Understanding influences of care-seeking behaviours for diarrhoeal illnesses: a qualitative meta-synthesis
Marissa H Miller, Skye M Hilbert, Erica N Rosser, Laura Sinko, Elizabeth C Lee, Kirsten E Wiens

TL;DR
This study explores why people seek care for diarrhoeal illnesses, identifying key factors like sociocultural beliefs and access barriers that influence their decisions.
Contribution
The paper provides a novel thematic framework from qualitative research on care-seeking behaviors for diarrhoea, emphasizing sociocultural and structural influences.
Findings
Sociocultural norms and beliefs about disease causation significantly influence care-seeking decisions.
Barriers such as travel distance, cost, and lack of trust in healthcare providers delay care.
Perceived severity of illness is a strong motivator for seeking care outside the home.
Abstract
Diarrhoeal illnesses remain a leading cause of morbidity and mortality worldwide. Understanding when and where individuals seek healthcare is essential for accurately assessing disease burden and improving access to appropriate care. We conducted a meta-synthesis of qualitative research examining barriers and facilitators to care-seeking for diarrhoeal illness among individuals and caregivers of children. We systematically reviewed qualitative studies examining the motivations for seeking care for diarrhoeal illness and conducted a thematic analysis to synthesise findings across studies. PubMed, Embase, Web of Science and Global Index Medicus were searched through 3 September 2024. We included qualitative studies that used interviews and/or focus group discussions to examine care-seeking decisions for diarrhoeal illness. Two independent reviewers assessed studies for eligibility,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
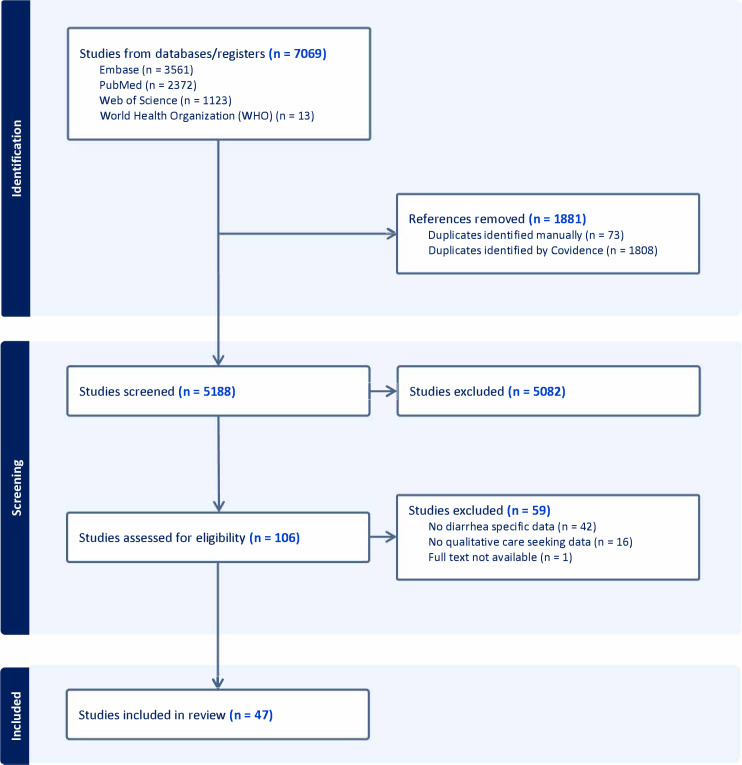 Figure 1
Figure 1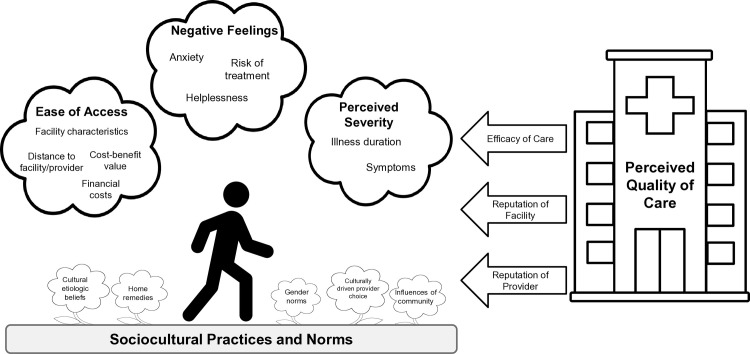 Figure 2
Figure 2| Theme | Subthemes | Papers with theme | Total |
|---|---|---|---|
| Sociocultural | Cultural aetiologic beliefs |
| 25 |
| Influence of the community |
| 20 | |
| Gender norms |
| 8 | |
| Culturally driven provider choice |
| 15 | |
| Awareness of home remedies |
| 29 | |
| Perceived severity | Illness duration |
| 12 |
| Symptoms |
| 23 | |
| Negative feelings | Feeling anxious |
| 24 |
| Feeling helpless |
| 11 | |
| Risk posed by treatment |
| 9 | |
| Ease of access | Financial costs |
| 25 |
| Distance to provider |
| 20 | |
| Cost-benefit value |
| 8 | |
| Facility characteristics |
| 10 | |
| Perceived quality of care | Efficacy of medication |
| 17 |
| Reputation of the facility |
| 13 | |
| Reputation of the provider |
| 22 |
- —http://dx.doi.org/10.13039/100000060National Institute of Allergy and Infectious Diseases
- —http://dx.doi.org/10.13039/100000865Bill and Melinda Gates Foundation
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsViral gastroenteritis research and epidemiology · Child Nutrition and Water Access · Inflammatory Bowel Disease
Introduction
Diarrhoeal diseases were associated with an estimated 4.7 billion incident cases and 1.2 million deaths in 2021.1 Many of these cases and deaths could have been averted through access to clean water, vaccination, proper nutrition and appropriate case management and treatment.2 3 Appropriate diarrhoeal treatment may involve rehydration, either intravenously or orally through oral rehydration solutions, zinc supplementation and/or use of antibiotics.4 While oral diarrhoea treatments are effective and generally inexpensive, they often require seeking care outside the home at a health post, pharmacy, hospital or clinic. Care-seeking at a public hospital or clinic is also required for cases to be reported to health systems and counted in estimates of diarrhoea burden, which are used to distribute limited diarrhoea mitigation resources such as vaccines. Cases reported to the health surveillance systems are typically used to assess disease trends and detect disease outbreaks in passive surveillance systems. Thus, understanding care-seeking behaviour for diarrhoea is important for improving access to treatment, estimating diarrhoea burden and preventing cases and deaths.
