The global profile of individuals undergoing total knee replacement surgery through a PROGRESS-PLUS equity lens: A systematic review
Marisa Coetzee, Amanda Clifford, Dominique C. Leibbrandt, Jacobus Jordaan, Quinette Louw

TL;DR
This paper reviews global data on knee replacement surgery patients, highlighting gaps in equity-focused research, especially in low-income countries.
Contribution
The study provides a systematic review of TKR demographics and equity factors using the PROGRESS-Plus framework across income levels.
Findings
Most TKR studies focus on high-income countries, with no representation from Africa.
Health equity indicators like socioeconomic status and education are poorly reported in global TKR research.
Abstract
Osteoarthritis (OA) of the knee is a common, disabling condition influenced by multiple biopsychosocial factors and often requiring a total knee replacement (TKR). However, most rehabilitation programmes are developed in high-income countries, potentially limiting transferability to lower-income settings with distinct health equity challenges. This study aimed to describe the demographic and health equity profiles of adults undergoing TKR for primary OA across low-, middle- and high-income countries. A systematic literature search was conducted in PubMed, Scopus, EBSCOhost, Web of Science and ProQuest for peer-reviewed primary research, including observational studies, randomised controlled trials and grey literature published between 2020 and 2024. Studies reporting on individuals undergoing TKR were selected. Data extraction followed the PROGRESS-Plus framework, and a descriptive…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
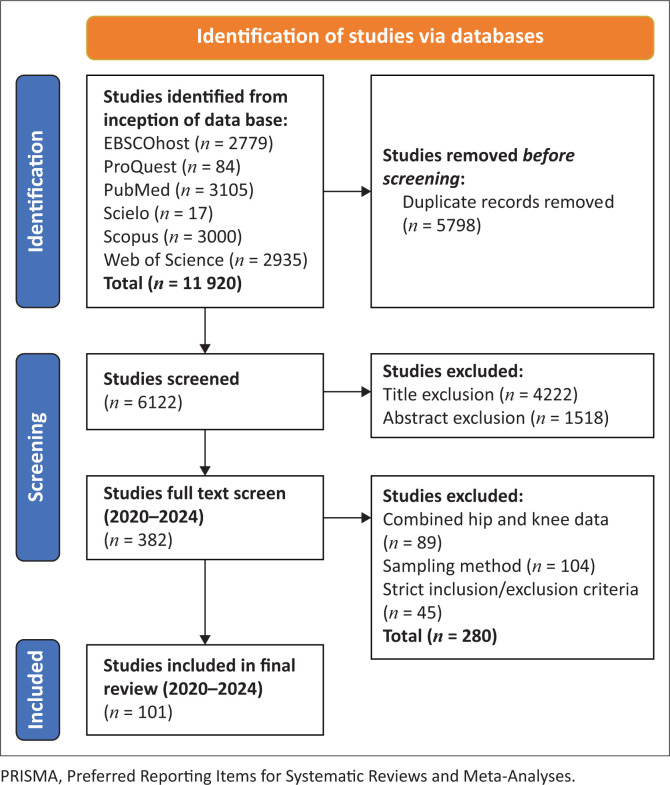 FIGURE 1
FIGURE 1| Category | Inclusion | Exclusion |
|---|---|---|
| Population | Adults | Patellofemoral joint OA |
| Study design | Observational studies (cross-sectional, cohort, case-control designs) | Case studies |
| Recruitment | All participants were included sequentially and/or consecutively | Restricted age range (example, between 50 years and 70 years) |
| Type of information | Studies reporting demographic and social profile information | Data presented as combined for hip and knee |
| Factor | Title in table | Description of data extracted |
|---|---|---|
| Place of residence | Country | Country and income level according to worldbank.org |
| Race or ethnicity | Race | Number of people listed as white |
| Occupation | Occupation | Number of people showed as currently employed or on pension |
| Gender | Gender | Number of female participants |
| Religion | n/a | None of the studies reported in this |
| Education | Education | Number of people having finished secondary education or higher |
| Socioeconomic | SES | Number of people listed as lower on the socioeconomic scale |
| Social capital | Social capital | Number of people listed as married, with a partner or having support |
| Age | Age | Mean age and range |
| Lifestyle | BMI Smoking | Body mass index, mean and s.d. Number of people who are smokers |
| Disability | OA severity | Number of people scoring Level four on the Kellgren–Lawrence scale for radiographic severity of OA |
| Article identifier | Aim | Data source | Study design | Instruments | Country | Income | Sample size |
|---|---|---|---|---|---|---|---|
|
| |||||||
| Heath et al. ( | Describe the pre- and postoperative self-reported health and quality of life status. | National registry | Retrospective cohort | EQ-5D-5L; OKS; KOOS-12 | Australia | High income | 8299 |
| Genel et al. ( | Determine the proportion of TKA and THA patients who use prescribed opioids regularly (daily) before surgery (i.e. opioid use reported between the time of waitlisting and any time up to 3 months before surgery). | National and regional registries | Retrospective cohort | OKS; EQ-VAS | Australia | High income | 1187 |
| Johns et al. ( | Determine the relative risk (RR) of having high pain post-op and evaluate the association of high pain on function. | Public and private hospital databases | Retrospective cohort | OKS; EQ-VAS | Australia | High income | 718 |
| Liu et al. ( | Determine mental health before TKA, preoperative psychological intervention would be necessary. | Hospital database | Prospective observational | WOMAC; SF-36 | China | Upper middle income | 532 |
| Wang et al. ( | Assess if the educational level of patients will affect the functional recovery after total knee arthroplasty (TKA). | Hospital database | Retrospective cohort | HSS; WOMAC; SF-12 | China | Upper middle income | 334 |
| Bian et al. ( | Examine the prevalence of preoperative psychological distress and its influences on patient satisfaction and function after TKA. | Hospital database | Prospective cohort | KSS | China | Upper middle income | 210 |
| Liu et al. ( | Assess the prevalence of patient satisfaction after TKA and the roles of different scales in measuring overall patient satisfaction. | Hospital database | Retrospective cohort | WOMAC; KSS; (SF)-12 | China | Upper middle income | 545 |
| Chan et al. ( | Determine the prevalence of prediabetes and diabetes in patients who underwent TKA and whether universal HbA1c screening and glycaemic control affected the rate of PJI after TKA. | Hospital database | Cross-sectional | - | Hong Kong SAR, China | High income/ upper middle income (China) | 1566 |
| Tanaka et al. ( | To determine if self-reported physical activity was related to muscle strength and walking ability in patients with knee osteoarthritis awaiting total knee arthroplasty. | Hospital databases | Cross-sectional | - | Japan | High income | 767 |
| Hasegawa et al. ( | To evaluate the presence of neuropathic pain in the knees of OA patients using the painDETECT questionnaire (PDQ). | Hospital database | Prospective cohort | - | Japan | High income | 158 |
| Tobinaga et al. ( | Examined the impact of physical activity SE on health-related quality of life (HRQOL) alongside other factors. | Hospital database | Cross-sectional | WOMAC; SF-36v2 | Japan | High income | 106 |
| Nagira et al. ( | Explore the trends in patient characteristics and implant survivorship (IS) for primary total knee arthroplasty (TKA) over the past three decades. | Hospital database | Retrospective cohort | - | Japan | High income | 307 |
| Choi et al. ( | Investigate the association of factors for OA-induced knee pain in Taiwanese patients who received total knee replacements (TKRs). | Hospital database | Retrospective cross-sectional | - | Korea, Rep. | High income | 158 |
