Development of the Alcohol Use Disorders Identification Test-Consumption (AUDIT-C) Score as a Predictor of Alcohol Withdrawal Syndrome in Trauma Patients at a Community Level 1 Trauma Center
Melinda Bottenfield, Karleigh Curfman, Shirin Siddiqi, Thomas Simunich, Avi Robinson, Russell Dumire, Shawna Morrissey

TL;DR
This study shows that the AUDIT-C score can effectively predict alcohol withdrawal syndrome in trauma patients, helping guide treatment decisions.
Contribution
The study introduces a validated AUDIT-C threshold for predicting AWS in trauma patients with moderate alcohol use.
Findings
AUDIT-C scores ≥ 5 predicted AWS with 90% sensitivity and 96.2% specificity.
An AUDIT-C threshold of ≥ 5 was identified using logistic regression and ROC analysis.
The study population included 662 trauma patients, mostly geriatric and female.
Abstract
Background and objective The Clinical Institute Withdrawal Assessment for Alcohol-Revised (CIWA-Ar) is an assessment tool that guides symptom-triggered therapy (STT) in alcohol withdrawal syndrome (AWS) patients. Institutionally, CIWA-Ar is used for STT when patients admit to daily alcohol use or arrive intoxicated. Given the lack of validated screening tools for predicting AWS, we hypothesized that CIWA-Ar and STT were used inefficiently, causing poor resource stewardship and overtreatment. Our current protocol is to complete the Alcohol Use Disorders Identification Test-Consumption (AUDIT-C), an evidence-based screening tool for hazardous alcohol use. Given this protocol and the absence of verified screening tools for alcohol withdrawal prediction, we aimed to analyze AUDIT-C efficacy in predicting AWS to guide STT. Methods A retrospective review was performed of admission AUDIT-C…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
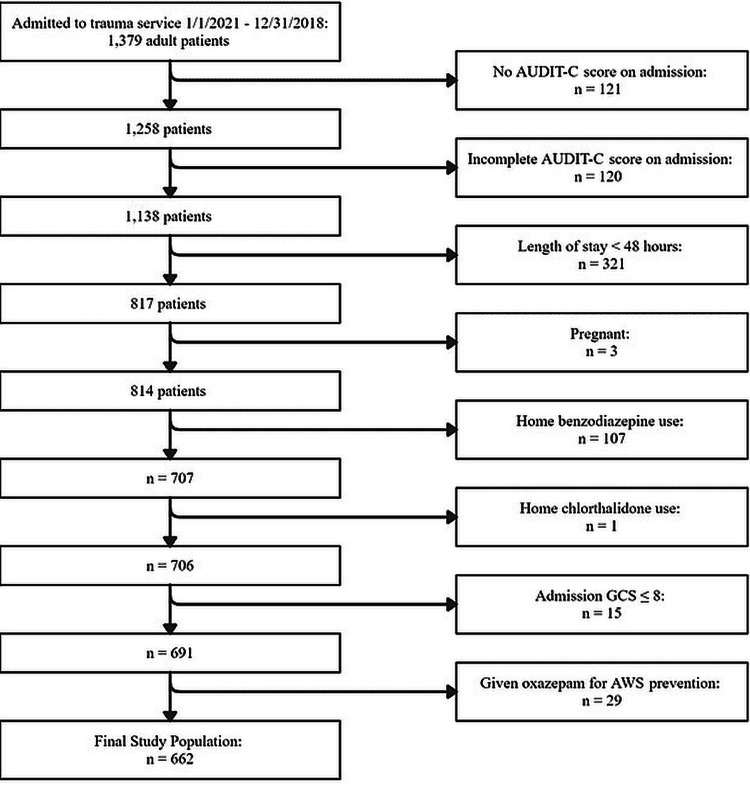 Figure 1
Figure 1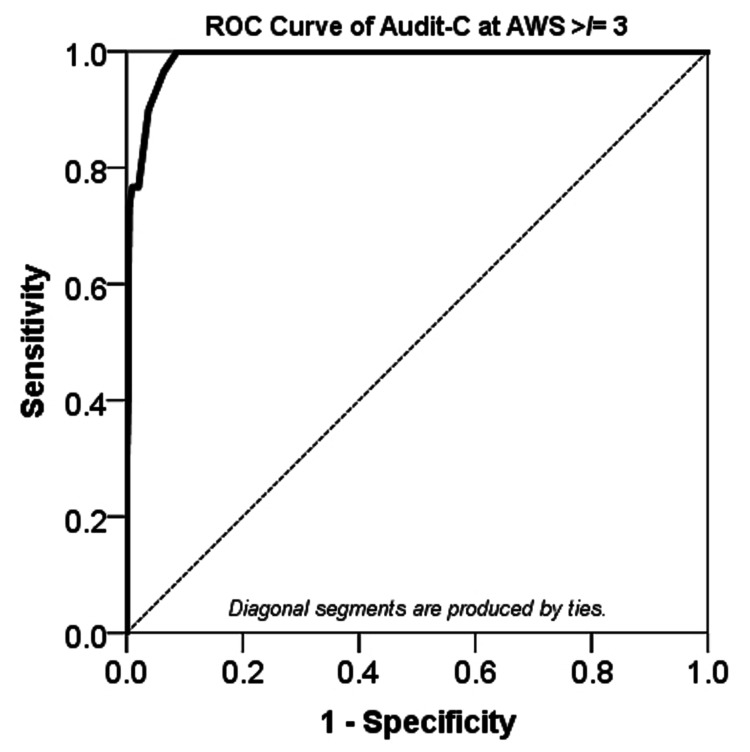 Figure 2
Figure 2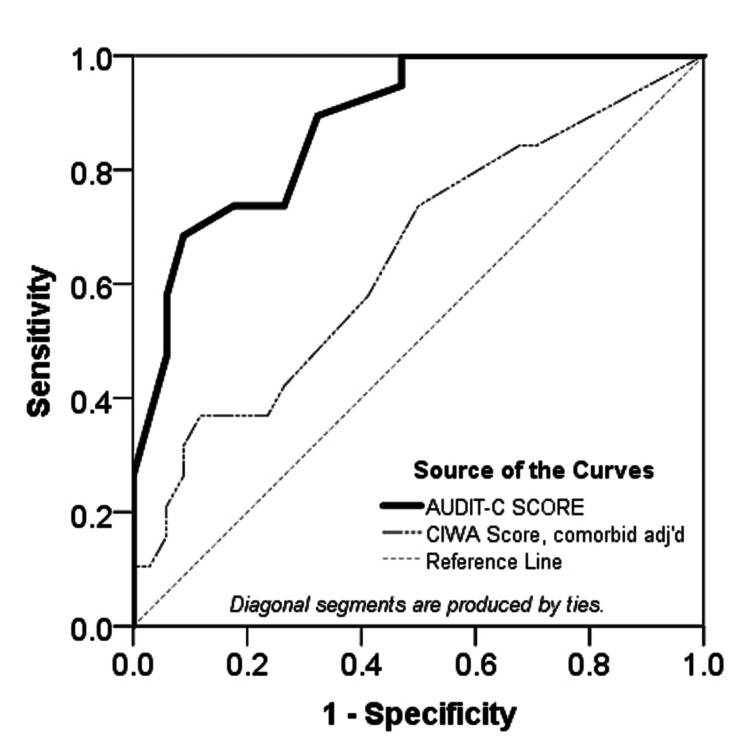 Figure 3
Figure 3| Criteria | Explanation of use | ||
| A. History of alcohol use: | |||
| A-1 | BAC > 0.08 | U.S. legal criteria for alcohol intoxication | |
| A-2 | AUDIT-C Score ≥ 3 (female) and ≥ 4 (male) | Definition of hazardous drinking use | |
| B. Each item counted as 1 point: | |||
| B-1 | AUDIT-C: frequency of drinking score = 4 | Equivalent to daily alcohol use | |
| B-2 | AUDIT-C: # of drinks at a time score > 1 | Equivalent to 3-4+ drinks at a time | |