To better understand how many community diarrhoea cases go unreported and possibly untreated, we previously conducted a systematic review and meta-analysis of studies that reported the proportion of individuals or caregivers who seek care when they or their child have diarrhoeal illness.5 We found substantial variation across the 166 quantitative studies identified from 62 countries for inclusion in the proportion of people who sought medical care, with estimates ranging from nearly 0% to 100% depending on the study context. The only factor that was consistently associated with this variation in care-seeking was diarrhoea case definition, with care-seeking significantly higher for severe diarrhoea or cholera compared with general diarrhoea. However, given the wide variation in the data reported in the 166 studies, we were not able to identify other common reasons that people do or do not seek care.
Secondary analyses of individual-level care-seeking survey data have found that education, healthcare knowledge and experience, wealth, gender roles and autonomy in decision-making are all associated with variation in care-seeking for diarrhoeal illness.610 A limitation of these studies and the systematic review is that they used survey data collected with pre-specified questionnaires and did not have the flexibility to examine nuanced reasons why individuals do or do not seek care. This limits our ability to understand what can be done to improve access to care, especially for hard-to-reach populations that are systematically not captured by surveillance due to low interaction with the healthcare system. Qualitative studies that employ open-ended questionnaires and semistructured interviews provide an opportunity to address this gap.
In this study, we synthesised information from qualitative studies to identify common themes and reasons that individuals or caregivers do not seek care at medical facilities when they or their child have diarrhoea. Only three studies, all conducted in Canada, were conducted in high-income countries, while the remaining studies were from low- and middle-income countries. We identified common global barriers and motivations to care-seeking across studies, as well as barriers specific to study settings. The findings may help to develop interventions that lower barriers to seeking care and/or identify alternate methods of collecting surveillance data and delivering care by leveraging insights into patterns of care-seeking to collect data and engage with informal care settings.
Methods
We conducted a qualitative meta-synthesis using a rigorous methodological approach to identify broad themes and insights across multiple study settings. Previous studies have demonstrated that this process can lead to a comprehensive understanding of complex issues, which is especially beneficial for interpreting complex care-seeking behaviours.1114 Our approach followed established guidance for qualitative evidence synthesis, drawing on methods outlined by Barnett-Page and Thomas,15 Finlayson and Dixon16 and Dixon-Woods et al.17 We use qualitative meta-synthesis to describe the overarching interpretive integration of our findings, thematic coding to denote the process used to organise and interpret findings across studies and grounded-theory-informed comparison to capture the techniques used during theme refinement.
Search strategy
Mixed-methods and qualitative studies were identified by a previous systematic review of care-seeking for diarrhoea.5 Briefly, PubMed, Embase, Web of Science and Global Index Medicus were initially searched on 23 January 2023, and the search was updated on 3 September 2024. The review included quantitative and qualitative studies examining the proportion of people with a diarrhoeal illness who sought care for themselves or their child. Any study reporting mixed or qualitative methods during title and abstract or full-text screening was flagged for inclusion in this qualitative meta-synthesis.5 Exact search terms and further descriptions of study methods can be found in the manuscript and supplementary materials of Wiens et al.5
Eligibility criteria
We included studies from any country and time period that employed a qualitative study design to examine reasons individuals did or did not seek care for themselves or a child with diarrhoeal illness. We did not set limits on language, publication date or sample size. We excluded studies that (1) did not report care-seeking motivations specifically for diarrhoea (eg, discussed general childhood illnesses), (2) did not report data obtained through qualitative study design methods, including individual interviews, focus group discussions or other forms of open-ended study design, (3) were reviews or secondary analyses or (4) did not have full texts available.
Study screening methods
Identified studies were uploaded to Covidence (https://covidence.org) and screened for eligibility. Full texts were assessed for eligibility by two independent reviewers (two of MHM, SMH, ENR and KEW). A third reviewer (MHM, SMH, ENR or KEW) served as a tie-breaking vote when needed.