| Sook Joung et al. ( | Identify preoperative physical performance factors that predict stair-climbing ability at 1 month after total knee arthroplasty. | Hospital database | Prospective cohort | WOMAC; EQ-5D | Korea, Rep. | High income | 213 |
| Sauder et al. ( | Investigate differences in patient demographics between centres in the United States, Scandinavia and South Korea for patients undergoing primary TKA. | Hospital databases | Cross-sectional | KOOS | Korea, Rep. | High income | 100 |
| Kim et al. ( | To determine the effect of comorbidities on the physical function and quality of life of patients at 3 months after total knee arthroplasty. | Hospital database | Retrospective cohort | WOMAC; EQ-5D | Korea, Rep. | High income | 140 |
| Baek et al. ( | Investigated the prevalence of adrenal insufficiency among patients in Korea admitted for TKA. | Hospital database | Prospective cross-sectional | - | Korea, Rep. | High income | 200 |
| Shon, Kim and Jo ( | Compare sex differences in the incidence of sarcopenia in patients undergoing TKA for advanced knee osteoarthritis (OA). | Hospital database | Retrospective comparative | KOOS; WOMAC; (SF)-12 | Korea, Rep. | High income | 892 |
| Snell et al. ( | Examined associations between self-reported and clinician-assessed comorbidity and quality of life (QOL) outcomes after hip and knee replacement. | National registry | Cross-sectional | EUROHIS-QOL; OKS | New Zealand | High income | 214 |
| Dumlao et al. ( | Describe the demographics, clinical profiles and outcomes of arthroplasty patients. | Hospital database | Descriptive and retrospective review | - | Philippines | Lower middle income | 111 |
| Zhang et al. ( | Compare the predictive performance of machine learning (ML) algorithms and preoperative PROM thresholds in predicting minimal clinically important difference (MCID) attainment at 2 years after TKA. | National registry | Prospective cohort | WOMAC; SF-36 | Singapore | High income | 2840 |
| Sim et al. ( | Evaluate the impact on knee function and quality of life of patients who had their planned TKA postponed because of the pandemic. | Hospital database | Retrospective review | KSFS; KSS; OKS; SF-36 | Singapore | High income | 160 |
| Chio et al. ( | Investigate the association factors for OA-induced knee pain in Taiwanese patients who received total knee replacements (TKRs). | Hospital database | Retrospective cohort | - | Taiwan, China | High income | 357 |
|
| |||||||
| Neuprez et al. ( | Determine if benefits observed during the first year were maintained or improved over time and to clarify their determinants. | Hospital database | Prospective cohort | SF-36; WOMAC; EQ-VAS; EQ-5D | Belgium | High income | 280 |
| El-Galaly et al. ( | Can a clinically meaningful model be built on the preoperative factors included in the Danish Knee Arthroplasty Registry. | National registry | Retrospective review | KSS; | Denmark | High income | 25 104 |
| Justesen et al. ( | Investigate whether intraoperative contamination results in lower patient-reported outcomes (PRO) for patients. | Hospital databases | Prospective cohort | OKS; FJS; EQ-5D-5L; EQ-VAS | Denmark | High income | 630 |
| Larsen et al. ( | Assess the changes in pain intensity and functional capacity in patients with post-surgical complications after 3 weeks of rehabilitation. | Hospital database | Retrospective cohort | KOOS; | Denmark | High income | 166 |
| Sauder et al. ( | Investigate differences in patient demographics between centres in the United States, Scandinavia and South Korea for patients undergoing primary TKA. | Hospital databases | Cross-sectional | KOOS | Denmark | High income | 169 |
| Bradbury et al. ( | Compare outcomes between RPT and OPT in patients undergoing SDD 36 TKA. | Hospital database | RCT | VR-12; KOOS, Jr; | Georgia | Upper middle income | 197 |
| Green, Walsh and Al-Dadah ( | Compare the clinic outcomes of THR and TKR using a comprehensive range of patient-reported outcome measures (PROMs). | Hospital database | Prospective longitudinal observational | EQ-5D; SF-12; WOMAC; KOOS; OKS | Germany | High income | 63 |
| Siviero et al. ( | Investigate patient QOL at the time of knee replacement surgery and 3 months later, identify the baseline predictors of change in QOL. | Hospital database | Prospective observational | - | Italy | High income | 151 |
| Harmsen et al. ( | Evaluate the anticipation and the fulfilment of sexual activity after TKA in men and women and identify prognostic factors. | Hospital databases | Prospective cohort | KOOS; SF-12; EQ-5D; EQ_VAS | The Netherlands | High income | 866 |
| Hafkamp et al. ( | Examine the relationship between physicians’ expectations patients’ expectations and primary outcome measures. | Hospital database | Prospective cohort | HSS-KRES; KOOS | The Netherlands | High income | 190 |
| Hafkamp et al. ( | Identify and characterise different subgroups of osteoarthritis patients with respect to the amount and level of expectations. | Hospital database | Prospective cohort | HSS-KRES; KOOS | The Netherlands | High income | 156 |
| Tolk et al. ( | Analyse the relationship between preoperative factors and preoperative outcome expectations in TKA patients. | Hospital database | Cross-sectional | KOOS-PS; OKS; HSS-KRES; EQ-5D; EQ-VAS | The Netherlands | High income | 204 |
| Hafkamp et al. ( | Examine different trajectories of physical symptoms in patients with preoperative anxiety and depressive symptoms. | Hospital database | Prospective cohort | WOMAC; KOOS | The Netherlands | High income | 186 |
| Van Egmond et al. ( | Distinguish specific recovery patterns using the Oxford knee score (OKS) to explore predictors of less favourable recovery patterns. | National registry | Descriptive retrospective | OKS; EQ-5D | The Netherlands | High income | 809 |
| Leichtenberg et al. ( | Investigate if OA-associated pain, functional limitations and QoL are associated with objectively measured physical activity in patients with end-stage hip/knee OA. | Hospital database | Cross-sectional cohort | SF12; KOOS | The Netherlands | High income | 48 |
| Hoelen et al. ( | Determine the association between socioeconomic status (SES) and patient-reported outcome measures. | National registry | Retrospective review | KOOS-PS; EQ-5D-3L; EQ-VAS | The Netherlands | High income | 78 811 |
| Lindberg et al. ( | Identify subgroups of patients with distinct chronic pain profiles following TKA and identified preoperative characteristics associated with these profiles. | Hospital database | Longitudinal cohort | - | Norway | High income | 202 |