| B-3 | AUDIT-C: frequency of 6+ drinks in one sitting score > 2 | Equivalent to weekly binge-drinking | |
| B-4 | CIWA-Ar Score > 10 | Reflective of complex AWS | |
| B-5 | Benzodiazepine given during admission | Surrogate for anxiety, agitation, or insomnia | |
| B-6 | Soft limb restraints used | Surrogate for severe agitation | |
| B-7 | GCS score < 15; | Surrogate for confusion | |
| --- | If dementia or Parkinson’s disease, the criterion is lowered to GCS < 14 | ||
| B-8 | Heart rate (HR) > 109 beats per minute (bpm) | Symptoms reflective of the autonomic hyperactivity seen in alcohol withdrawal syndrome | |
| B-9 | Systolic blood pressure (SBP) > 179 mmHg | ||
| B-10 | Respiratory rate (RR) > 24 breaths per minute (BRPM) | ||
| B-11 | Temperature (T) > 38.3 °C | ||
| Item B-4 was adjusted for comorbid conditions likely to confound scoring, e.g., dementia, Parkinson's disease, anxiety, seizure disorders | |||
| Scoring (0-12) | |||
| Both Part A and Part B must meet or exceed the individual scoring threshold for that part in order to proceed to the calculation of an alcohol withdrawal syndrome score. | |||
| Part A threshold: | |||
| Either item A-1 or A-2 must be true | |||
| Part B threshold: | |||
| 11 items, each scored as 1 point | |||
| If both elements of Part A are true, add 1 point to the Part B score before comparing the Part B sum to its threshold | |||
| When the Part B score is ≥ 3, the threshold for this part has been met | |||
| When the thresholds for both Parts A & B have been met, the AWS score is calculated as: 1 + the sum of Part B | |||
| An AWS score ≥ 3 is associated with alcohol withdrawal syndrome symptomology | |||
| An AWS score ≤ 2 implies that the symptoms are unlikely to be caused by alcohol withdrawal syndrome | |||
| Characteristics | Total study population | Subgroup of population with AUDIT-C ≥ 5 |
| (n = 662) | (n = 51) | |
| Mean age, years (range) | 70.6 (18-106) | 52.0 (19-81) |
| Women, n (%) | 395 (59.6) | 12 (23.5) |
| Men, n (%) | 267 (40.4) | 39 (76.7) |
| Use of restraints, n (%) | 51 (7.7) | 8 (15.7) |
| Anxiety/sleep disorder, n (%) | 47 (7.1) | 7 (13.7) |
| Dementia, n (%) | 43 (6.5) | 0 |
| Admission BAC > 0.08, n (%) | 33 (5.0) | 24 (47.1) |
| Benzodiazepines given, n (%) | 20 (3.0) | 9 (17.6) |
| Seizure disorder, n (%) | 20 (3.0) | 1 (2.0) |
