Multisystem Disease With Suspected Malignancy: Clinical Management Following Diagnostic Refusal
Márcia Moreira Costa, Anabela Andrade, Ana Raquel Dias, Marta Henriques Baptista, Afonso Carvalhal

TL;DR
This paper discusses the ethical and clinical management of an elderly patient who refused further cancer testing, emphasizing personalized care and patient autonomy.
Contribution
The paper highlights a practical approach to managing diagnostic uncertainty and respecting patient autonomy in primary care.
Findings
The patient's refusal of further testing led to a shift in care toward palliative support and continuous follow-up.
The case demonstrates how ethical principles guide clinical decisions in the absence of a definitive diagnosis.
Primary care physicians can maintain quality care through trust and individualized strategies in complex cases.
Abstract
Follow‑up of older adults in primary care often entails clinical challenges that go beyond diagnosis. Comorbidities, functional limitations, and social vulnerabilities require a holistic, person‑centred approach grounded in a continuous and trusting doctor-patient relationship. We present a case of an 88-year-old man followed in Family Medicine consultations, who presented with cervical and abdominal skin lesions evolving over three months. Imaging findings were highly suggestive of disseminated oncologic disease. Two biopsies were performed, but no definitive diagnosis was reached. After a clear clinical explanation regarding diagnostic hypotheses and likely disease progression, the patient refused further aetiological investigations. Respecting the principle of autonomy, the clinical management strategy shifted towards continuous follow‑up, adaptation of the therapeutic plan, and a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
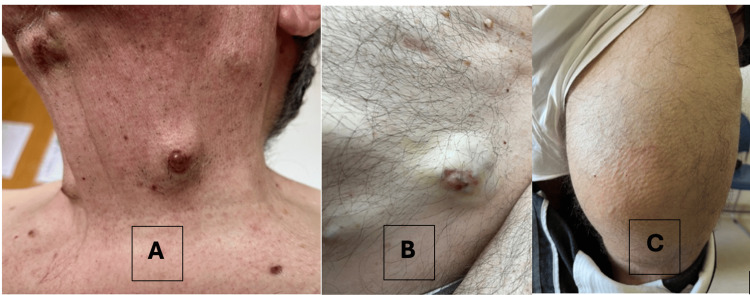 Figure 1
Figure 1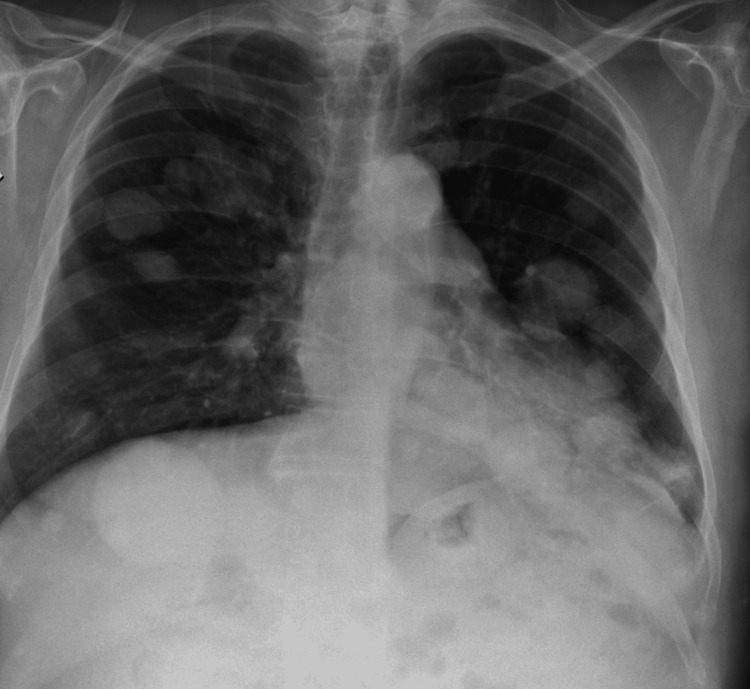 Figure 2
Figure 2| Test | Result | Reference Range |
| Hemoglobin (Hb) | 12.7 g/dL | 13.0–17.0 g/dL |
| Mean Corpuscular Volume (MCV) | 88.9 fL | 80–100 fL |
| Red Cell Distribution Width (RDW) | 15.6% | 11.5–14.5% |
| Erythrocyte Sedimentation Rate (ESR) | 43 mm/h | <20 mm/h |
| C-Reactive Protein (CRP) | 12.2 mg/L | <5 mg/L |
| Lactate Dehydrogenase (LDH) | 271 U/L | 135–225 U/L |
| Creatinine | 0.91 mg/dL | 0.70–1.20 mg/dL |
| Alanine Transaminase (ALT) | 29 U/L | <41 U/L |
| Aspartate Transaminase (AST) | 25 U/L | <40 U/L |
| Total PSA | 4.90 ng/mL | <4.00 ng/mL |
| Free/Total PSA Ratio | 46.9% | >25% |
| CEA | 1.3 ng/mL | <5.0 ng/mL |
| CA 19-9 | 6.4 U/mL | <37 U/mL |
| CA 15-3 | 8.8 U/mL | <25 U/mL |
| CA 72-4 | 3.5 U/mL | <6.9 U/mL |
| Alpha-fetoprotein (AFP) | 1.8 ng/mL | <10 ng/mL |
| Cyfra 21-1 | 1.0 ng/mL | <3.3 ng/mL |
| Serum Protein Electrophoresis | Polyclonal increase in gamma globulins | No monoclonal peak |
| Date | Clinical events |
| April 2025 | Onset of multiple cutaneous lesions |
