The interaction between lifestyle and blood pressure on Stroke: A cross-sectional study from Northern China
Jiantao Yu, Qiang Zhou, Yanyan Zhao, Haiying Chen, Huiyong Yu, Yuying Li, Xiuguo Zhang

TL;DR
This study shows that high blood pressure and unhealthy lifestyles together increase stroke risk in older adults in northern China.
Contribution
The study identifies synergistic effects between elevated blood pressure and unhealthy lifestyles on stroke risk in older adults.
Findings
Elevated systolic and diastolic blood pressure are significantly linked to higher stroke incidence.
Unhealthy lifestyle factors and high blood pressure synergistically increase stroke risk.
Smoking partially mediates the relationship between diastolic blood pressure and stroke.
Abstract
This study aimed to explore and quantify the extent of interaction between lifestyle factors and systolic and diastolic blood pressure on stroke among adults over 65 years of age. This investigation sought to provide valuable insights into the multifactorial risk factors for stroke, with the ultimate goal of supporting clinicians in implementing more focused and comprehensive preventive strategies. Data were obtained from the 2019 health examination records of community hospitals in northern China. A stratified cluster random sampling method was used to select a representative sample from resident health records within the essential public health service management system. Participants were categorized into four subgroups based on systolic and diastolic blood pressure levels. Odds ratios (ORs) with 95% confidence intervals (CIs) and trend tests were used to examine the association…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