| Parkinson’s disease, n (%) | 12 (1.8) | 0 |
| AUDIT-C Score | Portion of Total Study Population per Each Possible Audit-C Score | Portion of Total Study Population per Audit-C Score of 0, (1-5, inclusive), (5-12, inclusive) |
| 0 | 495 (74.7) | 495 (74.5) |
| 1 | 60 (9.1) | 116 (17.5) |
| 2 | 22 (3.3) | |
| 3 | 15 (2.3) | |
| 4 | 19 (2.9) | |
| 5 | 15 (2.3) | 51 (7.7) |
| 6 | 7 (1.1) | |
| 7 | 4 (0.6) | |
| 8 | 5 (0.7) | |
| 9 | 5 (0.7) | |
| 10 | 7 (1.1) | |
| 11 | 3 (0.5) | |
| 12 | 5 (0.7) |
| AWS defined as an AWS score ≥ 3 | Estimated value | 95% confidence interval | |
| Prevalence | 4.5% | 3.1% – 6.5% | |
| Sensitivity | 90.0% | 72.3% – 97.4% | |
| Specificity | 96.2% | 94.3% – 97.5% | |
| Positive predictive value (PPV) | 52.9% | 38.6% – 66.8% | |
| Negative predictive value (NPV) | 99.5% | 98.4% – 99.9% | |
| Likelihood ratio (LR), if AUDIT-C score | ≥ 5 | 1.13 | 0.76 – 1.66 |
| < 5 | 0.005 | 0.0016 – 0.015 | |
| Note: Likelihood ratios weighted by prevalence | |||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAlcoholism and Thiamine Deficiency · Substance Abuse Treatment and Outcomes · Fibromyalgia and Chronic Fatigue Syndrome Research
Introduction
Alcohol use and abuse are extremely prevalent problems in current society, for which approximately 48% to 50% of trauma patients are found to be at risk for hazardous drinking habits or have evidence of an alcohol use disorder (AUD) [1-3]. Nearly 50% of trauma patients are found to have detectable serum levels of alcohol upon hospital admission [4], with 10% of those experiencing a readmission within one year to the same hospital for a new traumatic injury [4]. Although documentation of AUD is robust in trauma patients, the rates of developing alcohol withdrawal syndrome (AWS) in this population, fortunately, remain low (0.8% to 0.9%) [1,5]. Despite the low rate, AWS remains a prime topic of interest in trauma research due to its risk of significant morbidities and possible effects on future related traumatic events. Several published studies have documented an association between trauma patients with AWS and an increased length of hospital stay, higher readmission rates, more frequent need for mechanical ventilation, and diagnosis of pneumonia [1,6,7]. Interestingly, AWS symptoms have also been found to be more pronounced and of longer duration in geriatric patients, increasing their delirium risk [8-10].