| July 2025 | Primary care follow‑up consultation: mass and cutaneous lesions identified. Laboratory workup and thoraco‑abdominopelvic CT scan requested |
| August 2025 | CT scan revealed multiple cutaneous, muscular, pulmonary, and osseous lesions. Referral to the Oncology Institute. |
| September 2025 | Incisional biopsy of an anterior cervical lesion (05/09/2025): diagnosis of benign chondroid syringoma. Biopsy of an abdominal lesion (26/09/2025): findings suggestive of mucinous adenocarcinoma, without immunohistochemistry |
| October 2025 | Patient declined further investigation; hospital teams proposed palliative care referral |
| November 2025 | Continued follow‑up in primary care |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsClinical Reasoning and Diagnostic Skills · Healthcare cost, quality, practices · Chronic Disease Management Strategies
Introduction
Clinical practice in Family Medicine is grounded in a biopsychosocial approach, where the therapeutic relationship, contextual understanding, and continuity of care are central pillars [1]. When confronted with signs suggestive of serious illness, particularly oncological disease, an aetiological investigation is typically conducted. This usually involves a structured diagnostic work-up, aiming to identify the underlying cause and initiate appropriate treatment. However, when patients decline further investigation, clinical priorities shift toward symptom-oriented management, structured follow-up, shared decision-making, and advance care planning.
Any diagnostic approach must respect the patient’s autonomy and sociocultural context [2]. A refusal to proceed with further diagnostic procedures should not be seen as the end of clinical care, but rather as a prompt to adapt the management plan in order to align with the patient’s values and preferences, within an ethical framework [2-4]. This case illustrates how primary care physicians can ensure meaningful and ongoing follow-up, even in the absence of a definitive diagnosis.
Case presentation
The patient was an 88-year-old retired man, formerly an electrician, living independently and with no apparent signs of cognitive impairment. Cognitive screening using the Mini-Mental State Examination (MMSE) scored 28/30, and the patient was oriented to person, place, and time. He lived with his wife, who was also functionally independent and had a diagnosis of myelodysplastic syndrome. Their social support network was limited: they had no nearby relatives, and the patient maintained regular phone contact only with one of his two daughters, both of whom lived abroad. He reported managing daily activities autonomously, with no external caregiving support at the time of consultation.
The patient reported no history of smoking or alcohol consumption. His medical history included hypertension, dyslipidaemia, and benign prostatic hyperplasia. His medications included candesartan 16 mg plus hydrochlorothiazide 12.5 mg once daily, atorvastatin 20 mg plus ezetimibe 10 mg once daily, acetylsalicylic acid 100 mg daily, and Serenoa repens.