Data extraction and coding
Two reviewers (MHM and SMH) extracted study information from included studies in a table format. We did not perform a formal quality assessment of the included qualitative studies. While the Critical Appraisal Skills Programme’s checklist for evaluating the quality of qualitative studies exists,18 there is no agreement on what score merits exclusion.17 19 Our objective was to conduct a meta-synthesis to identify cross-contextual patterns and themes in care-seeking behaviour, rather than to rank or aggregate findings quantitatively. As described below, systematic extraction and transparent thematic analysis were used to ensure rigour and credibility while preserving insights from a broad range of study contexts.
Two reviewers (MHM and SMH) independently coded factors influencing care-seeking decisions using ATLAS.ti Web (https://atlasti.com/atlas-ti-web). This platform was selected to facilitate simultaneous collaboration and data management among the research team. ATLAS.ti allowed the team to manage the large volume of material and maintain consistent coding across all sources that could be easily revisited. The two reviewers divided the articles to code, extracted qualitative data and then reviewed each other’s work to assess agreement. Throughout this process, both reviewers kept audit journals, tracking any questions, comments or thoughts they had during this process to ensure transparency and reproducibility and reduce bias. For the updated search, a single reviewer (MHM) extracted and qualitatively coded data in accordance with the parent study.5 A third reviewer (KEW or ENR) moderated group reconciliation meetings to resolve any disagreements, and all reviewers agreed on the final decision.
We developed the codebook using a structured approach informed by thematic analysis and grounded theory principles. We began the process by brainstorming potential influences on care-seeking behaviours informed by the research team’s existing understanding, as well as concepts the full-text reviewers identified during the screening process. A single reviewer (ENR) then conducted a preliminary screening of a small sample of included, geographically distinct studies using open coding. Subsequently, we combined the concepts already identified as potentially relevant with any new concepts that emerged from the screening and open coding to create a preliminary codebook. We structured the codebook hierarchically, with parent codes representing anticipated major themes and child codes capturing more specific aspects of each theme. As we worked through this process, we continuously compared our codes to ensure each one was clearly defined and did not overlap with others.
We applied the codebook to all included studies and refined it as needed when information in the articles did not clearly fit within the existing codes. For example, we expanded the ‘external other’ code to also capture religious ideas. Similar ideas were managed as groups under one parent code in ATLAS.ti, with individual child codes in the parent group used for thematic synthesis. The final codebook used by reviewers is shown in online supplemental table S1.
Thematic analysis
After coding all studies, we summarised and reviewed the content included under each child code to search for broader patterns of meaning. Within each code, we identified themes to capture the nuances of the data and structure the main themes. To develop a comprehensive thematic framework, two researchers (MHM and SHM) independently created model theme trees based on patterns in the coded data. We then presented these frameworks to the full research team, using their input to refine the two frameworks into a single structure. After this initial restructuring, we conducted two rounds of feedback to ensure all themes and subthemes were comprehensive, distinct from each other and answered the research question.
Patients and public involvement
Patients or members of the public were not involved in the design, conduct, reporting or dissemination of this qualitative meta-synthesis, as the study relied exclusively on published literature.
Results
Search results
After screening 5188 studies, Wiens et al identified 106 studies for review.5 Following full-text screening, 47 studies met the inclusion criteria for our meta-synthesis (figure 1).
Preferred Reporting Items for Systematic Reviews and Meta-Analyses diagram. The diagram shows the search, screening and inclusion process for the systematic review, including the databases searched and reasons for studies that were excluded. Studies were identified and initially screened in a previous review.5
Characteristics of included studies
The included studies are detailed in online supplemental table S2. The studies came from 25 countries, with most from Sub-Saharan Africa and Southeast Asia. Specifically, South Africa (n=4), Pakistan (n=4), Kenya (n=3), Nigeria (n=3), Bangladesh (n=3), Vietnam (n=3), the Democratic Republic of the Congo (n=2), Ethiopia (n=2), Ghana (n=2), Mali (n=2), Sierra Leone (n=2), India (n=2), Thailand (n=2), Burkina Faso (n=1), Cameroon (n=1), Central African Republic (n=1), Niger (n=1), Uganda (n=1) and Nepal (n=1). The remaining studies were from Canada (n=4), Ecuador (n=1), Brazil (n=1), Nepal (n=1), Egypt (n=1) and Vanuatu (n=1). 25 studies were conducted in rural areas and 10 in urban areas, with the remaining 12 study locations in mixed rural-urban settings. Among studies with information about sampling dates (n=39), completion dates ranged from 1993 to 2021, with the majority from 2010 to 2014 (n=14). Studies employed individual interviews (n=18), group interviews (n=5) or a mix of both (n=24). Most studies asked about care-seeking practices for children with diarrhoea (n=39), but some asked about care-seeking for the respondents themselves (n=9) and/or a hypothetical diarrhoeal episode (n=4). 35 studies did not provide an explicit definition for diarrhoea, while the remainder used the WHO’s case definition20 (n=3), acute gastroenteritis (n=4) or cholera/severe diarrhoea (n=5).
Thematic analysis
For clarity, we described key insights from the thematic analysis linearly in the sections below. However, in reality, care-seeking decisions are multifaceted and deeply contextual. Across the included studies, care-seeking behaviours were influenced by sociocultural practices and norms, perceived severity of the diarrhoeal illness, ease of access to different providers and facilities and the perceived quality of those providers and facilities (figure 2). The presence of themes, as well as their influence on care-seeking decisions, varies across studies. To explore how these themes affect care-seeking decisions overall and within individual studies, please refer to online supplemental table S3. A complete summary of all the themes and subthemes that we identified is summarised in table 1, along with the studies that described them.