Despite the significant prevalence of alcohol use in adult trauma patients, an obvious lack of validated AWS screening tools persists [11]. Instead, various methods, such as patient admission blood alcohol concentration (BAC) or reports of hazardous habits on screenings, have been haphazardly used to place patients on Clinical Institute Withdrawal Assessment for Alcohol-Revised (CIWA-Ar) protocols to guide symptom-triggered therapy (STT). The CIWA-Ar is a 10-question assessment applied to those at moderate risk for alcohol withdrawal and validated for AWS symptom identification and classification of severity [12,13]. It is not copyrighted and may be reproduced freely.
For CIWA-Ar to be used effectively, patients must first be screened for increased risk of AWS [14], which represents a major application flaw, as currently there are no applicable evidence-based screening tools validated in the prediction of alcohol withdrawal. For this reason, there is concern that CIWA-Ar protocols are potentially being misused, which can lead to the overuse of recommended sedatives in STT [14,15]. One study at the Mayo Clinic revealed that only 48% of admitted patients were appropriately assessed and correctly placed on CIWA-Ar [14]. This is especially concerning in both trauma and elderly patients who are inherently predisposed to hospital delirium, medication-induced over-sedation, and respiratory depression [16].
The 10-question Alcohol Use Disorders Test (AUDIT) has been validated for the accurate detection of hazardous alcohol use in patient populations [17-19]. This assessment has been further abbreviated into three surveys: AUDIT-Consumption (C), AUDIT-Dependence (D), and AUDIT-Picinelli (P) (see Appendix A). The AUDIT-C survey is composed of the first three questions of the AUDIT questionnaire, which assess the quantity and frequency of alcohol consumption [20,21]. Next, the AUDIT-D is comprised of the three subsequent elements, which determine the degree of alcohol dependence. Finally, the AUDIT-P represents the remaining four constituents, assessing for psychosocial problems related to alcohol use. Generally, the higher the score, the more likely it is that a person's drinking is affecting his or her safety. However, the AUDIT questionnaire has not been validated in the prediction of AWS. The AUDIT-C/D/P is available for use in the public domain.
Several studies have been published that analyze these different components of the AUDIT questionnaire and their clinical application. For example, four individual studies demonstrated that a higher AUDIT-C score is reflective of severe alcohol misuse and was associated with an increased risk of trauma-related hospitalizations, fractures, and postoperative complications [22-25]. Literature published by Pecoraro et al. studied the application of AUDIT-PC, a combination of AUDIT-P and AUDIT-C, in the prediction of alcohol withdrawal in hospitalized patients. This report demonstrated that an admission AUDIT-PC score ≥ 4 was associated with 91.0% sensitivity and 89.7% specificity for AWS and could be used as a reliable tool in withdrawal prediction [11]. Given their success in validating the use of AUDIT-PC for AWS prediction in hospitalized patients, we decided to perform a similar study at our institution. Of note, the Pecoraro et al. [11] study was not performed specifically with an increased-risk trauma population, nor did it individually evaluate the AUDIT-C and AUDIT-P components of the AUDIT-PC score.
Our study evaluated the use of AUDIT-C alone in predicting AWS in hospitalized adult trauma patients. Despite other resources, like the Christiana Care study [26], which evaluated different AUDIT components or combinations thereof, the AUDIT-C was specifically used in our study for several reasons. First, as previously described, a higher AUDIT-C score suggests severe alcohol use, which is associated with an increased risk for trauma-related medical care and complications; therefore, we felt that the AUDIT-C would be most applicable to a trauma patient-focused study [22-25]. Next, per the guidelines of the American College of Surgery Verification Review Committee for level 1 trauma center accreditation, routine screening for hazardous alcohol use is a requirement [27]. As such, the AUDIT-C as a screening tool had been implemented at our institution before the commencement of this study and was available for retrospective review. Finally, the brevity of the AUDIT-C, containing only three questions as opposed to the 10-question AUDIT or the seven-question AUDIT-PC, lends itself to efficient screening in busy emergency departments [17].