| Getachew et al. ( | Test the hypothesis that the co-occurrence of high symptom levels prior to surgery is a risk factor for pain 12 months after TKA. | Hospital database | Longitudinal cohort | - | Norway | High income | 202 |
| Lindberg et al. ( | Identify subgroups of patients with distinct pain profiles for 12 months following TKA. | Hospital database | Longitudinal cohort | - | Norway | High income | 245 |
| Kocic et al. (2020) | Evaluate patients’ perception of function and physical and mental dimensions of health-related quality of life (HRQoL). | Hospital database | Cross-sectional | OKS; SF-36v2 | Serbia | Upper middle income | 100 |
| Jiménez Ortiz et al. ( | Analyse the influence of preoperative anxiety and depression on TKA outcomes. | Hospital database | Longitudinal observational prospective | WOMAC; KSS | Spain | High income | 260 |
| Dursteler et al. ( | Investigate whether preoperative CPM can predict persistent pain after KR surgery | Hospital database | Retrospective cohort | WOMAC; SF-36 | Spain | High income | 146 |
| Sebastia- Forcada et al. ( | Assess clinically important differences in functional outcome over 10 years after primary total knee arthroplasty. | Hospital database | Prospective observational cohort | WOMAC; KSS; (SF)-12 | Spain | High income | 309 |
| Berg et al. ( | Study the influence of fast-track programmes on patient-reported outcomes (PROs) 1 year after surgery. | National registry | Retrospective cohort | EQ-5D; EQ VAS; KOOS | Sweden | High income | 8393 |
| Mahdi, Halleberg-Nyman and Wretenberg ( | Investigate the prevalence of symptom improvement among patients with preoperative anxiety and/or depression. | National registry | Prospective cohort | KOOS; EQ-5D-3L | Sweden | High income | 458 |
| Mahdi, Halleberg-Nyman and Wretenberg ( | Investigate changes in the prevalence of anxiety and depression 1 year after primary TKA. | Hospital database | Prospective cohort | KOOS; EQ-5D-3L | Sweden | High income | 403 |
| Giesinger et al. ( | Comparison of pre-surgery patient characteristics (sex, age, BMI, comorbidity), health status and joint awareness. | National registry | Retrospective analysis | FJS-12; EQ-5D-3L | Switzerland | High income | 2075 |
| Huber et al. ( | Differences in the suitability for KA between different knee morphotypes and the differences between a true KA and an rKA in terms of alignment. | Hospital database | Retrospective review | KOOS; KSS; OKS, EQ-5D | Switzerland | High income | 111 |
| Giesinger et al. ( | Investigate the impact of body mass index (BMI) on improvement in pain, function and general health status following total knee arthroplasty. | Hospital database | Retrospective analysis | WOMAC; EQ-5D-3L | Switzerland | High income | 1565 |
| Vogel et al. ( | Evaluate the responsiveness of different patient-reported outcome measures in patients with primary total knee arthroplasty. | Hospital database | Prospective observational | KSS; KOOS; FJS-12; EQ-5D-3L | Switzerland | High income | 309 |
| Vogel et al. ( | Correlation of preoperative patient expectations with postoperative satisfaction, patient characteristics or patient-reported outcome measures. | Hospital database | Retrospective observational | HSSK-RES; EQ-5D-3L; EQ-VAS | Switzerland | High income | 193 |
| Kaya et al. ( | Determine the relationship between preoperative knee joint function and postoperative QoL in patients undergoing primary TKA. | Hospital database | Cross-sectional descriptive | OKS; EQ-5D-5L; EQ-VAS | Turkey | Upper middle income | 208 |
| Clement et al. ( | Assess a clinically important change in the Oxford knee score (OKS) between one and 2 years postarthroplasty, and identify predictors of change. | Hospital database | Retrospective cohort | OKS; EQ-5D | United Kingdom | High income | 5857 |
| Giesinger et al. ( | Comparison of pre-surgery patient characteristics (sex, age, BMI, comorbidity), health status and joint awareness. | National registry | Retrospective analysis | FJS-12; EQ-5D-3L | United Kingdom | High income | 994 |
| Ramaskandhan et al. ( | Study the 1-, 3-\ and 5-year outcomes of TAR in comparison with the THR and TKR outcomes. | Hospital database | Prospective cohort | WOMAC; SF-36 | United Kingdom | High income | 3520 |
| Evans et al. ( | Describe the association of BMI at the time of surgery with revision after 10 years, 90-day mortality and patient-reported outcomes 6 months following primary. | National registry | Observational retrospective cohort | OKS | United Kingdom | High income | 490 351 |
| Mohammad, Judge and Murray ( | Compared the functional outcomes and quality of life of matched TKRs and UKRs, both overall and in different age groups, using data from 3 national datasets. | National registries | Retrospective observational | OKS; EQ-5D | United Kingdom | High income | 254 355 |
| Ramaskandhan et al. ( | Evaluate PROMs only and does not include clinical, radiographic or adverse event outcomes from surgery. | Hospital database | Prospective | SF-36; WOMAC | United Kingdom | High income | 2475 |
| Scott et al. ( | Determine association of radiographic severity, extent or pattern of knee OA with pain and function before total knee arthroplasty (TKA) or improvement therein 1 year after TKA. | Hospital database | Cross-sectional | OKS; EQ-5D-3L | United Kingdom | High income | 259 |
| Fabiano et al. ( | Exploratory analysis to examine how physical activity and HRQoL evolve in a defined cohort of patients with post-operative chronic pain over the initial 12 months post-TKR period. | Hospital database | Secondary to a randomised controlled trial | OKS-PS; EQ-5D-5L | United Kingdom | High income | 83 |
|
| |||||||
| Moghtadaei et al. ( | Investigate the influence of psychological status and physical and mental health on the outcome of patients undergoing TKA. | Hospital database | Prospective cross-sectional | SF-12; KOOS | Iran, Islamic Rep. | Upper middle income | 52 |
| Al-Otaibi ( | Analyse and discuss patient characteristics and their outcomes in the Abha region of Southwestern Saudi Arabia. | Hospital database | Cross-sectional | KSS | Saudi Arabia | High income | 420 |
| Alomran ( | To investigate the QOL and overall satisfaction post TKA. | Hospital database | Retrospective review | WOMAC; SF-36 | Saudi Arabia | High income | 200 |
|
| |||||||