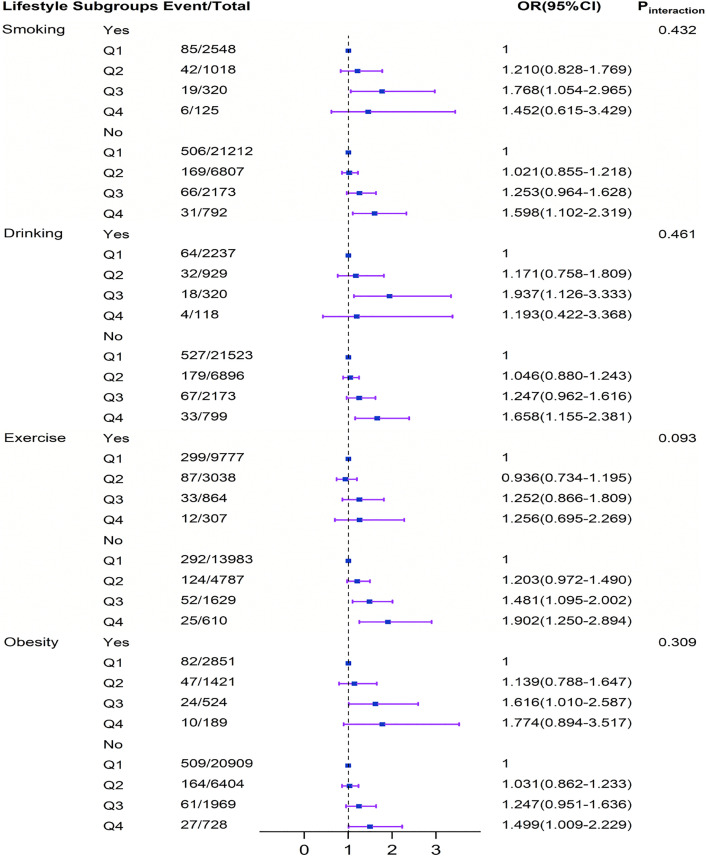 Fig 1
Fig 1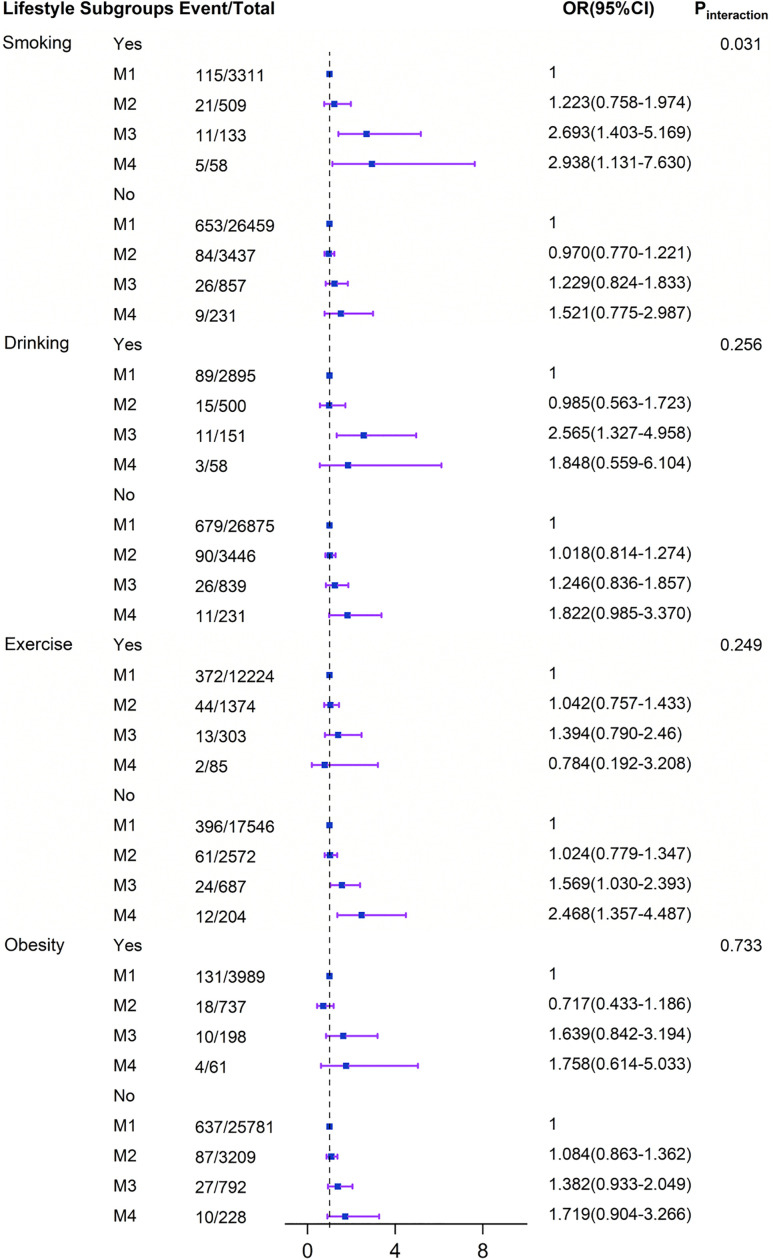 Fig 2
Fig 2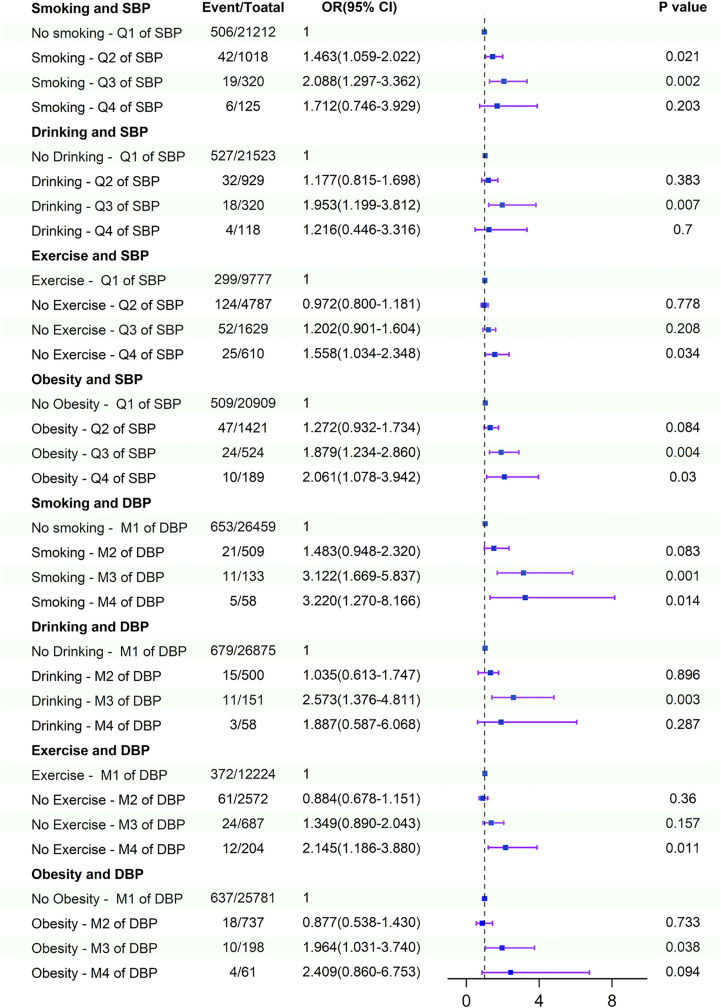 Fig 3
Fig 3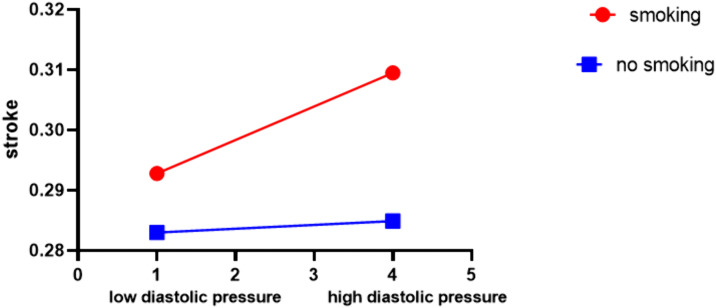 Fig 4
Fig 4- —http://dx.doi.org/10.13039/100017959Health Commission of Hebei Province
- —http://dx.doi.org/10.13039/100017959Health Commission of Hebei Province
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAcute Ischemic Stroke Management · Blood Pressure and Hypertension Studies · Dementia and Cognitive Impairment Research
Introduction
Stroke is a group of cerebrovascular diseases characterized by acute brain tissue injury resulting from the sudden rupture or obstruction of cerebral blood vessels. It is associated with high morbidity, high mortality, and high disability rates, placing a substantial economic burden on patients and their families. As a major global health issue, stroke ranks as the third-leading cause of both death and disability worldwide [1]. According to the latest Global Burden of Disease Study (GBD), the lifetime risk of stroke in China is 39.9% [2], the highest in the world, and is increasing at an annual rate of 8.3% [3]. Therefore, the prevention and treatment of stroke represent an urgent public health challenge that requires immediate attention.