Additional studies have demonstrated that independently, a higher AUDIT-C score is reflective of severe alcohol misuse and was associated with an increased risk of trauma-related hospitalizations, fractures, and postoperative complications [22-25]. Therefore, we hypothesized that the AUDIT-C specifically would be significantly predictive of AWS in hospitalized trauma patients. Additionally, we expected this to be associated with a discrete AUDIT-C score that would inform more appropriate application of CIWA-Ar and STT protocols. Finally, as this study aimed to fill a previously identified void in validated and reliable tools predictive of inpatient development of AWS, we predicted that insights gained from assessing our application of the AUDIT-C would reveal opportunities for more selective use of alcohol withdrawal protocols.
This work was previously presented virtually as an abstract and as a poster at the American Association for the Surgery of Trauma conference in 2020.
Materials and methods
This study was approved by the Institutional Review Board (IRB) of the Conemaugh Memorial Medical Center (approval no. 19-25). This retrospective cohort analysis included adult patients (age ≥ 18 years) admitted to the trauma service at a community level 1 trauma center from January 1, 2018, through December 31, 2018, regardless of traumatic mechanism or injury (n = 1,379).
Patients were excluded for the following reasons: length of stay < 48 hours (n = 321), lack of documented complete AUDIT-C score on admission (n = 256, which includes 15 cases in which the clinical state was unclear, pregnancy (n = 3), home benzodiazepine use (n = 107), home chlorthalidone use (n = 1), and patients given oxazepam as a fixed dose taper to prevent AWS during their hospitalization (n = 29). After exclusions, the final study population consisted of 662 patients (Figure 1).
Study population exclusion processThe data presented represent patient counts.AUDIT-C: Alcohol Use Disorders Identification Test-Consumption, AWS: Alcohol withdrawal syndrome
Data was extracted from both the electronic medical record (EMR) and trauma database. Values at admission for Glasgow Coma Scale score (GCS), vital signs, blood alcohol content (BAC), and AUDIT-C scores (total and individual components) were collected. Additionally, documented alcohol use, CIWA-Ar score, inpatient administration of benzodiazepines (lorazepam, diazepam, or oxazepam), use of soft-limb restraints, and hospital length of stay were obtained. Patient history, specifically home medications as listed in the EMR at admission, was used to identify comorbidities that could potentially confound AWS determination, including anxiety, dementia, seizure disorders, and Parkinson’s disease.
Defining alcohol withdrawal syndrome via novel AWS score
Given the absence of a documented diagnosis of AWS in the EMR and that most patients were not placed on our institution’s CIWA-Ar protocol for AWS identification, a generalized method based on the collected patient data was retrospectively devised to identify AWS or the risk for its occurrence. The AWS Score was formed from the Diagnostic & Statistical Manual of Mental Disorders (DSM)-V criteria for the diagnosis of AWS [28], known risk factors of AWS and/or symptoms reflective of the autonomic hyperactivity seen in AWS, insights from CIWA-Ar methodology, and AUDIT-C scoring that implies 'moderate' alcohol use. As complete documentation of all factors contained within the DSM-V proved to be elusive, use of the DSM-V AWS definition alone was not feasible. As with the DSM-V AWS criteria, our study AWS score was based upon the patient having exhibited a history of 'moderate' alcohol use [28]. However, the DSM-V criteria do not specify the quantity or duration of alcohol use that would be considered moderate. Therefore, we defined 'moderate' alcohol use as an admission BAC of greater than 0.08%, the legal limit for intoxication in the United States of America [29], and/or an admission AUDIT-C (see Appendix A) of greater than or equal to three (female) and four (male), which defines 'hazardous drinking use' [20,30]. The AUDIT-C is available for use in the public domain.
Initially, our AWS score included sub-scores of CIWA-Ar. However, as most patients in this study were not placed on CIWA-Ar protocol (n = 609) and, as such, were not regularly assessed for CIWA-Ar-monitored symptoms such as tremors, insomnia, anxiety, or hallucinations, the inclusion of CIWA-Ar subscores was abandoned. Additionally, the incorporation of CIWA-Ar sub-scores allowed for too much selection bias towards patients on CIWA-Ar protocols. Despite these difficulties, a total CIWA-Ar score greater than 10 was used as an AWS score component since that is reflective of complex alcohol withdrawal (see Appendix B) [12,13]. The CIWA-Ar is not copyrighted and may be reproduced freely. As CIWA-Ar monitored symptomology was lacking, surrogate variables were needed. To that end, the necessity of limb restraints was chosen as a surrogate marker for agitation, as soft limb restraints were often used in patients showing signs of severe agitation and jeopardizing the safety of themselves and others. Furthermore, the use of benzodiazepines in naïve patients was used as a surrogate for anxiety, agitation, or insomnia.