| King et al. ( | Assess prior use of core recommended non-surgical treatment among patients with knee osteoarthritis (OA) scheduled for total knee arthroplasty (TKA). | Regional registry | Cross-sectional prospective cohort | WOMAC; KOOS-PS | Canada | High income | 2277 |
| King et al. ( | Assessed the association between comorbidity and use of recommended OA therapies with current opioid use. | Regional registry | Cross-sectional prospective cohort | WOMAC; KOOS-PS | Canada | High income | 2769 |
| Lebedeva et al. ( | Evaluate resource use, costs and health-related quality of life (HRQoL) across the continuum of care for patients with knee OA. | Hospital database | Prospective cohort | WOMAC; SF-12; EQ-5D-5L | Canada | High income | 119 |
| Perruccio et al. ( | Investigate whether sex modified the influence of presurgery characteristics on post-TKA knee pain. | Hospital database | Prospective | KOOS-PS | Canada | High income | 477 |
| Costello et al. ( | Discover associations between a number of demographic, anthropological, epidemiological and medical factors and non-responders to TJR. | Regional registry | Prospective cohort | WOMAC | Canada | High income | 416 |
| Baghbani- Naghadehi et al. ( | Evaluate the association between BMI, patient-reported outcome measures (PROMs) preoperatively, and 3 and 12 months postoperatively. | Regional registry | Retrospective secondary analysis | WOMAC; EQ-5D | Canada | High income | 7714 |
| Christensen et al. ( | Identify which patient characteristics are related to gait mechanics in the surgical limb during walking post-TKA. | Hospital database | Cross-sectional | KOS-ADL | United States | High income | 191 |
| Anastasio et al. ( | Investigate potentially modifiable risk factors affecting LOS, with a focus on opioid use. | Hospital database | Cross-sectional | - | United States | High income | 1033 |
| Kunze et al. ( | Develop machine learning algorithms to predict dissatisfaction after TKA. | Hospital database | Retrospective review | PRHS; KSS | United States | High income | 430 |
| Lange et al. ( | Identify specific and disparate trajectories of PROs in the first year following TKA and correlate with patient characteristics. | Hospital database | Prospectivecohort | SF-36; KOOS | United States | High income | 656 |
| Lopez-Olivo et al. ( | Evaluate the association of preoperative psychosocial and demographic factors with total knee arthroplasty (TKA) outcomes. | Hospital database | Prospectivecohort | WOMAC; SF-36 | United States | High income | 178 |
| Riddle ( | Examine osteoarthritis and symptom severity profiles of index versus contralateral knees of persons preparing for KA. | Hospital database | Cross-sectional | WOMAC | United States | High income | 362 |
| Sauder et al. ( | Investigate differences in patient demographics between centres in the United States, Scandinavia and South Korea for patients undergoing primary TKA. | Hospital databases | Cross-sectional | KOOS | United States | High income | 129 |
| Haffar et al. ( | Investigate the relationship between patient resilience, mental health and functional outcomes, and satisfaction up to 2 years after primary unilateral TKA. | Hospital database | Prospectivecohort | KOOS, Jr.; KSS; VR-12 | United States | High income | 86 |
| Johnson et al. ( | Document the nationwide trends in age and obesity in primary THA and TKA throughout the obesity epidemic. | Hospital database | Retrospective analysis | - | United States | High income | 1 556 651 |
| Melnic et al. ( | Investigate the relationship between patient-reported mental health and postoperative physical function following TKA. | Hospital databases | Retrospectivereview | KOOS-PS | United States | High income | 1392 |
| Sideris et al. ( | Analyse the relationship between persistent postoperative pain scores and perioperative cytokine levels in patients undergoing unilateral TKA. | Hospital database | Prospective cohort | - | United States | High income | 162 |
| Emara et al. ( | Test the association of preoperative overdose risk score with postoperative health care use. | Hospital database | Prospective cohort | - | United States | High income | 4326 |
| Dugdale et al. ( | Learn more about real-world patient experiences in returning to driving after total knee arthroplasty. | Regional registries | Retrospectivereview | - | United States | High income | 541 |
| Darrith et al. ( | Determine which patient demographic factors influence the postoperative Patient-Reported Outcomes Measurement Information System (PROMIS) Global Health (GH) scores. | Hospital database | Retrospectivecohort | KOOS-JR | United States | High income | 872 |
| Katakam et al. ( | Assess the association between body mass index (BMI) and failure to achieve the 1-year Knee Disability and Osteoarthritis Outcome Score-Physical Function Short Form (KOOS-PS). | Regional registries | Retrospectivereview | KOOS-PS | United States | High income | 1059 |
| Held et al. (2022) | Investigate perioperative outcomes, complications and early patient-reported outcome measures (PROMs) of one imageless RA-TKA system compared to conventional. | Hospital database | Retrospectivecohort | KSS-FS; WOMAC; SF-12 | United States | High income | 221 |
| Kugelman et al. ( | Understand the use of opioids during the acute post-surgical episode following TJA. | Hospital database | Retrospectivereview | - | United States | High income | 5784 |
| Zhai et al. (2023) | Determine overall 30-day mortality rate for unilateral primary elective TKA patients, stratified by age, comorbidities and preoperative diagnosis. | Hospital database | Retrospective analysis | - | United States | High income | 325 837 |
| Spiering et al. ( | Assess the responsiveness and determine the minimally important difference of 2 patient-reported outcome measures (PROMs) in patients after TKA. | Hospital database | Retrospectivecohort | KOOS-JR; PROMIS | United States | High income | 1315 |
| Gebauer et al. ( | Is baseline depression diagnosis associated with the likelihood of and time to TKA. | Regional registries | Retrospectivecohort | - | United States | High income | 9466 |
| Rechenmacher et al. ( | Examine the impacts of preoperative weight loss on patient-reported and adverse outcomes among TKA patients. | Hospital database | Retrospective analysis | PROMIS | United States | High income | 90 |
| Blackburn et al. ( | Determine the 1-year postoperative factors, specifically patient-reported outcome measures (PROMs) that were associated with 3-year and 5-year postoperative satisfaction. | Hospital database | Retrospectivereview | - | United States | High income | 404 |