The etiology of stroke is complex and influenced by a combination of individual, genetic, behavioral, and environmental factors [2,4–6]. Understanding its multifactorial nature is essential for enhancing prevention and treatment strategies. Findings from the “INTERSTROKE” study across 32 countries indicated that modifiable risk factors—including hypertension, dyslipidemia, obesity, smoking, and alcohol consumption—accounted for 90.7% of the population-attributable risk of stroke [7]. Among these, hypertension remains one of the most significant modifiable risk factors and is globally prevalent. Epidemiological data show that approximately 73.91% of stroke patients have comorbid hypertension [6]. A synthesis of 61 prospective observational studies worldwide (involving approximately one million individuals aged 40–89 years) demonstrated a continuous, independent, and direct positive association between clinic-measured systolic blood pressure (SBP) and diastolic blood pressure (DBP) and stroke-related mortality. For blood pressure levels ranging from 115/75 mmHg to 185/115 mmHg, each increase of 20 mmHg in SBP or 10 mmHg in DBP was associated with a doubling of the risk of cardiovascular and cerebrovascular events [8]. However, the effects of systolic and diastolic blood pressure on stroke risk among older adults remain controversial. A study by Miura et al. conducted among middle-aged and elderly individuals in Japan reported a positive correlation between both SBP and DBP and stroke risk [9]. In contrast, Makino et al. found that in hypertensive patients over 70 years of age, stroke risk was not associated with elevated systolic blood pressure [10]. Some studies have even suggested that lower blood pressure may increase stroke risk, possibly due to reduced cerebral perfusion leading to hypoperfusion and hypoxia, which could subsequently contribute to incident stroke [11].
However, in recent years, a growing number of researchers have focused on the significant role of modifiable factors, particularly lifestyle, in reducing the risk of stroke. The American Heart Association/American Stroke Association (AHA/ASA) has issued guidelines for the secondary prevention of stroke, which advocate for health-promoting behaviors such as reducing cigarette and alcohol consumption and increasing physical activity. These recommendations aim to decrease stroke-related morbidity and mortality among stroke survivors by controlling risk factors and encouraging the adoption of healthy behaviors [12].
Although existing research has extensively examined the individual associations between hypertension and lifestyle with stroke, a significant gap remains regarding their interactive or joint effects on stroke risk. Furthermore, the underlying mechanisms are not fully understood, and current studies lack robust causal inferences pertaining to the combined influence of lifestyle and blood pressure on stroke. There is a clear need to investigate the interaction between these factors. Such research would enhance our understanding of stroke etiology, improve risk stratification, and potentially contribute to the development of updated treatment guidelines that account for multiple interacting risk factors. This study aims to provide valuable insights into the multifactorial risk profile of stroke, with the ultimate goal of supporting clinicians in delivering more targeted and comprehensive preventive interventions.
Methods
Research object and data source
To promote comprehensive health, the Chinese Ministry of Health established primary healthcare institutions to provide free health management services—including annual health examinations for adults aged 65 and older—and to create electronic health records for this population. This retrospective cross-sectional study was conducted within the framework of this long-term chronic disease management project for older adults in northern China. We utilized data collected during the screening period from February to September 2019. A stratified cluster random sampling method was employed to obtain a representative sample from the resident health records within the Essential Public Health Service Management System. All participants provided written informed consent allowing the use of their medical records for research purposes. All data were fully anonymized prior to access and analysis.
The study design and sampling procedure were conducted as follows. Participants were selected from all 11 cities within a province in northern China. In the first stage, two subdistricts or townships from both urban and rural areas were selected from each city using probability proportional to size sampling, based on the population of each subdistrict/township. In the second stage, two additional subdistricts were chosen from the previously selected districts by simple random sampling. Finally, two community hospitals were randomly selected from each subdistrict. All residents aged 65 years or older who voluntarily participated in the health examination at the selected community hospitals were included in the study. The inclusion criteria were: (1) age ≥ 65 years, and (2) residency in the target county or district for more than six months. The exclusion criteria included: (1) hearing impairment or inability to communicate normally. (2) inability to cooperate due to cognitive impairment or mental illness. A total of 39,179 individuals aged over 65 years from the selected communities were initially enrolled. After excluding participants with missing values in the lifestyle survey, 34,995 individuals were included in the final analysis, yielding a response rate of 89.32%. All covariates with complete data were incorporated into the study.
General study questionnaire
An interview-based survey was conducted by trained staff using a standardized questionnaire. Sociodemographic data were collected, including sex, age, occupation (laborer, peasant, or leadership), educational level (college graduate, high school graduate, or below high school), marital status (married, never married, or widowed/divorced), medical insurance status, family history of stroke, and medical history (including atrial fibrillation, hypertension, and diabetes mellitus). Lifestyle information was obtained through self-reporting via a structured questionnaire, covering details such as smoking habits, alcohol consumption, and physical activity. Smoking status was categorized into three groups: never smoker, former smoker, and current smoker. Current smokers were defined as those who smoked at least one cigarette per day for a minimum of six months. Drinkers were defined as individuals who consumed at least 30 mL of alcohol per week for one year or longer. Non-exercisers were identified as participants who had not engaged in leisure-time or recreational physical activity for at least one year, and who had not performed medium or heavy manual labor during that period. It should be noted that transport-related physical activity was not assessed in this survey.
