to protocols, based on experience from anesthesiology and emergency medicine [56]. In dermatology, where LAST events are infrequent, such simulations are arguably the only practical way to ensure that response pathways are retained and executable under stress.
Collectively, these data and frameworks support the central thesis that in dermatologic practice, LAST has shifted from an unpredictable catastrophe to a rare but manageable complication, if dosing is rational, patient and drug factors are appreciated, and teams are trained and equipped to respond swiftly.
Special populations: tailored approaches
Pediatric patients
6.1
Pediatric pharmacokinetics and pharmacodynamics differ substantially from adults and amplify both the benefits and risks of local anesthetics. Infants and young children have a higher surface-area-to-weight ratio, reduced levels of α1-acid glycoprotein, and immature hepatic enzyme systems, leading to higher free fractions and slower clearance of amide anesthetics such as lidocaine and prilocaine [6]. Because barrier disruption in atopic dermatitis and other pediatric dermatoses amplifies absorption (Section IV), topical doses and contact times must be reduced relative to intact-skin protocols [9].
Regulatory labeling reflects this vulnerability. EMLA (lidocaine 2.5% / prilocaine 2.5%) carries a methemoglobinemia warning and should not be used in: (1) preterm neonates with a gestational age <37 weeks, or (2) infants younger than 12 months who are receiving other methemoglobin-inducing drugs; neonates and infants younger than 3 months are particularly susceptible to prilocaine-associated methemoglobinemia because of immature MetHb-reducing pathways. Infants <6 months, with immature MetHb-reducing capacity, are especially vulnerable to prilocaine- and benzocaine-induced methemoglobinemia (Section 5.3) [13,14]. Age-specific intact-skin EMLA limits are summarized in Table 3; on diseased skin (for example, atopic dermatitis or chronic leg ulcers), we restrict both total dose and application time to values below those used on intact skin, in line with studies showing faster absorption and higher local and systemic concentrations on eczematous and ulcerated skin [47].
For infiltrative anesthesia, weight-based dosing must be non-negotiable. Standard maximum doses for lidocaine should be treated as ceilings, not targets, in children: weight-based infiltrative dosing should not exceed 4.5 mg/kg without epinephrine (some pediatric dental guidelines cite 4.4 mg/kg) or 7 mg/kg with epinephrine, and in infants and toddlers we avoid approaching these maxima [18]. Using more dilute solutions (0.25–0.5% lidocaine with epinephrine) allows coverage of larger fields with lower total drug load and reduced injection pain, while maintaining adequate anesthesia for cutaneous surgery [49,50]. Buffered and warmed solutions further attenuate injection pain and can be combined with very small-gauge needles [52,58].
In common pediatric procedures, a staged, layered strategy is usually safest. A thin layer of topical lidocaine (without prilocaine), applied to intact skin over a limited area for a brief period shorter than the standard adult application time, can blunt the initial needle sting [13,14]. On acutely inflamed or eczematous skin, we either avoid topical anesthetics altogether or use substantially lower doses and shorter application times than standard adult intact-skin protocols, favoring dilute infiltrative anesthesia for larger or highly inflamed fields, given the accelerated and enhanced absorption documented on diseased skin.
Parental anxiety is frequently as consequential as the child’s pain. Transparent counselling and informed consent in pediatrics should explicitly address off-label topical use on inflamed skin, the rare but real possibility of methemoglobinemia or seizures with prilocaine- and benzocaine-containing products, and the signs that would prompt emergent evaluation after discharge [52].
Geriatric and frail patients
6.2
In older adults, the pharmacology of local anesthetics is shaped less by chronological age than by cumulative organ dysfunction, comorbidity, and frailty. Amide anesthetics, including lidocaine and bupivacaine, rely on hepatic cytochrome P450 metabolism; aging is associated with reduced hepatic blood flow, diminished metabolic capacity, and lower plasma albumin and α1-acid glycoprotein concentrations, increasing the unbound fraction of drug and prolonging elimination [6]. Concomitant medications such as non-selective β-blockers, calcium channel blockers, and certain SSRIs further slow clearance or reduce cardiac output, thereby increasing area-under-the-curve exposure for a given infiltrated dose [6–8].
Frailty indices, which integrate functional status, comorbidity burden, and nutritional reserve, likely predict anesthetic risk more accurately than age alone. A frail octogenarian with congestive heart failure and cirrhosis will have markedly reduced lidocaine clearance and little physiologic reserve to tolerate even transient CNS or cardiovascular depression, whereas a robust septuagenarian may safely receive near-standard doses. Yet current dermatologic guidelines do not incorporate formal frailty assessments, and dosing remains largely anchored to adult mg/kg limits [6]. High-impact practice should move toward individualized dosing that treats advanced frailty as a relative “dose-reducing comorbidity,” analogous to hepatic insufficiency.
Pragmatically, in elderly patients with significant frailty, hepatic dysfunction, or polypharmacy that impairs clearance, we limit lidocaine to a maximum of 4–5 mg/kg, even though standard adult limits for lidocaine with epinephrine allow doses up to 7 mg/kg, and we reduce other amide doses analogously [6]. Preferential use of more dilute solutions (0.25–0.5% lidocaine with epinephrine) and smaller total volumes can often achieve adequate field anesthesia in atrophic geriatric dermis, which allows wider spread of injectate [49]. Epinephrine remains useful for reducing systemic uptake and improving hemostasis, but transient tachycardia and blood pressure elevations may unmask coronary insufficiency; cautious titration and avoidance of large, rapid boluses are warranted in patients with unstable coronary disease or significant arrhythmias [6].