During a routine Family Medicine consultation, the patient reported the onset of multiple rapidly growing subcutaneous lesions located on the scalp, neck, chest, and abdomen. He mentioned only mild, non-significant weight loss (two kilograms over nine months) and denied fever, anorexia, along with respiratory, gastrointestinal, or genitourinary symptoms. On physical examination, approximately 10 cutaneous nodules were noted on the scalp, neck, chest, and abdominal wall, measuring between 1 and 5 cm in diameter (Figure 1). These were firm, non-tender, violaceous, and in some cases fixed to underlying tissues. One lesion on the abdominal wall presented with superficial ulceration (Figure 1B). A large, longstanding indurated mass measuring approximately 18 × 13 cm was also identified on the anterior aspect of the left thigh (Figure 1C), reportedly unchanged for over two decades. No axillary or cervical lymphadenopathy, hepatosplenomegaly, or peripheral oedema were detected. Vital signs were: BP 112/58 mmHg, BMI 27.3 kg/m², afebrile. Cardiopulmonary and abdominal examinations were unremarkable.
Clinical presentation of cutaneous and subcutaneous lesions.A) Firm, violaceous nodules on the cervical region; B) Subcutaneous lesion with superficial ulceration on the abdominal wall; C) Large, longstanding indurated mass on the anterior aspect of the left thigh.
A thoracoabdominopelvic computed tomography (CT) scan and blood tests were requested. Blood tests were performed and showed mild normocytic anaemia with increased red cell distribution width (RDW), along with slightly elevated inflammatory markers, including erythrocyte sedimentation rate and C‑reactive protein. Renal function was preserved, and liver enzymes were within normal limits, except for a mild elevation in lactate dehydrogenase (LDH). Serum protein electrophoresis revealed a diffuse increase in the gamma-globulin fraction without a monoclonal peak, consistent with a possible polyclonal hypergammaglobulinaemia. Tumour marker analysis showed a mildly elevated prostate-specific antigen (PSA) level (total PSA 4.90 ng/mL, free/total PSA ratio 46.9%), while other tumour markers (carcinoembryonic antigen (CEA), CA 19‑9, CA 15‑3, CA 72‑4, alpha-fetoprotein (AFP), and Cyfra 21‑1) were within the reference range (Table 1).
The CT revealed multiple subcutaneous and intramuscular lesions, nodular pulmonary lesions, mediastinal lymphadenopathy, and lytic bone lesions. The thigh mass involved diffuse infiltration of the left quadriceps. These findings were strongly suggestive of disseminated oncologic disease. Additionally, a chest radiograph (Figure 2) showed multiple bilateral nodular opacities with a random distribution pattern. While some nodules displayed well-defined borders, others had ill-defined margins, raising suspicion for hematogenous dissemination. These radiologic findings further supported the hypothesis of widespread metastatic disease. However, the patient was unable to retrieve the CT images from the oncology centre due to logistical limitations; thus, representative CT images could not be included in this report.
Chest radiograph showing multiple bilateral pulmonary nodules.The radiographic pattern suggests hematogenous spread, raising suspicion for disseminated metastatic disease.
The patient was referred to the national oncology centre, where he underwent a multidisciplinary evaluation by the Internal Medicine, Dermatology, and Pulmonology teams. An excisional biopsy of a cervical nodule (Figure 1A) revealed histological features consistent with chondroid syringoma, without evidence of malignancy. Due to the discordance between histological findings and the clinical/imaging context, a second incisional biopsy was performed on an abdominal lesion (Figure 1B), which revealed mucinous adenocarcinoma with extensive necrosis. Immunohistochemical analysis was non-contributory due to lack of viable tissue, and repeat sampling was recommended.
After explaining the likely diagnosis and need for further investigation (including a third biopsy), the patient declined. At a follow-up visit, he confirmed his decision, citing the absence of symptoms and his advanced age. His ability to understand, deliberate, and communicate healthcare decisions was reaffirmed during the consultation, supporting the ethical basis for informed refusal. Respecting his autonomy, a referral for hospital-based palliative care was proposed which he accepted but preferred to postpone scheduling. The clinical course and key milestones are summarized in Table 2.
In the primary care setting, a management plan was developed including regular clinical monitoring, functional assessment, and medication review. Advance care planning was initiated, addressing the patient's values, preferences, and potential future treatment limitations. Given the fragile support network and his wife’s health condition, psychosocial support was offered, and home care services and community resources were considered depending on future clinical needs.