| Benes et al. ( | Determine 1-year postoperative factors associated with 3-year and 5-year postoperative satisfaction. | National registries | Retrospectivereview | KOOS; EQ-5D-3L; EQ-5D-VAS | United States | High income | 270 |
| Albright et al. ( | Determine if Knee Injury and Osteoarthritis Outcome Score Joint Replacement (KOOS-JR) MCID values varied among patients undergoing TKA based on patient-specific factors. | Hospital databases | Retrospective review | KOOS-JR; PROMIS | United States | High income | 976 |
| Rahman et al. ( | Investigate the relationship between outcomes following total knee arthroplasty (TKA) and both the Social Vulnerability Index (SVI) and the Area Deprivation Index (ADI). | Regional registry | Retrospective review | KOOS, JR | United States | High income | 19 321 |
| Zheng et al. ( | Explore adding a single variable, the preoperative PROM score, to the CMS-Yale model would improve its ability to predict TKA success. | Hospital database | Prospective cohort | KOOS, JR; SF-36MCS | United States | High income | 5958 |
| Kop et al. ( | Determine the prevalence of contralateral joint OA for patients presenting for unilateral total knee (TKA). | Hospital database | Retrospective review | - | United States | High income | 933 |
| Jabbouri et al. ( | This study evaluates trends of cemented versus press-fit total knee arthroplasty (TKA). | National registry | Retrospective review | - | United States | High income | 348 282 |
|
| |||||||
| Devasenapathy et al. ( | Compare impairments, activity limitation and participation restriction between men and women scheduled for TKA. | Hospital database | Cross-sectional analysis | KOOS; LEAS; LLDI | India | Lower middle income | 240 |
| Chhaya et al. ( | Evaluate the quality-of-life following physiotherapy management in patients with total knee replacement. | Hospital database | Cross-sectional | EQ-5D; KOOS | India | Lower middle income | 11 |
| Bakshi et al. ( | Assess the HRQOL outcome after TKR in patients with knee osteoarthritis (OA). | Hospital database | Longitudinal cohort | KOOS | India | Lower middle income | 56 |
| Chaudhary et al. ( | Assess early functional and clinical outcomes of TKA by analysing post-operative mechanical axis and Knee Society Score (KSS) data. | Hospital database | Prospective observational | KSS | India | Lower middle income | 40 |
| Country | Number of studies | Sample total ( | Age (years) (Mean range) | Gender Female | Race | Occupation | Occupation | Education | SES | Social capital | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
| % |
| % |
| % |
| % |
| % |
| % |
| % | ||||
|
| |||||||||||||||||
| Australia | 3 | 10 204 | 67–68.5 | 5853 | 57.4 | - | - | - | - | - | - | - | - | - | - | - | - |
| Belgium | 1 | 280 | 66.7 | 152 | 54.0 | - | - | - | - | - | - | 165 | - | - | - | - | - |
| Canada | 6 | 13 772 | 65.4–66.9 | 7104 | 51.6 | - | - | 33 | 27.7 | 75 | 63.0 | 555 | 24.0 | 643 | 26.8 | 95 | 80.0 |
| Denmark | 4 | 26 069 | 64–68 | 15 578 | 59.76 | - | - | - | - | - | - | - | - | - | - | - | - |
| Germany | 1 | 63 | 72.1 | 41 | 65.0 | - | - | - | - | - | - | - | - | - | - | - | - |
| Hong Kong | 1 | 1566 | 68–69 | 1170 | 75.0 | - | - | - | - | - | - | - | - | - | - | - | - |
| Italy | 1 | 151 | 67.9 | 97 | 64.0 | - | - | - | - | - | - | 46 | 30.0 | - | - | - | - |
| Japan | 4 | 1338 | 73.6–74.9 | 1112 | 83.2 | - | - | - | - | - | - | - | - | - | - | - | - |
| Korea | 6 | 1703 | 68–72.8 | 1357 | 79.7 | - | - | - | - | - | - | - | - | - | - | - | - |
| The Netherlands | 8 | 81 270 | 65–70 | 50 843 | 62.6 | - | - | 127 | 21.9 | - | - | 357 | 65.4 | - | - | 768 | 73.0 |
| New Zealand | 1 | 214 | 68.5 | 101 | 47.0 | 185 | 86.0 | - | - | - | - | - | - | - | - | - | |
| Norway | 3 | 649 | 68–68.3 | 409 | 63.0 | 202 | 100.0 | 259 | 57.9 | - | - | 325 | 50.1 | - | - | 407 | 62.7 |
| Saudi-Arabia | 2 | 620 | 62.7–69.5 | 498 | 80.3 | - | - | - | - | - | - | - | - | - | - | - | |
| Singapore | 2 | 3000 | 66.3–68 | 2115 | 70.5 | - | - | - | - | - | - | - | 1988 | 66.3 | - | - | |
| Spain | 3 | 715 | 69.2–73.1 | 497 | 69.5 | - | - | - | - | - | - | - | - | - | - | - | |
| Sweden | 3 | 9254 | 69–70 | 5250 | 56.7 | - | - | - | - | - | - | - | - | - | - | - | |
| Switzerland | 5 | 4253 | 68–69.3 | 2723 | 63.9 | 1676 | 100.0 | 293 | 18.7 | 730 | 46.7 | 1537 | 98.0 | - | - | - | - |
| Taiwan | 1 | 357 | 71 | 282 | 79.0 | - | - | - | - | - | - | - | - | - | - | - | - |
| UK | 9 | 757 945 | 66.8–70.3 | 434 350 | 57.3 | 243 452 | 96.0 | - | - | - | - | - | - | - | - | - | |
| US | 29 | 2 287 146 | 63–69.5 | 1 405 929 | 61.5 | 1 852 834 | 81.2 | 77 | 43.3 | 85 | 47.8 | 753 | 68.2 | 3801 | 17.7 | 1283 | 68.7 |
|
| |||||||||||||||||
| China | 5 | 1699 | 65.3–75.5 | 1338 | 78.8 | - | - | - | - | - | - | 167 | 50.0 | - | - | 197 | 94.0 |
| Georgia | 1 | 197 | 70.2 | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
| Iran | 1 | 52 | 67.2 | 37 | 73.0 | - | - | - | - | - | - | - | - | - | - | - | - |
| Serbia | 1 | 100 | 69.4 | 69 | 69.0 | - | - | 6 | 6.0 | 69 | 69.0 | - | - | - | - | 94 | 94.0 |
| Turkey | 1 | 208 | 65.7 | 179 | 86.0 | - | - | 8 | 4.0 | - | - | 22 | 10.6 | - | - | 162 | 78.0 |
|
| |||||||||||||||||
| India | 4 | 347 | 58.9–65.6 | 236 | 68.0 | - | - | 47 | 20.0 | - | - | 105 | 43.8 | - | - | 101 | 42.1 |
| Philippines | 1 | 111 | 64.5 | 93 | 84.0 | - | - | - | - | - | - | - | - | - | - | - | - |
| Country | Number of studies | Smoking Yes | BMI(Mean range) | OA severity KL IV | ASA II | ASA III | Previous surgery | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
| % |
| % |
| % |
| % |
| % | |||
|
| ||||||||||||
| Australia | 3 | - | - | 32.5 | - | - | 4443 | 53.5 | 3379 | 40.7 | - | - |
| Belgium | 1 | - | - | 29.3 | 30 | 10.7 | - | - | - | - | 97 | 34.6 |
| Canada | 6 | 177 | 6.4 | 30.7–34.9 | - | - | - | - | - | - | - | - |
| Denmark | 4 | - | - | 28.9–29.5 | 42 | 24.9 | - | - | - | - | 5421 | 21.6 |
| Germany | 1 | - | - | 30.4 | - | - | - | - | - | - | - | - |
| Hong Kong | 1 | - | - | 27.1–28.4 | - | - | - | - | - | - | - | - |
| Italy | 1 | 17 | 11.3 | 28.7 | - | - | - | - | - | - | - | - |
| Japan | 4 | - | - | 25.6–27.2 | 575 | 62.2 | - | - | - | - | - | - |
| Korea | 6 | 76 | 8.5 | 25.6–27.1 | 1014 | 67.5 | 161 | 80.5 | 33 | 16.5 | - | - |
| The Netherlands | 8 | 6278 | 7.9 | 29–30.6 | 177 | 86.8 | 52 511 | 66.6 | 16 462 | 20.9 | - | - |
| New Zealand | 1 | - | - | 30.1 | - | - | 147 | 68.7 | 40 | 18.7 | - | - |
| Norway | 3 | - | - | 28–29.4 | - | - | - | - | - | - | - | - |
| Saudi Arabia | 2 | - | - | 28.4–29.4 | - | - | - | - | - | - | - | - |