Visualisation of care-seeking decisions. Factors that influence individual decisions to seek care across geographic settings. The diagram structure was adapted from Tefera and Yu.75
Theme 1: sociocultural practices and norms guide care-seeking behaviour
We found that cultural factors influenced perceptions of diarrhoeal illness and its appropriate treatment. While included studies represented many diverse settings, several common patterns of care-seeking emerged. Respondents widely reported integrating both biomedical and traditional approaches, blending elements of each rather than strictly following either. These beliefs influence how symptoms are understood, who is regarded as the authority on the illness and thus how respondents make care-seeking decisions. This syncretic system reinforces the importance of culturally competent care and community-based participatory research.
Cultural aetiological beliefs
We found that cultural beliefs about the cause of diarrhoea often influenced care-seeking behaviour. Study participants in 10 studies made a distinction between diarrhoeal episodes that were recognised as diarrhoeal illness and diarrhoea that was not associated with any illness. Caregivers commonly viewed diarrhoea as a normal part of childhood development, not as a symptom of disease. As explained by one mother in urban Yemen, “This diarrhoea is not a disease; it never responds to doctors’ advice.”21 These episodes were seen as benign and self-limiting, not requiring treatment, while other forms of diarrhoea were interpreted as signs of disease that necessitated treatment outside the home.2130
When diarrhoeal episodes were seen as pathogenic, perceived causes shaped both how severe they were perceived to be and treatment choices. Caregivers believed some illnesses were ‘traditional’ and untreatable with Western medicine. These illnesses, though recognised as pathogenic, were considered uniquely specific to the community and distinct from modern disorders. Traditional illnesses were often viewed as serious and required traditional rather than medical treatments.2122 2427 30 Similarly, perceived supernatural causes of diarrhoea could deter families from seeking care at a hospital or clinic, leading them to consult traditional or spiritual healers instead. As these cases were typically regarded as serious, treatment was usually sought promptly. Respondents’ belief in witchcraft, punishment from the gods, evil eyes, malicious spirits and undefined supernatural entities was not limited to any specific region.2526 28 30 32 34 3744 In contrast, when diarrhoea was attributed to weather or diet, the illness was often viewed as mild and self-limiting, thus not requiring care from hospitals or clinics.2123 25 26 2830 35 39 41 As a mother in South Africa explained, “I did not think it was serious. I thought it was due to cold weather and it will subside.”28
Influence of community
Community members played a wide variety of roles in care-seeking, including giving advice, herbs for treatment, financial or logistical support or, in some cases, permission if a father or husband was not available. Elders in rural communities often discouraged the use of modern medicine in favour of traditional treatments in sub-Saharan Africa and Southeast Asia.232527 29 31 35 36 39 41 As one parent stated, “Everything must be discussed with the grandparents […]. After discussing, if all agree, we let the child go (to the CHS [community health station]).”35
Gender norms
We also found that gender roles in decision-making shaped care-seeking. In five studies, fathers held financial control and authority within families, especially in rural sub-Saharan Africa. Women participating in the included studies often recounted having limited autonomy to seek care for their children without first obtaining their husbands’ approval, which could delay treatment. If the male authority figure was unavailable or unwilling to provide money for care, women turned to traditional medicine or informal vendors as cheaper alternatives.24 31 35 36 41 50 As a father in Nigeria explained, “Money can actually delay the mother from seeking care; as a mother, when you don’t have money, you would have to wait for the father…”24 In one of the rare studies that did not limit the inclusion to mothers, fathers in a rural area of Ethiopia were deterred from seeking care at health posts, which respondents described as women-only spaces. One father explained, “I do not go to the health post, as it is only for women and children.” Fathers also reported not knowing what treatments or levels of care were available at these posts.42 A study conducted in Egypt during 1996–1997 found that a child’s sex influenced care-seeking behaviour. As one mother explained, “Here the attention is more focused on the boy than the girl. For example, if the boy gets sick, we take him to the doctor, but if it is the girl… God supports her, and she gets well on her own.”53
Culturally driven provider choice
Cultural norms often shaped care-seeking practices, not always through specific beliefs but because it was simply what one does: what is familiar and expected.212325 27 31 35 36 39 41 43 The choices often reflected a sense of embeddedness in cultural routines and expectations, where traditional care was not necessarily weighed against biomedical options but accepted as a part of the natural course of action. As one mother in rural South Africa explained, both options exist within that familiar world: “There is help from a traditional healer, and there is help from the hospital, so you don’t know where your child is going to get help. And there are things that sangoma [traditional healer] can do, and the hospital cannot do, and there are things that the hospital can do that a sangoma cannot do.”39
Awareness of home remedies
Home remedies were a culturally ingrained part of care-seeking behaviour in many communities. Reliance on home remedies could act as both a solution and a barrier212327 29 31; they may provide immediate relief or comfort for mild to moderate diarrhoea, but study authors noted that they could also delay medical care.25 43 50 51 54 57
Theme 2: diarrhoea perceived to be severe is treated outside the home
We found that care-seeking for diarrhoeal disease can be viewed on a continuum that varies with diarrhoea severity. Respondents often reported higher rates of care-seeking for diarrhoeal illnesses they perceived to be more serious, while illness episodes viewed as minor were primarily treated with home management or traditional remedies. Participants also used illness duration and symptoms as tools to assess the severity of the illness and as a means to determine what, if any, type of care-seeking was necessary.