Discussion
This case exemplifies the complexity frequently encountered in primary care, particularly when there is strong clinical suspicion of serious disease but further investigation is limited by patient choice. In such scenarios, a person-centred approach becomes essential, emphasising attentive listening, transparent communication, respect for autonomy, and adaptable care planning [1-3].
The presence of multiple cutaneous and visceral lesions, along with imaging findings highly suggestive of disseminated occult malignancy, warranted further diagnostic investigation. However, the absence of definitive histological confirmation and the patient’s refusal to pursue further testing required a readjustment of the clinical strategy without compromising continuity of care.
The physician’s longstanding relationship with the patient, coupled with an understanding of his personal history, family dynamics, and core values, enabled close and individualised follow-up. Active surveillance, clear and open communication, and the non-coercive proposal of palliative care reflect key principles of Family Medicine as outlined by the World Organization of National Colleges, Academies, and Academic Associations of General Practitioners/Family Physicians (WONCA), including person-centredness, care continuity, and complexity management [1].
While chondroid syringoma is a rare benign cutaneous neoplasm, its isolated identification in the context of widespread disease demands caution in interpretation, particularly when it contradicts clinical and imaging findings. Although malignant variants of chondroid syringoma with infiltrative or metastatic potential have been described, their rarity calls for a broader differential diagnosis, including primary malignancies of non-cutaneous origin, which appears more likely in this case [5-7].
The finding of extensive necrosis and morphological features suggestive of mucinous adenocarcinoma in the second biopsy raised the possibility of an undetected primary malignancy. Although the primary tumour remained unidentified, a gastrointestinal or pancreatic origin could not be excluded. In the context of strong clinical and radiological suspicion of malignancy, the absence of histological confirmation highlights the diagnostic limitations posed by suboptimal sampling. This case therefore underscores the importance of integrating clinical, imaging, and pathological data to support informed, values-based decision-making [2-4,8].
Conclusions
The absence of a definitive diagnosis in this case may reflect clinical complexity and shared decision-making, rather than a failure of the diagnostic process. Upholding ethical and professional principles, particularly respect for patient autonomy, is essential to building a strong doctor-patient relationship and ensuring appropriate care. Managing clinical uncertainty requires not only technical competence but also a solid ethical foundation and relational skills that support continuity and progressive adaptation of care plans. This case exemplifies how primary care can accommodate diagnostic uncertainty through ethical, person-centred care that preserves patient dignity and supports ongoing reassessment.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Core values and principles of general practice and family medicine: perspectives of German GP residents-a cross-sectional study Front Med (Lausanne) Dreher AC Ko J Becker C 14957891220254007839810.3389/fmed.2025.1495789 PMC 11898739 · doi ↗ · pubmed ↗
- 2Principles of clinical ethics and their application to practice Med Princ Pract Varkey B 17283020213249807110.1159/000509119 PMC 7923912 · doi ↗ · pubmed ↗
- 3Shared decision-making in primary care: the neglected second half of the consultation Br J Gen Pract Elwyn G Edwards A Kinnersley P 477482491999 https://pmc.ncbi.nlm.nih.gov/articles/PMC 1313449/10562751 PMC 1313449 · pubmed ↗
- 4The cost of refusing treatment and equality of outcome J Med Ethics Savulescu J 231236241998975262410.1136/jme.24.4.231PMC 1377671 · doi ↗ · pubmed ↗
- 5Siringoma condroide maligno de localización facial con metástasis a distancia Actas Dermosifiliogr Mirandaa JA Mazzottab MM ZalazaraÉV 6526541142023
- 6Malignant chondroid syringoma: a systematic review Skin Health Dis Zufall AG Mark EJ Gru AA 03202310.1002/ski 2.144PMC 1006676037013126 · doi ↗ · pubmed ↗
- 7Clinical and dermoscopic characteristics of cutaneous chondroid syringoma: a systematic review Dermatol Pract Concept Di Guardo A Balampanos CG Gargano L Giordano D Capalbo A Persechino F Persechino S 14202410.5826/dpc.1404 a 237PMC 1162000939652927 · doi ↗ · pubmed ↗
- 8“The patient is being pressured!” Coercion versus relational autonomy J Palliat Med Mc Intee MF Madigan Mc Cown L Chessa F Hutchinson RN 9649672720243830616310.1089/jpm.2023.0333 PMC 12136145 · doi ↗ · pubmed ↗