| Singapore | 2 | - | - | 27.3–28 | - | - | - | - | - | - | - | - |
| Spain | 3 | - | - | 30.8–31.2 | - | - | - | - | - | - | - | - |
| Sweden | 3 | - | - | 28.8–29 | - | - | 565 | 65.6 | 72 | 8.3 | - | - |
| Switzerland | 5 | 269 | 17.2 | 29.6 | 394 | 78.5 | 378 | 75.3 | 92 | 10.3 | 61 | 55.0 |
| Taiwan | 1 | 20 | 5.6 | 28 | 152 | 42.6 | - | - | - | - | - | - |
| UK | 9 | 3 | 5 | 27.9–30.9 | 142 | 54.8 | 552 926 | 74.2 | 123 259 | 16.6 | - | - |
| USA | 29 | 2241 | 8.3 | 29.8–36.7 | 246 | 50.1 | 12 016 | 42.5 | 15 179 | 53.7 | 66 | 40.7 |
|
| ||||||||||||
| China | 5 | - | - | 23.5–30 | - | - | 304 | 73.8 | 53 | 12.9 | - | - |
| Georgia | 1 | - | - | 30.2 | - | - | 61 | - | 39 | 19.8 | - | - |
| Iran | 1 | - | - | - | - | - | - | - | - | - | - | - |
| Serbia | 1 | - | - | 29 | - | - | - | - | - | - | - | - |
| Turkey | 1 | 3 | 1.4 | 32.1 | - | - | - | - | - | - | - | - |
|
| ||||||||||||
| India | 4 | - | - | 28.7 | - | - | - | - | - | - | - | - |
| Philippines | 1 | - | - | - | - | - | - | - | - | - | - | - |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTotal Knee Arthroplasty Outcomes · Osteoarthritis Treatment and Mechanisms · Knee injuries and reconstruction techniques
Introduction
Osteoarthritis (OA) most frequently affects the knee joint. While its estimated global prevalence is 22% in individuals over 40 years of age (Cui et al. 2020), the condition predominantly impacts older adults, and its global, regional and national burden continues to rise significantly, with analyses projecting this burden to 2050 (Steinmetz et al. 2023).
Furthermore, the burden of OA is escalating, particularly among postmenopausal women globally. The classification of knee OA is typically demarcated into two main categories: primary OA, which lacks a clear causal factor for articular degeneration, and secondary OA, which is associated with specific factors such as joint trauma (e.g. previous fractures, ligament and meniscus injuries) or inflammatory conditions such as rheumatoid arthritis (Hsu & Silwec 2023).
The risk factors for the development of primary knee OA include age, gender, genetics, increased body mass index (BMI), physical activity levels and occupational demands (Cui et al. 2020). Additionally, factors that affect both the clinical progression (level of pain, functional ability) and the structural progression of knee OA also include socioeconomic indicators (e.g. level of education and social class), psychological factors (coping, mechanisms, anxiety, depressive states) and the presence of comorbidities (Bastick et al. 2016; Chen et al. 2025; Deveza, Loeser & Katz 2017; Li et al. 2024; Silverwood et al. 2015; Swinnen et al. 2021). Many of these risk factors are interconnected within the social context of the individual, and in conjunction with personal factors, community perceptions and psychological influences, they exert a considerable influence on the health-related outcomes for individuals presenting with knee OA (Luong, Lohmander & Sowers 2012). An important aspect of managing primary knee OA is the identification of modifiable risk factors, as these can be more effectively addressed through targeted interventions (Georgiev & Angelo 2019).
Given the complex and diverse presentation of knee OA, management strategies should consider the individual within their biopsychosocial context. However, a significant limitation is that data exploring risk factors, social determinants and progression trajectories primarily come from high-income countries (HICs). These data may not accurately reflect the profiles of individuals experiencing knee OA in low-middle-income countries (LMICs), where a significant proportion of the population faces lower socioeconomic circumstances (Dell’ Isola et al. 2016, 2018; Deveza et al. 2017; Li et al. 2024; Luong et al. 2012; Steinmetz et al. 2023). Existing international OA management interventions are typically designed for HIC contexts and may therefore not be generalisable or transferable to local contexts in LMIC because of health equity differences. Health equity differences may introduce barriers to the implementation of best-evidence OA care such as fragmented healthcare systems, inadequate human resources and inexperience among health professionals in managing OA post TKR (Castro et al. 2021; Keller & Sankah 2025).
Evidence suggests that physiotherapy plays a vital role in addressing the complex biopsychosocial factors following a TKR, as physiotherapists possess specialised expertise in understanding the multifaceted contributors to chronic pain and functional limitations (Kohia et al. 2015; Nishimoto et al. 2025). However, the availability and scope of physiotherapy services may vary considerably between high-income and LMICs, potentially creating additional barriers to comprehensive post-TKR rehabilitation.
To develop effective, context-specific programmes, the global demographic profile of individuals with OA should be designed using an equity lens that considers key factors influencing health outcomes. The PROGRESS-Plus equity lens framework is an acronym representing the following key factors: place of residence, race or ethnicity or culture or language, occupation, gender or sex, religion, education, socioeconomic status (SES), social capital, age, disability, sexual orientation and other vulnerable groups (Kavanagh, Oliver & Lorenc 2008). This framework was developed for description and assessment of social determinants related to health equity across populations, offering insights for translating interventions into different contexts (Kavanagh et al. 2008), by including descriptors linked to the variability in health outcomes (O’ Neill et al. 2014).
To the authors’ knowledge, no studies have comprehensively described the global demographic and social profiles of individuals undergoing TKR. An overview of these profiles through an equity-focused lens, such as the PROGRESS-Plus framework, can facilitate the adaptation of existing rehabilitation interventions to diverse local contexts. Therefore, this systematic review aims to describe the demographic characteristics and PROGRESS-Plus profiles of adults undergoing TKR for primary knee OA across low-, middle- and high-income countries. The findings are intended to identify evidence-based interventions and highlight critical gaps in research from lower-income contexts, particularly African settings. This will inform future research priorities and adapted implementation strategies for underrepresented contexts.