Monitoring thresholds should be lower in frail elders. For any procedure requiring moderate-to-large volumes of anesthetic, or incorporating tumescent technique, baseline and interval vital signs and pulse oximetry are appropriate; continuous ECG monitoring is reasonable when doses approach the upper end of the reduced geriatric range, or in those with structural heart disease [51]. Cognitive changes, dizziness, or new confusion in the hours after a procedure should trigger evaluation for subclinical systemic toxicity, which appears at lower plasma thresholds in frail patients than in healthy adults [6].
Procedural techniques influencing safety
Tumescent technique: the high-volume safety paradigm
7.1
Tumescent anesthesia exemplifies how procedural technique can recast toxicity risk. By combining extreme dilution of lidocaine (0.05–0.1%) with epinephrine 1:1,000,000 in large volumes instilled into subcutaneous fat until tissues are firm, tumescent infiltration produces profound regional anesthesia, hydrodissection, and hemostasis while dramatically slowing systemic uptake [17]. Pharmacokinetic studies show that within evidence-based mg/kg ranges, tumescent anesthesia yields peak serum lidocaine concentrations well below the 6 μg/mL threshold for mild CNS toxicity, with peaks delayed for many hours after infiltration [26]. Epidemiologic reviews encompassing 396,457 tumescent liposuction procedures performed with tumescent anesthesia as the sole anesthetic technique and following contemporary dosing protocols have not identified a single tumescent-anesthesia–associated death [59,60].
Safety in this paradigm depends critically on infusion rate and infiltration pattern. Slow, staged instillation (often via a pump or pressure bag) into a fan or grid of subcutaneous tunnels allows epinephrine’s vasoconstriction to develop as lidocaine is deposited, limiting early systemic escape and flattening the plasma concentration–time curve [17,26,41]. Segmenting very large fields (for example, tumescing one limb or oncologic field, completing surgery, then tumescing the next) further reduces peak levels by distributing absorption over time. The same principles underlie the successful extension of tumescent anesthesia beyond liposuction to extensive Mohs surgery, large excisions and flap/graft reconstructions, full-face laser resurfacing, hair transplantation, axillary hyperhidrosis surgery, and even burn debridement [39,51].
Despite its “mega-dose” appearance on paper, tumescent anesthesia should be viewed as a safety-enhancing technique in high-risk dermatologic settings where large areas must be anesthetized and topical strategies would entail unpredictable, rapid absorption through compromised skin [9,17]. Its principal procedural caveat is architectural distortion: all margins and anatomic landmarks must be carefully marked before tumescence [17]. Key practice recommendations across these domains are summarized in table 5.
Conclusion
In summary, when local anesthetic choice, dose, and technique are matched to vascular reserve, barrier integrity, and host pharmacokinetics, even traditionally high-risk dermatologic scenarios can be managed with very low rates of serious harm. The main threats arise not from routine use but from predictable amplifiers such as severe vasculopathy, extensive barrier loss, compressed cumulative dosing, and unrecognized drug interactions. This shift from dogma to risk-stratified utilization heightens rather than relaxes the obligation for preparedness: rigorous dose calculation and documentation, systematic medication review, context-sensitive selection of agent and route, and office-level readiness with phentolamine and 20 percent lipid emulsion rescue supported by checklists and team training.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mc Namara CT, Greyson M, Digital ischemia after lidocaine with epinephrine injection in a patient with primary Raynaud’s phenomena. Case Reports Plast Surg Hand Surg 9 (2022): 193–196.36082186 10.1080/23320885.2022.2117702 PMC 9448404 · doi ↗ · pubmed ↗
- 2Saskia MS, Franziska CG, Alexander S, Use of local anesthetics with an epinephrine additive on fingers and penis - dogma and reality. J Dtsch Dermatol Ges 19 (2021): 185–196.
- 3Lalonde D Minimally invasive anesthesia in wide awake hand surgery. Hand Clin 30 (2014): 1–6.24286736 10.1016/j.hcl.2013.08.015 · doi ↗ · pubmed ↗
- 4Brofeldt BT, Doherty D, Batra K, Topical lidocaine in the treatment of partial-thickness burns. J Burn Care Rehabil 10 (1989): 63–68.2921260 10.1097/00004630-198901000-00009 · doi ↗ · pubmed ↗
- 5Stymne B, Lillieborg S. Plasma concentrations of lignocaine and prilocaine after a 24-h application of analgesic cream (EMLA) to leg ulcers. Br J Dermatol 145 (2001): 530–534.11703277 10.1046/j.1365-2133.2001.04408.x · doi ↗ · pubmed ↗
- 6Figueiredo PC, Glaysson TT. Safety of local anesthetics. An Bras Dermatol 95 (2020): 82–90.31952994 10.1016/j.abd.2019.09.025PMC 7058875 · doi ↗ · pubmed ↗
- 7Maria AS, Ioannis F, Vasileios Z. Pharmacological Interactions of Epinephrine at Concentrations Used in Dental Anesthesiology: An Updated Narrative Review. Reports 8 (2025): 224.41283592 10.3390/reports 8040224 PMC 12643428 · doi ↗ · pubmed ↗
- 8Ngcobo NN. Silent Dangers in Elderly Pharmacotherapy: The Interplay of Polypharmacy, Multimorbidity, and Drug Interactions. J Eval Clin Pract 31 (2025): e 70283.41025835 10.1111/jep.70283 PMC 12482850 · doi ↗ · pubmed ↗