Anthropometric tests and laboratory examinations
Qualified medical professionals conducted physical and laboratory examinations. Participants were instructed to remove their shoes and wear lightweight clothing for the measurement of weight and height. An automatic sphygmomanometer was used to measure blood pressure (BP). Measurements were performed twice in a quiet environment, with participants resting for at least 10 minutes between each measurement. If the difference between the two readings exceeded 5 mmHg, a third measurement was taken, and the mean of all measurements was calculated as the final blood pressure value. Fasting blood samples were collected in the morning after an overnight fast. These samples were used to assess fasting blood glucose (FBG), triglycerides (TG), total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), and high-density lipoprotein cholesterol (HDL-C). Additionally, imaging examinations included abdominal color ultrasound, chest radiography, and electrocardiography.
Ascertainment of Stroke
The identification of stroke cases in this study was based on a combination of self-reported medical history and neurologist assessment, in accordance with World Health Organization criteria. Additional information regarding symptoms, date of onset, diagnostic units, medical records, and imaging data were collected to validate the initial diagnosis. Stroke was defined as an event comprising subarachnoid hemorrhage, intracerebral hemorrhage, or cerebral ischemic necrosis. Cases of secondary stroke due to transient cerebral ischemia, brain tumor, metastatic brain tumor, or trauma were excluded.
Definition of independent variables
Hypertension was diagnosed in patients with systolic blood pressure (SBP) ≥140 mmHg or diastolic blood pressure (DBP) ≥90 mmHg in the absence of antihypertensive medication, as well as in those with a documented history of hypertension who were receiving antihypertensive treatment, irrespective of current blood pressure measurements [13]. According to the evidence-based guidelines for adult hypertension in China, hypertension was classified into four categories [14]: Normotension (SBP < 140 mmHg and DBP < 90 mmHg), Grade 1 hypertension (SBP 140–159 mmHg and/or DBP 90–99 mmHg), Grade 2 hypertension (SBP 160–179 mmHg and/or DBP 100–109 mmHg), and Grade 3 hypertension (SBP ≥ 180 mmHg and/or DBP ≥ 110 mmHg). Based on these criteria, SBP and DBP were each divided into four groups: Q1 (SBP ≤ 139 mmHg), Q2 (SBP 140–159 mmHg), Q3 (SBP 160–179 mmHg), Q4 (SBP ≥ 180 mmHg); M1 (DBP ≤ 89 mmHg), M2 (DBP 90–99 mmHg), M3 (DBP 100–109 mmHg), M4 (DBP ≥ 110 mmHg). Diabetes mellitus was defined as fasting blood glucose (FBG) ≥7.0 mmol/L and/or the use of hypoglycemic medication or a previous diagnosis of diabetes [15]. Hyperlipidemia was defined as total cholesterol (TC) ≥6.2 mmol/L, low-density lipoprotein cholesterol (LDL-C) ≥4.1 mmol/L, triglycerides (TG) ≥2.3 mmol/L, or high-density lipoprotein cholesterol (HDL-C) <1.0 mmol/L [16]. Atrial fibrillation was identified based on self-reported history or findings from on-site electrocardiogram examinations. Body mass index (BMI) was calculated as weight in kilograms divided by the square of height in meters. Overweight was defined as BMI between 24.0 and 27.9 kg/m², and obesity as BMI ≥ 28.0 kg/m² [17].
Statistical analysis
All statistical analyses were performed using SPSS 26.0 (IBM SPSS Statistics for Windows, Version 26.0. Armonk, NY: IBM Corp). A two-sided P value <0.05 was considered statistically significant. Descriptive analyses were conducted across blood pressure groups. Categorical variables are expressed as numbers and percentages. Three logistic regression models were fitted to estimate odds ratios (ORs) and their corresponding 95% confidence intervals (CIs) for the association between blood pressure and stroke. Trend tests were performed using the median value of each systolic blood pressure (SBP) and diastolic blood pressure (DBP) group. Subgroup analyses were carried out to evaluate the effects of both continuous and categorical SBP and DBP on stroke incidence across various lifestyle subgroups, including obesity (yes/no), smoking (yes/no), drinking (yes/no), and exercise (yes/no). Multiplicative interaction terms within logistic regression models were used to examine the interaction effects between lifestyle factors and different SBP/DBP groups on stroke.
Statement of Ethics
The research complied with the ethical guidelines outlined in the Declaration of Helsinki and received approval from the Ethics Committee of The Hebei Medical University Third Affiliated Hospital China. All participants are informed about the study and written informed consent. Furthermore, all collected data are kept confidential and anonymous.
Results
General characteristics of study subjects
A total of 34,995 individuals were included in the analysis, comprising 44.3% males (n = 15,484) and 55.7% females (n = 19,511). The age range was 65–103 years, with a mean age of 71.91 ± 5.65 years. Among the participants, 924 (2.6%) were identified as stroke patients. Hypertension was the most prevalent chronic condition, affecting 58.4% of participants, followed by hyperlipidemia (31.4%), diabetes (23.3%), and fatty liver (21.3%). Unhealthy lifestyle factors included smoking (11.5%), alcohol consumption (10.3%), obesity (14.1%), and physical inactivity (60.0%) (Supplementary File, S1 Table).