Illness duration
Participants in the reviewed studies often described escalating care-seeking depending on the length of symptoms, moving from home management to outside care or traditional healers to health facilities, with the timeframes for these transitions varying between studies from days to years.262831 34 As one woman in Niger reported, “My child had diarrhoea for 3 years, and then it became life-threatening, and I took the child to the clinic.”26 In comparison, a caregiver in Pakistan reported that, “We observe for whole day and night; if the child’s condition gets worse, then we rush to the doctor.”50 For example, among caregivers in urban Canada, when their child’s illness lasted longer than they expected, they escalated care-seeking to the paediatric emergency room.47
Symptoms
Study participants viewed the presence or absence of certain symptoms as evidence of severe disease. Signs of dehydration,24 35 37 38 56 59 60 diarrhoea in combination with fever or vomiting,27 29 47 49 59 61 decreased or loss of appetite29 60 61 and bloody or watery diarrhoea21 23 29 37 38 49 58 60 were all noted as signs that participants should seek care outside the home for their child. Specifically, caregivers who identified signs of dehydration24 35 37 38 56 59 60 62 or symptoms consistent with cholera21 23 27 29 37 38 49 58 60 largely reported seeking care outside the home. Respondents frequently did not consider diarrhoea on its own severe, and thus it was not treated outside the home, especially in rural areas.28 29 31 44 48 54 63 64 Canadian respondents reported conflicting influences of observed ‘suffering’ during diarrhoeal illness on care-seeking, varying by age. For caregivers of children in a mixed urban-rural setting, the perception that their child was suffering led them to the emergency room,47 while for adults in a rural community of indigenous people in Canada, acute gastrointestinal illness was something the community believed a person had to ‘suffer through’.48
Theme 3: negative feelings drive the type of care sought
Study participants who used modern healthcare providers often expressed negative feelings, including anxiety, helplessness and fear. These negative feelings collectively influenced respondents’ healthcare decisions, reflecting how emotional state drives the nature and urgency of care sought. This sense of urgency often led to care-seeking in hospitals or clinics. For others, fear over the treatment itself might result in avoidance of hospitals or clinics.
Feeling anxious
Worry was a common reason caregivers sought care outside the home. Concern over a patient’s vulnerability, due to their age or pre-existing conditions, often prompted seeking more intensive care, such as moving from home remedies to clinical treatment or from primary care to emergency care. Patient vulnerability frequently led to an increased sense of urgency,27 35 39 47 56 58 62 as one caregiver in Canada explained, “I didn’t want it to go on to a point where it was going to cause more problems for her, so I wanted to get her in as soon as possible” (Interview 4).47 In many cases, caregivers described seeking more advanced levels of care when the illness did not improve or worsened, as continued symptoms deepened their concern and prompted action.212426 29 31 34 36 38 40 43 45 50 55 As a caregiver in Pakistan states, “We try to treat them at home. We give Flagyl (metronidazole) and ORS [oral rehydration solution] (for diarrhoea), despite that if the child’s condition is not getting better, then we take the child to hospital.”50 Feeling distress over the uncertainty of what was wrong was also an impetus to seeking care47 56.
Feeling helpless
Feelings of helplessness in managing diarrhoeal illness prompted caregivers to seek care and reassurance from healthcare providers.25 27 31 35 39 47 56 61 62 65 This was especially true for first-time parents,27 31 35 47 including a caregiver in Canada who stated, “I tried to [treat the illness] this time…I really try my best to take care of what I can here, and then if things get to a point that I’m a little worried, then we normally go in to see a doctor.”47 Caregivers in an indigenous community in Uganda also described feeling helpless if they felt they had limited options for care outside of the home.55
Risk posed by treatment
Participants, especially caregivers of sick children, sometimes viewed Western treatments intended to help manage diarrhoeal illness as harmful. Participants reporting these concerns came from rural areas27 31 35 36 38 41 44 or had arrived in an urban area from either slums or rural areas.43 Participants reported fear that the Western medicine and pharmaceuticals offered might be harmful and possibly even cause death. This led to decreased use of health facilities and drug peddlers whom caregivers did not trust.21 35 36 38 41 43 44 58 One mother stated that she finds “herbal medicines more ‘compatible’ for a body of a child since they are not harmful as drugs can be.”35 In rural Uganda, respondents were concerned that hospitals could expose them to other pathogens.55
Theme 4: ease of access shapes care-seeking practices
Structural and logistical factors played a critical role in shaping participants’ ability to obtain healthcare. Financial burden, including both direct service costs and indirect expenses, was a key deterrent. Many participants also reported barriers, such as distance and operating hours, that diminished their ability to seek care at desired facilities. These barriers often create opportunity costs, as overcoming them requires time, energy and financial resources that could be allocated to other essential needs. This dynamic may reflect systemic inequities that compound barriers to care, making the decision to seek treatment even more challenging.