Research methods and design
Eligibility criteria
The systematic review used specific criteria for the inclusion of studies, as detailed in Table 1. The eligibility criteria for this systematic review included studies involving adults (≥ 18 years) awaiting or undergoing TKR surgery for primary knee OA. Eligible study designs comprised observational studies (cross-sectional, cohort, case-control) and randomised controlled trials. Studies were required to recruit participants sequentially or consecutively, with minimal age restrictions permissible. Only studies reporting baseline pre-surgical information specific to knee OA were included. To maintain feasibility and relevance, the review was limited to studies published between 2020 and 2024 because of the vast number of publications on the topic. Studies focusing on patellofemoral joint OA, secondary OA because of trauma or primary OA diagnoses not related to TKR individuals were excluded. Case studies and systematic reviews were excluded. Studies with restricted age ranges or those that selectively excluded participants based on factors such as BMI or comorbidities were not considered. Additionally, studies presenting combined hip and knee data, duplicate cohorts or those superseded by a more comprehensive included study were excluded. Studies published outside the specified 5-year period were also excluded to ensure manageability, given the volume of literature.
For the purpose of our review, ‘undergoing Total Knee Replacement (TKR)’ refers to individuals who are either awaiting TKR surgery or have already received the procedure, provided that baseline pre-surgical information is reported. Classification of countries by income group was based on the World Bank’s List of Income Classification of Economies (available at www.worldbank.org/en/home), which categorises economies according to the Atlas Gross National Income (GNI) per capita into four groups: low-income, lower-middle-income, upper-middle-income and high-income countries. Primary OA was defined as articular degeneration occurring without any identifiable underlying cause (Hsu & Siwec 2023). In contrast, secondary OA was considered to result from either abnormal mechanical loading of the joint, such as post-traumatic events, or conditions affecting normal articular cartilage (Hsu & Siwec 2023).
Search strategy
In collaboration with a faculty librarian who was experienced in conducting systematic searches, an initial exploratory search was conducted using the Stellenbosch University online library to identify databases containing relevant peer-reviewed literature, as well as grey literature, including academic theses. The following databases, PubMed (Medline), Scopus (abstracts from Elsevier or other sources), EBSCOhost (Africa Wide, CINAHL, Academic Premier, Health Source Nursing), Web of Science and ProQuest, were accessed for our review. Key search terms were identified by reviewing author keywords and index terms in relevant articles retrieved from PubMed and the Cochrane Library. A full list of these terms is provided in Online Appendix 1 – Table 1-A1, and the specific search strings used for each database are detailed in Online Appendix 1 – Table 2-A1.
Study selection and procedure
Following the database searches outlined in Online Appendix 1 – Table 2-A1, the identified studies were exported as comma-separated values (CSV) files containing the titles and abstracts. These CSV files were imported into the Rayyan Intelligent Systematic Review web-based software (https://www.rayyan.ai/) where automated duplicate detection was performed by the software. After duplicates were removed, the remaining titles were screened using the eligibility criteria. Articles not meeting the criteria based on their titles were excluded, after which the abstracts of the remaining studies were assessed for relevance and potential inclusion. Full-text versions of eligible articles were retrieved for further review by the main author and research assistant, and where conflicts arose, the supervisory team were consulted.
Both the primary researcher and a research assistant independently reviewed the titles, abstracts and full texts according to the eligibility criteria. Upon selection of the final studies, the supervisory team reviewed the articles and the extracted data. Any conflicts were resolved by the supervisory team. Reporting of the review process was done according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 flow diagram for new systematic reviews, which included database and register search results (Page et al. 2021). This flowchart can be seen in Figure 1 in the results section.
Identification of included studies according to the PRISMA 2020 flow diagram for new systematic reviews.
Assessment of reporting quality
Reporting quality of the final list of included studies was assessed using the appropriate study design appraisal tool from the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist (Von Elm et al. 2007) or the JBI Critical Appraisal Checklist for Randomised Controlled Trials (Tufanaru et al. 2020). The focus on assessing the reporting quality of the included studies was prioritised because of the descriptive nature of the data sought and to understand the profile of participants, especially in observational studies, where quality reporting is essential. Because of time constraints, two research assistants were educated on using the STROBE checklist by the primary researcher and conducted the quality of reporting assessment, each taking half of the studies. All uncertainties and queries were resolved by the primary researcher. The STROBE checklist is presented in Online Appendix 1 – Table 3-A1.
Data extraction and management
In addition to the study characteristics (which included title, authors, date of publication, aims and objectives, study design, study setting, sample size and results), the PROGRESS Plus framework was used as a guide to extract the relevant information required for applying an equity lens. This included place of residence, race or ethnicity or culture or language, occupation, gender or sex, religion, education, SES, social capital, age, disability and other vulnerable groups (Dell’Isola & Steultjens 2018). Furthermore, smoking, BMI and severity of OA were also extracted for descriptive purposes. Data were extracted by the main reviewer into a Microsoft Excel spreadsheet for recordkeeping and analysis, and a description of the factors can be seen in Table 2.
Data synthesis and reporting
Basic synthesis of the data was done using the descriptive quantitative information available from the studies. Most of the studies reported the demographic and social data using percentages, averages and ranges. Data are reported in the ranges provided by the studies, and counts were combined as a total and percentages calculated according to the total counts of the combined studies.
Ethical considerations
This systematic review was registered with the International Prospective Register of Systematic Reviews (PROSPERO) (review number 284634 on https://www.crd.york.ac.uk/prospero/) and adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) Statement (Page et al. 2021). Our study was approved by the Stellenbosch University Health and Research Ethics Committee under Ethics number S20/11/315. The protocol was published and can be accessed online on https://hdl.handle.net/10520/ejc-sajp_v78_i1_a1649 (Coetzee et al. 2022).
Results
The systematic review identified a total of 101 studies (Figure 1) from diverse global regions, encompassing East Asia and the Pacific (n = 23), Europe and Central Asia (n = 38), the Middle East (n = 3), North America (n = 33) and South Asia (n = 4). Of these, only five were conducted in lower middle-income countries, specifically the Philippines and India (Bakshi et al. 2021; Chaudhary et al. 2024; Chhaya, Padmashri & Krishnan 2020; Devasenpathy et al. 2020; Dumlao, Delgado & Azores 2020), and nine in upper middle-income countries (Bian et al. 2021; Bradbury et al. 2024; Chan et al. 2020; Kaya, Seyman & Kaya 2024; Kocic et al. 2024; Liu et al. 2020, 2021; Moghtadaei et al. 2020; Wang et al. 2022). The rest were conducted in HICs. No African studies were included. Detailed information regarding the selected articles is presented in Table 3, segmented by geographic region.
Table 4 summarises the PROGRESS-Plus data extracted from the studies, and Table 5 summarises the PLUS factors such as smoking, BMI and severity. When combining the results of different studies for one country, the range of the results is reported. Sample sizes varied widely, ranging from 11 to over 490 000 participants, and the final sample of individuals included in our review is 3 203 292. Australia, Denmark, the United Kingdom (UK) and the United States (US) used large knee replacement databases for their studies and were able to provide retrospective data on basic demographic profiles of their OA population. Most studies employed retrospective or prospective hospital databases and national or regional registries, with a smaller number using cross-sectional, descriptive or longitudinal designs. Common data collection instruments included validated patient-reported outcome measures (PROMs), reflecting a focus on functional recovery, patient satisfaction, mental health, pain and quality of life post-TKR.