Association of systolic and diastolic blood pressure with Stroke
Tables 1 and 2 present the associations between SBP and DBP(both as continuous and categorical variables) and the incidence of stroke. After adjusting for confounding factors (including sex, age, occupation, marital status, education level, medical insurance, atrial fibrillation, family history of stroke, diabetes mellitus, dyslipidemia, and fatty liver), logistic regression analysis indicated that higher levels of SBP and DBP were associated with an increased incidence of stroke. Both systolic and diastolic blood pressure showed a positive correlation with stroke incidence, and these associations were linear (Ptrend for SBP = 0.001; Ptrend for DBP = 0.001). Compared with the Q1 group of SBP, the adjusted odds ratios (ORs) with 95% confidence intervals (CIs) for the Q2–Q4 groups were 1.086 (0.926–1.274), 1.384 (1.098–1.744), and 1.648 (1.175–2.313), respectively. Compared with the M1 group of DBP, the adjusted ORs (95% CIs) for the M2–M4 groups were 0.69 (0.53–0.88), 0.52 (0.39–0.70), and 0.42 (0.30–0.58), respectively. When analyzed as continuous variables, each 1 mmHg increase in SBP and DBP was associated with a multivariable-adjusted odds ratio for stroke of OR = 1.008 (95% CI: 1.004–1.012) and OR = 1.012 (95% CI: 1.005–1.019), respectively.
Table 1: Multivariate-adjusted Odds ratios (95% confidence intervals) of estimated SBP for Stroke.
Table 2: Multivariate-adjusted Odds ratios (95% confidence intervals) of estimated DBP for Stroke.
Interaction effects between systolic and diastolic pressure and lifestyle on stroke
Stratified analyses were conducted to evaluate whether the associations between elevated systolic and diastolic blood pressure (analyzed both as continuous and categorical variables) and the incidence of stroke were modified by predefined lifestyle subgroups. The relationship between increased systolic and diastolic blood pressure and stroke incidence remained consistent with the primary results across most subgroups (Table 3; Figs 1–2). In subgroup analyses, a significant positive association between SBP and stroke incidence was observed across various lifestyle categories, including smokers, non-smokers, non-drinkers, physically inactive individuals, and those with or without obesity (all Ptrend < 0.05; see Supplementary S3 Table). Similarly, a significant positive association between DBP and stroke incidence was confirmed in subgroups such as smokers, drinkers, physically inactive individuals, and non-obese participants (all Ptrend < 0.05; see Supplementary S2 Table).
Table 3: Subgroup analysis of the association between estimated Systolic and diastolic blood pressure and Stroke.
Subgroup and interaction analyses among the group Q1 − 4 of SBP and Stroke across various lifestyle subgroups.The multiplicative interaction model of Logistic regression is used to explore the impact of the interaction between lifestyle and different groups of SBP with Stroke. All models were adjusted for sex, age, occupation, marital status, education level, medical insurance, atrial fibrillation, family history of stroke, diabetes, dyslipidemia, and fatty liver. CI, confidence interval; OR, odds ratio; SBP, systole blood pressure. Q1: SBP ≤ 139 mmHg, Q2: 140 ≤ SBP ≤ 159 mmHg, Q3: 160 ≤ SBP ≤ 179 mmHg, Q4: SBP ≥ 180 mmHg.
Subgroup and interaction analyses among the group M 1 − 4 of DBP and Stroke across various lifestyle subgroups.The multiplicative interaction model of Logistic regression is used to explore the impact of the interaction between lifestyle and different groups of DBP with Stroke. All models were adjusted for sex, age, occupation, marital status, education level, medical insurance, atrial fibrillation, family history of stroke, diabetes, dyslipidemia, and fatty liver. CI, confidence interval; DBP, diastolic blood pressure; OR, oddsratio; M1: DBP ≤ 89 mmHg, M2: 90 ≤ DBP ≤ 99 mmHg, M3: 100 ≤ DBP ≤ 109 mmHg, M4: DBP ≥ 110 mmHg.
Interaction and joint effects analyses of elevated SBP and DBP and unhealthy lifestyle factors on stroke indicated that unhealthy behaviors and higher blood pressure levels synergistically increased the incidence of stroke after adjusting for confounding factors. Compared with non-smokers with SBP < 140 mmHg or DBP < 90 mmHg, smokers with SBP 140–159 mmHg, 160–179 mmHg, or DBP 100–109 mmHg and ≥110 mmHg had increased stroke incidence by 46%,108%, and 212%, 222%, respectively. Compared with non-drinkers with SBP < 140 mmHg or DBP < 90 mmHg, drinkers with SBP 160–179 mmHg or DBP 100–109 mmHg showed increased stroke incidence by 95% and 157%, respectively. Compared with non-obese individuals with SBP < 140 mmHg or DBP < 90 mmHg, obese participants with SBP 160–179 mmHg, ≥ 180 mmHg, or DBP 100–109 mmHg had increased stroke incidence by 88%, 106%, and 96%, respectively. Compared with physically active individuals with SBP < 140 mmHg or DBP < 90 mmHg, those who were physically inactive with SBP ≥ 180 mmHg or DBP ≥ 110 mmHg exhibited increased stroke incidence by 56% and 115%, respectively (Fig 3).
Interaction and joint effects for exposures to higher SBP and DBP and unhealthy lifestyle on Stroke.All models were adjusted for sex, age, occupation, marital status, education level, medical insurance, atrial fibrillation, family history of stroke, diabetes, dyslipidemia, and fatty liver. Q1 of SBP: SBP ≤ 139 mmHg, Q2 of SBP: 140 ≤ SBP ≤ 159 mmHg, Q3 of SBP: 160 ≤ SBP ≤ 179 mmHg, Q4 of SBP: SBP ≥ 180 mmHg; M1 of DBP: DBP ≤ 89 mmHg, M2 of DBP: 90 ≤ DBP ≤ 99 mmHg, M3 of DBP: 100 ≤ DBP ≤ 109 mmHg, M4 of DBP: DBP ≥ 110 mmHg. CI, confidence interval; OR, odds ratio; SBP, systole blood pressure; DBP, diastolic blood pressure.