Financial costs
Costs were frequently mentioned as a reason to avoid or delay care at a hospital or clinic. This often led participants to rely on traditional healers, traditional medicines or informal drug sellers because they were less expensive.222531 35 36 38 40 46 50 52 As a respondent in rural Bangladesh explained, “It is not easy for us to seek medical treatment now, it is easy to seek treatment when you have the money and can afford to access the medical facilities available.”46 Similarly, a participant in rural Uganda explained that “If I have not paid the hospital, I try by all means to get herbs from forests or places around my home. I take the herbs, and if they fail to heal me, I wait for death” (male).55 In addition, one study reported that pharmacists or informal service providers who offer payment plans were preferred when participants could not pay all hospital fees up front.24
Specific medical costs associated with not seeking care included the cost of medications, consultations, admission fees and/or laboratory tests. Studies mentioning these costs were all in rural areas,24 31 35 46 50 54 57 61 65 67 although some of these locations noted having free services or fee exemption programmes in place for children under five.24 35 50 57 61 65 Only urban caregivers in a mixed study population in Kenya mentioned free or low-cost care being available, and it was those caregivers who stated they frequented health facilities when their children were sick.38 Caregivers in Thailand reported occasionally using a health centre because it was free but most often used private services, despite the increased cost, because they found that the services were better.49 11 studies, all in rural areas, reported that transportation costs associated with care-seeking were a barrier to seeking care at formal care providers.242631 35 36 43 46 50 55 65 67
Distance to provider
Distance to a health facility was frequently reported as a barrier to seeking care, especially in studies in rural areas. Distance often led to decreased ability to get to clinics, hospitals and other medical providers, and so respondents relied instead on traditional healers, drug sellers and home remedies.2324 26 3436 38 39 45 46 49 50 53 However, what constituted distance varied widely and was not consistently reported by study authors. In South Africa, one caregiver described travelling 60 km to obtain medication for their child as easy,39 while another recounted a half-day to full-day walk as a huge barrier to seeking care in rural Vietnam.35 As explained by one mother in Nepal, “I believe in herbs but not in traditional healers. However, my mother took my baby to dhami-jhankri, a traditional healer, and she was cured. If hospital is far, we should sometimes visit traditional healers for the sake of child” (in-depth interview (IDI)-mother 2).23 Many respondents mentioned needing to walk to the healthcare provider. This was even more challenging in flood-prone areas, where travel by foot or vehicle was frequently impossible or difficult to navigate.26 28 29 57 65 Many caregivers described selecting whoever was closest to home, as explained by one focus group participant, “If the health centre was close by, we would go there for medication, but we always find trouble getting to Bwindi Hospital, so we have to take herbs.”55 Another mentioned a “fear of walking long distances” and that it “always takes a lot of time to reach the hospital.”55 In a study that interviewed respondents from both urban and rural areas, some caregivers sought care from health facilities and chemists because they were closer to their homes. However, rural community members still cited distance as a barrier.38
Optimising cost-benefit value
Some studies found that the direct and indirect financial burden of care-seeking necessitated forgoing other important expenditures such as food35 54 67 and clothing.43 55 Seeking care outside the home might also require taking time off from work, which again reinforced the financial burden of care-seeking.26 50 Respondents, particularly female caregivers, cited competing priorities, such as work obligations, childcare and household needs, that prevented them from seeking care outside the home.26 35 43 50 65 Participants weighed the costs of transportation and services against the potential benefits of care, which were not always certain. This was illustrated by a mother in rural Kenya, who stated, “Sometimes, even if you find money and go [to the health facility], you feel like you are wasting money because it [treatment] doesn’t always work.”65
Facility characteristics
Limited facility hours resulted in delayed care, especially when illnesses were identified at night, when hospitals might not be open. In these situations, caregivers described relying on traditional medicine and healers, drug peddlers, family and home care.24 29 36 44 61 Caregivers described prolonged wait times as a reason to avoid certain facility types.24 25 29 36 44 55 56 As Brubacher et al described, “We always get to the hospital around 8 am, but we spend the whole day not being attended to, and sometimes they close up when they have not attended to us. This doesn’t make us happy at all. In most cases, when that happens, I never go back to the hospital but go back home and look for my herbs” (female).55 Only among ethnic minority caregivers in rural Vietnam did language barriers impact care, as facilities did not provide translators, requiring those seeking to bring someone with them or rely on patients at the facility to act as translators.35
Theme 5: the perceived quality of care influences care-seeking
We also found that the decision to seek care outside the home was influenced by participants’ perception of the efficacy of treatment and the reputation of the facility or provider. While many respondents’ explanations of how sociocultural factors influenced the types of care sought, respondents in many settings also reported viewing modern pharmaceuticals as essential for treating diarrhoea and often sought out facilities with reputations of being well-stocked. Quality issues were mentioned in 27 unique studies, 25 of which also mentioned sociocultural factors. The actual capacity of a healthcare site to deliver care was important, and decisions were strongly shaped by past experiences that built trust and confidence in providers’ competence. This illustrated how those seeking care must weigh the tangible benefits of medical treatments and their personal relationships with those providing them.