A GCS score of less than 15 was used to reflect confusion. To reduce confounding by the concomitant presence of dementia or Parkinson’s disease, where the patient may function at a lower baseline GCS, the score threshold was lowered to less than 14. Abnormal vital signs that reflected autonomic hyperactivity consistent with an increased risk of AWS were also included [12]. Minimal values were set at a higher-than-normal threshold for our study to minimize secondarily inflated scores in patients who may have experienced abnormal vital signs due to pain and trauma.
To ensure that a higher AWS score was associated with heavier alcohol use, the component questions of the AUDIT-C score were also included [20]. The threshold score of the first question, assessing frequency of drinking, was set to 4 as a reflection of daily alcohol use. The threshold score of the second question, quantity of drinking, was set to greater than 1, correlating with consuming more than four drinks in one sitting. Finally, the third question, analyzing the frequency of binge drinking (defined as 6 or more drinks in one sitting), was given a threshold of 2 or greater, consistent with binge drinking at least two to three times per week.
Both AWS scores and documented CIWA-Ar scores were adjusted for patient comorbidities to minimize potential score inflation and confounders. Parkinson’s disease (patients prescribed carbidopa-levodopa with or without entacapone) nullified CIWA-Ar sub-scores of confusion and tremors. Dementia (designated in our study as patients prescribed donepezil or memantine) nullified CIWA-Ar sub-scores of confusion. Seizure disorders (patients prescribed divalproex, temazepam, carbamazepine, or phenobarbital) nullified CIWA-Ar sub-scores of tremors. Anxiety/sleep disorders (patients prescribed quetiapine, melatonin, or haloperidol) nullified CIWA-Ar sub-scores of anxiety. Our AWS scoring system is detailed in Table 1.
Statistical analysis
The AWS score was confirmed using binary logistic regression and receiver-operating characteristic curve (ROC) analyses. For this study, AWS was defined as an AWS score ≥ 3 in the setting of documented/known moderate alcohol use. The SPSS Statistics version 24 was used to conduct the statistical analyses (IBM Corp., Armonk, NY, USA). The overall type I error (alpha) was set at 0.05.
Results
Of the 662 patients admitted to the trauma service between January 1, 2018, and December 31, 2018, who met selection criteria, 30 (4.5%) patients experienced alcohol withdrawal, as defined by an AWS score of ≥ 3. The population in this study was found to be predominantly female (59.6%) with a mean age of 70.6 years old. Further demographic information regarding the study population can be seen in Table 2. The frequency distribution of AUDIT-C scores is detailed in Table 3.
By defining alcohol withdrawal syndrome as an AWS score of ≥ 3, an ROC analysis revealed that AUDIT-C scores of 5 or greater were predictive of AWS development (Figure 2). The area under the ROC curve was 0.989 (95% CI (0.980, 0.997), p < 0.0005), which is considered outstanding discrimination according to Hosmer et al. [31].
The ROC analysis of AUDIT-C scores using AWS score ≥ 3 to define alcohol withdrawal syndromeArea under the ROC = 0.989 (95% CI (0.980, 0.997), p < 0.0005); A p-value < 0.05 was considered statistically significantROC: Receiver-operating characteristic curve, AUDIT-C: Alcohol Use Disorders Identification Test-Consumption
A binomial logistic regression was performed to ascertain the predictive value of the AUDIT-C score on the likelihood of a patient developing AWS. Linearity of the AUDIT-C variable with respect to the logit of the dependent variable was assessed via the Box-Tidwell (1962) procedure [32]. Based on this assessment, the AUDIT-C variable was found to be linearly related to the logit of the dependent variable (p = 0.549). Nine standardized residuals with a value > 2.600 standard deviations were identified and retained in the analysis. The logistic regression model was statistically significant, χ2(1) = 172.371, P < 0.0005. The model explained 74.3% (Nagelkerke R2) of the variance for AWS greater than or equal to three and correctly classified 98.3% of cases. The AUDIT-C was a statistically significant predictor (p < 0.0005) for AWS. For every unit increase in AUDIT-C score, the odds of having AWS increase by a factor of 2.4. For AWS, defined as an AWS score ≥ 3, an Audit-C score ≥ 5 yields a 90.0% sensitivity, a 96.2% specificity, a positive predictive value of 52.9%, and a negative predictive value of 99.5%, using the observed prevalence of 4.5% (Table 4).