No significant interactions between systolic blood pressure and stroke incidence were observed across the lifestyle subgroups (P for interaction >0.05)(Figs 1–2). In contrast, the association between diastolic blood pressure and stroke was modified significantly only by smoking status (P for interaction = 0.031). Simple effect analysis further revealed a stronger positive association between DBP and stroke among smokers compared to non-smokers (Fig 4).
Modulating effect of smoking on diastolic blood pressure.Models were adjusted for sex, age, occupation, marital status, education level, medical insurance, atrial fibrillation, family history of stroke, diabetes, dyslipidemia, and fatty liver.
Discussion
This study examined the joint predictive value of SBP, DBP, and lifestyle on incident stroke among adults aged over 65 in northern China. The main findings can be summarized as follows: (1) Based on blood pressure group analyses, higher SBP and DBP were significantly associated with an increased incidence of stroke. This association exhibited a linear trend and remained consistent across most lifestyle subgroups. (2) Unhealthy lifestyle factors synergistically interacted with elevated SBP and DBP levels to further increase the incidence of stroke among older adults. (3) The predictive effect of DBP on stroke incidence was modified by smoking status, indicating a stronger positive association between DBP and stroke among smokers compared to non-smokers.
Among the various risk factors contributing to stroke, hypertension remains a well-established modifiable element, with a global prevalence that warrants significant attention [18]. Our study identified a positive association between blood pressure and the incidence of stroke among adults over 65 years of age. This association remained consistent across subgroups with different lifestyle factors, including smoking, alcohol consumption, physical inactivity, and obesity. These findings align with previous research. For instance, Perry et al. reported that both systolic blood pressure (SBP) and diastolic blood pressure (DBP), whether considered individually or in combination, are independently, continuously, and positively associated with an increased risk of stroke [19]. Similarly, Lewington et al. demonstrated that stroke risk increases linearly once blood pressure levels exceed 115/75 mmHg [8].
Previous studies have also examined the relationship between blood pressure and stroke incidence using stratified analyses, though differences exist in both blood pressure categorization and study populations compared to our research [20]. For example, a survey conducted among elderly Ghanaians calculated incident stroke over an 18-month follow-up using three blood pressure cut-offs: < 120/80 mmHg, 120–159/80–99 mmHg, and ≥160/100 mmHg. This study found that a lower blood pressure target of <120/80 mmHg was associated with a signal of reduced incident stroke [21]. However, although lowering blood pressure generally decreases stroke risk in a linear manner within the general population, a J-shaped relationship has been observed in individuals with diabetes [20,22]. Elevated systolic and diastolic blood pressure can contribute to cerebrovascular diseases through mechanisms such as atherosclerotic plaque formation, smooth muscle cell remodeling, reduced cerebral blood flow, and arterial baroreflex dysfunction [23,24]. Effective antihypertensive treatment has been shown to reduce both the incidence and recurrence risk of stroke [23]. Therefore, active management of blood pressure in hypertensive patients is of considerable importance for stroke risk reduction.
Although the 2017 AHA/ACC guidelines lowered the diagnostic threshold for hypertension from ≥140/90 mmHg to ≥130/80 mmHg in the general population, the 2014 evidence-based guidelines for hypertension in adults have continued to be widely adopted in China [25]. In accordance with these Chinese guidelines, we categorized and analyzed the relationship between systolic and diastolic blood pressure and stroke. This classification approach has also been employed in other similar studies [26,27]. The use of this grouping method provides a valuable reference for future hierarchical management of hypertension. Furthermore, exploring the association between systolic and diastolic blood pressure and stroke based on this classification system offers practical insights for risk-stratified management of hypertension and stroke prevention strategies.
The findings of this study provide substantial evidence for a synergistic effect between lifestyle factors and elevated systolic and diastolic blood pressure on incident stroke. Both unhealthy lifestyles and increased blood pressure are well-established risk factors for stroke, and their individual associations with stroke have been extensively documented [28–34]. This study further demonstrates that when these factors coexist, their combined impact on stroke risk exceeds the sum of their individual effects. This insight suggests that a coordinated strategy targeting both types of risk factors could yield additional benefits in stroke prevention.
The mechanism underlying the interaction between lifestyle and blood pressure in relation to stroke is complex. First, elevated blood pressure is directly associated with an increased risk of stroke. Second, lifestyle factors may exert specific regulatory effects on blood pressure [35–37]. For example, alcohol consumption can raise blood pressure through activation of the sympathetic nervous system [36], and is positively correlated with hypertension risk. The adverse effects of alcohol on blood pressure may also directly increase the risk of hemorrhagic stroke [38]. The relationship between obesity and blood pressure is nearly linear [39], and obesity-related hypertension can further elevate stroke risk. Cigarette smoking, whether active or passive, significantly impairs endothelial function and increases the risk of atherosclerotic disease and hypertension [40]. Furthermore, interventions such as physical activity have been shown to mitigate these effects. For instance, a study of 50 participants with treatment-resistant hypertension reported that 8–12 weeks of aerobic exercise reduced daytime systolic and diastolic ambulatory blood pressure by 5.9 mmHg and 3.3 mmHg, respectively [41]. Thus, unhealthy lifestyles may elevate stroke risk partly through their impact on increasing blood pressure.