Efficacy of medication sought
Respondents frequently noted the efficacy of modern pharmaceuticals as a reason for seeking care outside the home, especially in Sub-Saharan Africa and Southeast Asia.2425 3336 38 39 43 49 50 54 55 57 61 63 For example, a caregiver in rural Uganda stated, “We always take the drugs and get cured…we always take the first option of going to a hospital” (female).55 Some believed the medications would stop the diarrhoea,25 33 35 38 49 55 while others mentioned it as a cure.25 55 As explained by a caregiver in Bangui, Central African Republic, “When you give the child medicine…this will stop the diarrhoea. Diarrhoea, isn’t that an illness? “If you don’t give the child medicine, she won’t get better!”25 This positive view of medications resulted in the selection of private facilities farther from home for study participants in several studies.27 33 49 50
Reputation of the facility
Study respondents reported that knowing a facility was adequately equipped with both doctors and medications positively impacted their decision to seek care there.24 29 33 35 36 38 46 50 53 61 63 65 When medications were not available at health facilities, respondents reported visiting informal providers or delaying care-seeking.29 35 36 46 50 61 63 Participants in several studies noted that the availability of medication was most frequently a problem at government and public health facilities.29 33 50 65 We identified only one study among an indigenous community in rural Uganda that stated that the cleanliness of the health facility and its improper maintenance were barriers to seeking care there.55
Reputation of the provider
We found that the reputation of a provider or facility for providing effective treatment engendered trust and confidence in seeking care there.24 33 34 36 39 43 47 49 50 55 62 Reasons for trusting providers included a history with the facility,33 36 39 successful treatment of past diarrhoeal illness34 47 or a high-quality service/interpersonal relationship with the provider.24 36 57 Others stated a more general feeling of confidence in the providers’ competence.24 36 47 48 55 56 Confidence that the provider could heal a child was especially important, as explained by a respondent in Canada, “…you know, it’s [the hospital emergency department] a magical place. Next time I’m bringing her after one day because right after we go, it always works out the same, [the illness] stops.”47 Cunnama and Honda described trust in hospital providers as a newer phenomenon, with one participant stating that “…it’s a good hospital…nowadays it’s not like before when our mothers used to go there. Like now, everything is done well there. It’s the right hospital.”39 Five studies, in both rural and urban areas, mentioned the desire to get a diagnosis as a reason to seek care at modern health facilities.24 35 36 38 50 56 Previous experiences of poor treatment, such as failure by the provider to successfully treat a past illness episode, providers responding negatively to patient accounts of home treatments administered before arrival or refusing to listen to patients’ understanding of the illness, also prevented caregivers from visiting specific health providers.21 25 29 35 36 44 46 50 53 58
Discussion
This review identified several barriers and facilitators to seeking care outside the home for diarrhoeal illness. We found that sociocultural beliefs about illness and caregiver response, the perceived severity of the illness, emotional reactions to a child being sick, accessibility of care and the expected quality of care all impacted the decision to seek care outside of the home across diverse geographic locations. In addition, while reasons for or against seeking care outside the home were presented here as discrete factors, respondents often reported multiple influences—some reinforcing each other and others in conflict—shaping their decisions. For example, an elder in the home advocating for traditional methods influenced decision-making, even in the presence of concerns about disease severity or aetiologic cause.27 41 42 Although respondents in one study trusted the quality of care available at a hospital, financial hardships remained a barrier to utilisation.25 Proximity to government facilities was not a facilitator of care-seeking when medications and equipment were unavailable, facilities were closed on weekends or providers were reported absent.29 Even positive views on the efficacy of medication are overlooked when home remedies and traditional healers are familiar and proximate.36 Ultimately, what an individual would have liked to do did not always align with what they could do.
In addition, we found that general diarrhoea—without signs of dehydration or blood in the stool—was often viewed as a routine part of child development rather than an illness requiring medical attention. This was frequently cited as a reason for not seeking care outside the home and may partially explain why we found no significant differences in hospital care-seeking for children under five compared with older individuals in our previous review of population-based survey data.5 While many examples related to mild episodes that may not require care outside of the home,222529 32 35 some involved moderate-to-severe dehydration or were described as illnesses that led to extended hospital stays or death.21 27 31 36 37 41 44 Considering these differences in understanding diarrhoea, using local terminology for diarrhoeal episodes and including descriptions of the event (ie, three loose stools) could improve the accuracy of studies investigating prevalence and care behaviour for diarrhoeal illness.
We also found that traditional healers were more commonly reported as a source of care in the qualitative studies than in our previous review of quantitative studies.5 This difference may reflect the fact that non-medical providers are included less frequently in survey questionnaires5 and/or could be a result of how the questions themselves are phrased. For example, participants may be less likely to report use of a traditional healer if only one source of care can be selected. Additionally, different perceptions of illness may influence responses to survey questions, as respondents in qualitative studies differentiated between illnesses requiring biomedical treatment and those best addressed by traditional or spiritual healers. Not explicitly asking about behaviours for a broad range of diarrhoeal symptoms may lead to incomplete utilisation histories, particularly for traditional and spiritual healers.