Interestingly, when CIWA-Ar scores were compared with AUDIT-C scores after adjusting for patient comorbidities, the AUDIT-C assessment outperformed CIWA-Ar in predicting AWS (Figure 3).
ROC analysis of AUDIT-C score vs CIWA-Ar score in predicting AWS as defined by AWS score ≥ 3Note: The sample size for this analysis of the CIWA-Ar score is 53; Audit-C: 0.881 (95% CI (0.791, 0.971), p < 0.0005); CIWA-Ar adjusted for comorbidities: 0.646 (95% CI (0.488, 0.803), p = 0.081); A p-value < 0.05. was considered statistically significantROC: Receiver-operating characteristic curve, AUDIT-C: Alcohol Use Disorders Identification Test-Consumption, AWS: Alcohol withdrawal syndrome
In fact, adjusted CIWA-Ar scores and AUDIT-C scores were negatively correlated, Kendall's tau b = -0.203, p = 0.049. Furthermore, our data revealed that length of stay (LOS) was not statistically associated with or affected by AUDIT-C (Spearman's rho = -.023, p = 0.562), CIWA-Ar (Spearman's rho = 0.199, p = 0.153), or adjusted CIWA-Ar (Spearman's rho = 0.179, p = 0.199); and it was only very mildly correlated with the study AWS score (Spearman's rho = 0.143, p < 0.0005). The overall mean (range) LOS was 5.0 days (two to 40), and the mean (range) LOS for the subgroup with an AUDIT-C ≥ 5 was 4.6 days (two to 12).
To provide clinicians a guide for more objective utilization of alcohol withdrawal protocols, an AUDIT-C threshold of 5 was identified by combining the binary logistic regression and ROC analyses results. As hypothesized, 48 patients (7.3%) were suboptimally managed regarding AWS and use of the CIWA-Ar protocol when this AUDIT-C threshold score was applied. Of those with AUDIT-C scores ≥ 5 (n = 51), 23 (45%) patients were not placed on CIWA-Ar for AWS prevention. This group represents the number of those in our study at risk for under/delayed treatment for AWS. Conversely, of the patients with an AUDIT-C score < 5 (n = 611), 25 patients (4.1%) were placed on CIWA-Ar without harboring a history of moderate alcohol use. This group represents the number of patients in our study at risk for over-sedation or overtreatment due to inappropriate CIWA-Ar use.
Discussion
As a community institution that is witnessing an increase in geriatric trauma admissions, along with rising alcohol use in the general population, it is important to acknowledge that the reported prevalence of AUD amongst geriatric emergency room evaluations is roughly 10% to 15% [8,16]. Our data were consistent with the reported range of AUD prevalence, as 12% of the study population was found to have moderate alcohol use (n = 78).
Though 78 patients were identified as at risk, only 30 patients were recognized to have undergone AWS, defined as an AWS score of ≥ 3. However, 51 patients scored ≥ 5 on the AUDIT-C scale. As 51 patients at risk for AWS were identified, but only 30 experienced it clinically, this may suggest that an AUDIT-C score of ≥ 5 is too conservative. The ROC and visual cluster analysis were used in deciding on an AUDIT-C cutoff value that balanced optimization of sensitivity and specificity while prioritizing a higher false positive rate over a false negative rate. An increase in the false negative rate would have equated to missed or delayed diagnosis of AWS, which, per the literature, has been associated with increased LOS, higher costs, and higher morbidity and mortality rates [1,6,7].
Of the 25 patients who had AUDIT-C scores < 5 but were placed on the CIWA-Ar protocol, only one patient appeared to have developed AWS and required benzodiazepine treatment, with no significant effect on this patient’s length of stay, overall health, or medical care. In fact, as detailed in the results section, our data revealed that length of stay was not statistically associated with or affected by AUDIT-C, CIWA-Ar, or adjusted CIWA-Ar; however, LOS did show a very mild statistically significant correlation with the study AWS score.
Due to the limited population that experienced AWS, it is difficult to analyze this subgroup for statistically significant complications. For example, of the 23 patients with an AUDIT-C score ≥ 5 who were not placed on CIWA-Ar, two patients received benzodiazepines for agitation (based on clinician judgement). One patient had a history of recent heavy alcohol use, but the other had no documented alcohol history. Subsequent research will be focused on including patients with moderate or heavy alcohol use and excluding patients who do not drink alcohol regularly, as their risk for AWS is low. Another way to improve upon this research is to exclude patients with severe traumatic brain injuries. This injury complex may confound results, as this patient population has been observed clinically at this institution to require benzodiazepines and restraints due to their increased agitation and confusion.