In our study, drinkers with elevated SBP and DBP showed a significantly increased incidence of stroke. This finding is consistent with a Korean cohort study, which demonstrated through combined risk analysis that alcohol consumption poses a greater danger for individuals with severe hypertension [38]. Therefore, controlling alcohol intake is particularly important among patients with severe hypertension. However, a prospective population-based cohort study conducted in China indicated that hypertension is an independent risk factor for stroke, while alcohol consumption was not significantly associated in their model [42]. Some studies have even suggested that moderate alcohol consumption may be associated with a reduced risk of ischemic stroke. Proposed mechanisms for such protective effects include cardioprotective properties, antithrombotic effects, and stress reduction [43,44]. The extent to which alcohol-induced hypertension contributes to stroke risk, and the underlying mechanisms, remain incompletely understood. Some evidence suggests that alcohol-related hypertension may involve catecholamine activity and genetically influenced inactivation pathways [45]. Heavy alcohol consumption may elevate blood pressure through activation of the sympathetic nervous system, a mechanism whose sensitivity may be genetically modulated. For instance, the methyl-adenosine phosphorylase rs10118757 G allele has been observed to modify the risk of ischemic stroke related to alcohol-induced hypertension [46]. These findings highlight the potential essential role of genetic factors in alcohol-induced hypertension and associated stroke.
Previous studies have indicated that the effect of physical exercise on blood pressure is influenced by the baseline blood pressure level of the patients. In individuals with stage II and III hypertension, physical exercise may partially substitute for pharmacological therapy by contributing to blood pressure reduction and improving circulatory function [37,47,48]. In contrast, among patients with mild hypertension, the antihypertensive effect of physical exercise has not been consistently significant [49]. Exercise can attenuate the activity of the renin-angiotensin system—a hormone system that promotes vasoconstriction and elevates blood pressure. It has also been shown to enhance endothelial function, which is critical for maintaining vascular tone and stable blood pressure levels [50,51]. Alternatively, the association between physical activity and reduced stroke risk may be attributed to non-blood-pressure-related effects, such as improvements in insulin sensitivity, lipid metabolism, endothelial function, and immune regulation [52].
Obesity is a significant risk factor for hypertension. The Framingham Study, one of the most influential cohort studies, reported that the prevalence of hypertension among obese individuals is twice that of non-obese individuals [53]. The Trials of Hypertension Prevention (TOHP) study demonstrated that for every 2 kg of weight loss, systolic and diastolic blood pressure decreased by 3.7 mmHg and 2.7 mmHg, respectively [54]. Additionally, body mass index (BMI) has been consistently shown to be positively correlated with stroke risk [55]. Animal experiments conducted by Osmond et al. revealed structural remodeling of the middle cerebral artery in obese rats, which exhibited more severe brain damage following cerebral ischemia compared to non-obese controls [56]. These cerebrovascular alterations are associated with the development of hypertension and suggest that elevated blood pressure may be a key mediator of stroke risk in obese individuals. Extensive studies have indicated that obesity, particularly visceral adipose tissue, substantially contributes to increased blood pressure [57]. The mechanisms underlying obesity-related hypertension are multifactorial and include sodium retention, insulin resistance, activation of the renin-angiotensin-aldosterone system, altered vascular function, and dysregulation of adipokine secretion [58,59]. Visceral fat plays a particularly critical role in activating these pathways. These insights underscore the potential benefit of a coordinated approach targeting both obesity and hypertension for enhanced stroke prevention.
A key finding of our study is the significant interaction between smoking status and diastolic blood pressure (DBP) in predicting stroke incidence. This interaction indicates a critical synergistic effect, in which the combined influence of smoking and elevated DBP on stroke risk exceeds the sum of their individual effects [60]. Further analysis confirmed that the positive association between DBP and stroke is substantially stronger among smokers than among non-smokers.
Smoking, a well-established independent risk factor for stroke, adversely affects vascular health through multiple mechanisms, including endothelial dysfunction, accelerated atherosclerosis, increased blood viscosity, and prothrombotic states [61–64]. Elevated DBP, on the other hand, contributes to chronic vascular stress, impairs microvascular perfusion, and increases the risk of cerebral small vessel disease [65–68]—each of which represents a key pathway in stroke pathogenesis. Our findings suggest that these two factors may act synergistically to amplify stroke risk: smoking may intensify the vascular damage associated with elevated DBP, or high DBP may exacerbate the prothrombotic and atherosclerotic effects of smoking. This mutual reinforcement could explain why the association between DBP and stroke is magnified among smokers, underscoring the importance of evaluating their combined impact in clinical risk assessment [5]. Notably, this interaction was specific to DBP, as no significant interactions were observed between systolic blood pressure (SBP) and smoking or other lifestyle factors in our analyses. This divergence raises important questions regarding the distinct roles of SBP and DBP in stroke pathogenesis, particularly under the influence of smoking. While SBP is widely regarded as a primary driver of macrovascular events, DBP may play a more critical role in microvascular injury—a process potentially aggravated by smoking-related endothelial damage. This specificity warrants further investigation to elucidate the underlying physiological mechanisms.