Our findings closely align with several established theoretical models identified by a review of healthcare utilisation models, particularly those by Andersen68 69 and Kukafka et al’s70 frameworks. Both models emphasise the importance of health beliefs, access to healthcare, social support and perception of illness. Cultural beliefs and severity of illness influence how individuals view their health and the need for care, much like Andersen’s68 69 model suggests. Fear, as identified in our review, ties into the emotional and psychological barriers highlighted by Kukafka et al,70 which stress the role of emotional responses, symptom interpretation and self-efficacy in the decision-making process. Together, these models and our findings point to a range of internal, external and community-level factors that collectively shape whether and how individuals seek care.71
While these findings provide context for understanding care-seeking behaviour, several limitations should be acknowledged. First, this is a synthesis of data that previously underwent synthesis. It is possible that loss or alteration of information occurred in either or both stages. Second, there was a wide variety of study designs, care provider options described and illness definitions, limiting direct comparison between studies. While no restrictions were set on the study population or geographical location, the majority of studies were conducted on caregivers of children in Sub-Saharan Africa and Southeast Asia, which may limit the generalisability of findings to other settings. Despite the rigour of our methods, it is possible that the search strategy and/or screening process missed pertinent articles. Studies missed may have produced stronger or contrary information than is presented here. Additionally, as we did not conduct a formal quality appraisal of included studies, it is possible that methodological limitations within individual studies influenced the patterns we identified. Finally, all authors of this study are from high-income countries, whereas most studies were conducted in low-income countries or low-resource settings. While we have aimed to centre participant perspectives, our analyses and conclusions may still be influenced by implicit biases shaped by our backgrounds.
Our findings highlight key methodological gaps that could be addressed in future studies. While there was broad consensus that severe illness prompts urgent care outside the home, it was not always clear how respondents defined severe illness. Including clear and location-appropriate case definitions and symptom descriptions will be important for future work. Consistent with our previous review,5 community health workers were rarely mentioned as a source of care. It remains unclear if this is evidence of non-use or a result of how ‘healthcare’ is defined. As community health workers are trained community members themselves rather than medical professionals,72 73 they may not be thought of as official sources of care without direct prompting. This perspective is supported by Hodgins et al, who noted that the term ‘community health worker’ encompasses a diverse cadre of roles and responsibilities, which complicates consistent recognition of their role as formal healthcare providers.74 Finally, this review highlights the relative scarcity of qualitative studies compared with quantitative research on care-seeking for diarrhoeal illness. Given the wide variation in care-seeking across settings,5 mixed-methods approaches that examine where, when and why people seek care will be important for understanding local-level care-seeking.
The themes we identified as shaping care-seeking decisions across diverse settings offer important insights for designing both interventions and more responsive surveillance systems. Understanding how and when individuals seek care can help identify where case detection is likely to miss milder illness, where mistrust or limited access hinders reporting and where community-based approaches may be needed to better estimate disease burden, despite their resource demands. In addition, expanding educational campaigns that engage with local understandings of disease aetiology may support more timely and appropriate care-seeking. This review found that decisions were influenced more by perceived necessity than by cost alone, suggesting that interventions should focus on improving recognition of when and what type of care may be needed. For these efforts to succeed, individuals must also have trust in local healthcare providers. Depending on the context, this may involve ensuring providers have appropriate treatments and adequate staffing or engaging community health workers and trusted local leaders in care delivery. Strengthening caregiver knowledge and confidence in a setting-specific manner may help reduce delays or avoidance in seeking care, ultimately contributing to reduced morbidity and mortality from diarrhoeal disease.
Supplementary material
10.1136/bmjopen-2025-109903online supplemental file 1
10.1136/bmjopen-2025-109903online supplemental file 2
10.1136/bmjopen-2025-109903online supplemental file 3
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ferrari AJ Santomauro DF Aali A et al Global incidence, prevalence, years lived with disability (YL Ds), disability-adjusted life-years (DAL Ys), and healthy life expectancy (HALE) for 371 diseases and injuries in 204 countries and territories and 811 subnational locations, 1990–2021: a systematic analysis for the Global Burden of Disease Study 2021 The Lancet 202440321336110.1016/S 0140-6736(24)00757-8PMC 1112211138642570 · doi ↗ · pubmed ↗
- 2Webb C Cabada MM A Review on Prevention Interventions to Decrease Diarrheal Diseases’ Burden in Children Curr Trop Med Rep 20185314010.1007/s 40475-018-0134-x · doi ↗
- 3Santosham M Chandran A Fitzwater S et al Progress and barriers for the control of diarrhoeal disease The Lancet 201037663710.1016/S 0140-6736(10)60356-X 20609988 · doi ↗ · pubmed ↗
- 4The integrated global action plan for prevention and control of pneumonia and diarrhoea (GAPPD)2013 Availablehttps://www.who.int/publications-detail-redirect/the-integrated-global-action-plan-for-prevention-and-control-of-pneumonia-and-diarrhoea-(gappd)
- 5Wiens KE Miller MH Costello DJ et al Care-seeking for diarrheal illness: A systematic review and meta-analysis PLOS Glob Public Health 20255 e 000448310.1371/journal.pgph.000448340261857 PMC 12013865 · doi ↗ · pubmed ↗
- 6Chakrabarti A Determinants of child morbidity and factors governing utilization of child health care: evidence from rural India Appl Econ 201244273710.1080/00036846.2010.498367 · doi ↗
- 7Geldsetzer P Williams TC Kirolos A et al The recognition of and care seeking behaviour for childhood illness in developing countries: a systematic review P Lo S One 20149 e 9342710.1371/journal.pone.009342724718483 PMC 3981715 · doi ↗ · pubmed ↗
- 8Pierce H Gibby AL Forste R Caregiver Decision-Making: Household Response to Child Illness in sub-Saharan Africa Popul Res Policy Rev 2016355819710.1007/s 11113-016-9396-y 28794575 PMC 5546145 · doi ↗ · pubmed ↗