There are several limitations of this study. First, although our study included a large patient population of 662 patients, most patients had an admission AUDIT-C score of 0 and had zero risk factors for the development of AWS (n = 495). These patients outnumbered the population of patients who had significant AUDIT-C scores and were at risk for developing AWS (n = 51) (Table 2). Though the proportion of patients that developed AWS in our study was comparable to the rates reported in current literature, this study was limited to only a single year of data. In future research endeavors, we intend to increase study duration to capture a larger study population and, in turn, increase the potential number of patients that would develop AWS.
The diagnosis of AWS was inconsistently documented in the EMR, making it difficult to retrospectively decide who experienced AWS. This may have contributed to the finding of 24 patients having had an AUDIT-C score > 5, yet their AWS score did not support a determination of alcohol withdrawal. As previously described, we developed an AWS score to define AWS for this study. In subsequent studies, AWS will be defined even more clearly with the inclusion of AWS-related diagnosis codes. Lastly, since the AUDIT-C questionnaire is a survey, it requires honest and accurate self-reporting by patients regarding their alcohol use. Although most patients appeared to have answered honestly, as later reflected by their development (or lack) of AWS, several patients with an AUDIT-C score of 0 (n = 10) had CIWA-Ar scores reflective of AWS and were placed on the CIWA-Ar protocol, suggestive of incongruity with self-reporting. This can improperly categorize patients and may contribute to the decreased sensitivity seen in this study.
Conclusions
The statistically significant and clinically meaningful findings of this study support the assertion that an AUDIT-C score of 5 or greater is predictive of AWS development in hospitalized trauma patients with a history of moderate alcohol use. Though we have provided evidence of its significance, this tool is not without flaws. Since our study population was primarily geriatric, further research is needed to determine if these findings are truly generalizable to non-geriatric trauma patients. For this reason, we encourage a combination of AUDIT-C and clinical assessment when making decisions regarding the use of withdrawal protocols and STT.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Alcohol withdrawal syndrome in admitted trauma patients Am J Surg Jawa RS Stothert JC Shostrom VK 78178720820142506296710.1016/j.amjsurg.2014.04.007 · doi ↗ · pubmed ↗
- 2A controlled trial of brief intervention versus brief advice for at-risk drinking trauma center patients J Trauma Soderstrom CA Di Clemente CC Dischinger PC Hebel JR Mc Duff DR Auman KM Kufera JA 110211126220071749570810.1097/TA.0b 013e 31804 bdb 26 · doi ↗ · pubmed ↗
- 3The prevalence and effect of alcohol and drug abuse on cohort-matched critically injured patients Am Surg Cornwell EE 3rd Belzberg H Velmahos G 461465641998 https://pubmed.ncbi.nlm.nih.gov/9585786/9585786 · pubmed ↗
- 4Screening for at-risk drinking behavior in trauma patients J Am Osteopath Assoc Plackett TP Ton-That HH Mueller J Grimley KM Kovacs EJ Esposito TJ 37638211520152602433110.7556/jaoa.2015.078 · doi ↗ · pubmed ↗
- 5Occurrence, predictors, and prognosis of alcohol withdrawal syndrome and delirium tremens following traumatic injury Crit Care Med Salottolo K Mc Guire E Mains CW van Doorn EC Bar-Or D 8678744520172826693710.1097/CCM.0000000000002371 · doi ↗ · pubmed ↗
- 6The effect of acute alcohol intoxication and chronic alcohol abuse on outcome from trauma JAMA Jurkovich GJ Rivara FP Gurney JG Fligner C Ries R Mueller BA Copass M 51562701993 https://pubmed.ncbi.nlm.nih.gov/8510296/8510296 · pubmed ↗
- 7The effects of alcohol abuse on readmission for trauma JAMA Rivara FP Koepsell TD Jurkovich GJ Gurney JG Soderberg R 1962196427019938105114 · pubmed ↗
- 8The prevalence of positive drug and alcohol screens in elderly trauma patients Subst Abus Ekeh AP Parikh PP Walusimbi M Woods RJ Hawk A Mc Carthy MC 51553520142458829310.1080/08897077.2013.797539 · doi ↗ · pubmed ↗