From a clinical perspective, our findings highlight the need for tailored risk management strategies. The significant interaction between smoking and DBP identifies a high-risk subgroup—smokers with elevated DBP—for whom targeted interventions could substantially reduce stroke incidence. These results enhance our understanding of how lifestyle factors and physiological markers interact to shape cardiovascular risk, with important implications for clinical practice and public health policy.
Limitation
The strengths of this study include its large sample size (n = 34,995) and the examination of interactive effects between systolic and diastolic blood pressure and lifestyle factors on stroke. However, several limitations should be acknowledged. First, due to the observational design, causality cannot be established, and the possibility of reverse causality cannot be excluded. Second, although our models adjusted for numerous covariates, residual confounding from unmeasured variables—such as diet, sleep quality, and inflammatory markers—may still remain, a challenge common to observational studies. Third, lifestyle factors were self-reported via a structured questionnaire, which may introduce recall bias and potential misclassification. Additionally, due to limitations in the questionnaire design, only leisure-time/recreational and occupational physical activity were assessed; transport-related physical activity was not evaluated. Thus, the findings should be interpreted with caution within these constraints. Finally, the study population was drawn from a single province in northern China. While this sample may be partially representative of the broader northern Chinese population, it does not fully capture the region’s diversity. Therefore, further validation through multi-regional, population-based longitudinal studies involving more diverse demographics is warranted.
Conclusion
The observed synergistic effect between blood pressure (systolic and diastolic) and lifestyle factors, along with the interaction effect of lifestyle in the blood pressure–stroke relationship, has important implications for stroke prevention and management. First, primary prevention strategies should emphasize reducing unhealthy lifestyle behaviors and controlling hypertension. Second, healthcare providers should assess both traditional risk factors and the interaction between blood pressure and lifestyle when evaluating stroke risk. Hypertension patients, in particular, require intensified lifestyle management. Integrating blood pressure and lifestyle profiles into existing risk assessment tools could improve risk stratification and help identify high-risk individuals for early intervention. Third, these findings underscore the value of individualized treatment. Clinicians should collaborate with patients to develop personalized plans that combine pharmacological treatments with lifestyle modifications tailored to specific risk profiles.
Supporting information
S1 TableClinical characteristics of person according to the specified Systolic and diastolic pressure categories.(DOCX)
S2 TableSubgroup analyses among the group M1 − 4 of DBP and Stroke across various lifestyle subgroups.(DOCX)
S3 TableSubgroup analyses among the group Q1 − 4 of SBP and Stroke across various lifestyle subgroups.(DOCX)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Pu L, Wang L, Zhang R, Zhao T, Jiang Y, Han L. Projected global trends in ischemic stroke incidence, deaths and disability-adjusted life years from 2020 to 2030. Stroke. 2023;54(5):1330–9. doi: 10.1161/STROKEAHA.122.040073 37094034 · doi ↗ · pubmed ↗
- 2GBD 2016 Lifetime Risk of Stroke Collaborators, Feigin VL, Nguyen G, Cercy K, Johnson CO, Alam T, et al. Global, Regional, and Country-Specific Lifetime Risks of Stroke, 1990 and 2016. N Engl J Med. 2018;379(25):2429–37. doi: 10.1056/NEJ Moa 1804492 30575491 PMC 6247346 · doi ↗ · pubmed ↗
- 3Wang W, Jiang B, Sun H, Ru X, Sun D, Wang L, et al. Prevalence, incidence, and mortality of stroke in china: results from a nationwide population-based survey of 480 687 adults. Circulation. 2017;135(8):759–71. doi: 10.1161/CIRCULATIONAHA.116.025250 28052979 · doi ↗ · pubmed ↗
- 4Chen J, Zhu Q, Yu L, Li Y, Jia S, Zhang J. Stroke risk factors of stroke patients in China: A Nationwide Community-Based Cross-Sectional Study. Int J Environ Res Public Health. 2022;19(8):4807. doi: 10.3390/ijerph 19084807 35457673 PMC 9030671 · doi ↗ · pubmed ↗
- 5Lee SM, Oh C-M, Kim M-H, Ha E, Hong M, Ryoo J-H. Current smoking status as a predictor of cerebral infarction in men: a retrospective cohort study in South Korea. BMJ Open. 2021;11(4):e 042317. doi: 10.1136/bmjopen-2020-042317 33853795 PMC 8054067 · doi ↗ · pubmed ↗
- 6Setyopranoto I, Bayuangga HF, Panggabean AS, Alifaningdyah S, Lazuardi L, Dewi FST, et al. Prevalence of stroke and associated risk factors in sleman district of yogyakarta special region, Indonesia. Stroke Res Treat. 2019;2019:2642458. doi: 10.1155/2019/2642458 31186829 PMC 6521526 · doi ↗ · pubmed ↗
- 7O’Donnell MJ, Chin SL, Rangarajan S, Xavier D, Liu L, Zhang H, et al. Global and regional effects of potentially modifiable risk factors associated with acute stroke in 32 countries (INTERSTROKE): a case-control study. Lancet. 2016;388(10046):761–75. doi: 10.1016/S 0140-6736(16)30506-2 27431356 · doi ↗ · pubmed ↗
- 8Lewington S, Clarke R, Qizilbash N, Peto R, Collins R, Prospective Studies Collaboration. Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet. 2002;360(9349):1903–13. doi: 10.1016/s 0140-6736(02)11911-8 12493255 · doi ↗ · pubmed ↗