Across all income levels, the majority of study participants were female, typically ranging from 54% to 86%. The mean age of participants ranged between 65 years and 75 years. Some variations across countries, such as Georgia, Germany and Japan, which had an older average age than India, which had the youngest cohort. Information on race/ethnicity was limited, with only a few countries reporting data on the percentage of white participants. Data on occupation, education and SES were sparse, particularly for lower-income countries. In HICs, such as Canada, the Netherlands and the US, where data were available, a significant proportion of participants had secondary education or higher (ranging from 24% to 98%) and were employed or receiving pensions. Low SES was reported for 17.7% of participants in the US and 26.8% in Canada. Social capital, measured by the percentage of participants with a partner, was reported only for a few HICs, with the highest percentage (94%) observed in China.
Smoking prevalence was reported for a few HICs, ranging from 5% to 17.2% of participants. Mean BMI tended to be higher in HICs (ranging from 25.6 kg/m^2^ to 36.7 kg/m^2^) compared to upper-middle and lower-middle-income countries (23.5 kg/m to 32.1 kg/m). Osteoarthritis severity, assessed using the Kellgren–Lawrence (KL) grading system, was reported for some HICs. The percentage of participants with severe OA (KL grade IV) ranged from 10.7% in Belgium to 78.5% in Switzerland. American Society of Anaesthesiologists (ASA) physical status classification was reported for several HICs, with a substantial proportion of participants classified as ASA II (ranging from 42.5% in the US to 80.5% in Korea) or ASA III (ranging from 8.3% in Sweden to 53.7% in the US). Previous surgery was reported for a few HICs, with percentages ranging from 34.6% in Belgium to 55% in Switzerland.
Discussion
The purpose of our review was to describe the demographic and health equity profiles of adults undergoing TKR for primary OA in lower, middle- and high-income countries. The review included 101 studies encompassing over 3.2 million individuals and represents the first comprehensive examination of the global demographic and health equity profile of adults undergoing TKR for primary OA through the PROGRESS-Plus equity lens.
Although a substantial volume of published research demonstrates ongoing clinical and academic interest in TKR, the findings show critical geographic biases and equity reporting deficiencies that fundamentally limit the clinical utility of the current evidence base in different contexts.
The concentration of TKR research in high-income and upper-middle-income countries underscores a significant gap in understanding the diverse populations affected by OA. This lack of representation from low-income countries is a significant limitation, as this may affect the generalisability of findings and limit the understanding of how socioeconomic factors influence outcomes in TKR across diverse populations. For example, no African studies met the criteria for inclusion, and this is problematic as the health system-related factors may significantly impact access to and quality of OA care in African contexts. Africa contributes significantly to the increasing global prevalence (estimated more than 37%), unmet needs and treatment burden for people with OA (Steinmetz et al. 2023). Despite the availability of evidence-based practice recommendations for OA management, evidence suggests that the implementation of these guidelines among African health professionals remains poor (Keller & Sankah 2025). Individuals often report a lack of support from clinics, with treatments predominantly focusing on pharmacological management (painkillers) and minimal mention of rehabilitation or pain management (Keller & Sankah 2025). There is an urgent need for a system-wide initiative that prioritises comprehensive, affordable and evidence-based OA care in low-resource settings, including improved education, consistent care pathways and better access to a range of appropriate health professionals and facilities (Owoyemi et al. 2025).
The application of the PROGRESS-Plus framework showed systematic underreporting of social determinants of health across all income levels, although particularly pronounced in lower-income countries. Equity indicators were inconsistently documented, limiting understanding of how these factors shape TKR access, outcomes and recovery trajectories.
This reporting gap is not merely a methodological oversight but represents a fundamental barrier to addressing documented health inequities. Without comprehensive equity data, service planning cannot be appropriately tailored, interventions risk perpetuating existing disparities, and the mechanisms through which social determinants influence clinical outcomes remain unsolved (Rizvi et al. 2022). Data pertaining to occupation, education and SES were particularly scarce, especially in the studies originating from lower-income countries. This is in contrast with the HICs such as Canada, the Netherlands and the US, which reported more comprehensive data on socioeconomic factors such as education and employment status. In these regions, 24% to 98% of participants undergoing TKR had attained secondary education or higher, and the majority of participants were either reemployed or receiving a pension (Ashkenazi et al. 2024). However, low SES was still a concern among this population, with figures indicating that approximately 17.7% of participants in the US and 26.8% in Canada were classified as having low SES. Social capital, which was most commonly defined as the percentage of participants with a partner, was reported in only a few HICs. In the included studies, China exhibited the highest percentage at 94%. This suggests a potential correlation between social support and health outcomes in OA populations (Wylde et al. 2019).
Despite geographic and methodological variation, the demographic profile demonstrated remarkable consistency, showing that individuals awaiting and undergoing TKR comprise 54% – 86% females, with a mean age consistently between 65 years and 75 years. This female predominance aligns with established literature attributing elevated OA burden in postmenopausal women to declining oestrogen levels, age-related degenerative changes and heightened pain sensitivity (Xu et al. 2025). However, this consistency contrasts with the clinical profile heterogeneity, particularly regarding BMI. The tendency towards higher mean BMI in HICs (25.6 kg/m^2^ – 36.7 kg/m^2^) compared with upper-middle and lower-middle-income countries (23.5 kg/m^2^ – 32.1 kg/m^2^) likely reflects differing lifestyle factors, dietary patterns and obesity prevalence (World Health Organization 2023). This variation underscores the necessity for context-specific pre-operative interventions, particularly weight optimisation programmes delivered by physiotherapists. The wide variation in reported severe OA (KL grade IV: 10.7% in Belgium to 78.5% in Switzerland) further suggests differing thresholds for surgical intervention, access barriers or disease progression patterns across settings.
Strengths and limitations
This systematic review is the first review to look at a global profile of individuals undergoing TKR surgery. Furthermore, the use of the PROGRESS-PLUS framework for data extraction in our study underscores an equity lens that may not be consistently applied in other research.
This method of portraying a wider range of the social determinants of health is crucial for understanding health outcomes. It also highlights critical gaps in representation and the need for improved reporting practices in the field. Our study adhered to reporting guidelines, such as STROBE and PRISMA, to ensure clarity and consistency in published studies.
The reporting quality of the final list of included studies was assessed using the appropriate study design appraisal tool from the STROBE, and the PRISMA checklist for reporting systematic reviews was completed and is presented in Online Appendix 1 – Table 4-A1.
Despite the overall large sample size, the limited representation from low-income countries is a significant limitation. The absence of data from these regions restricts our understanding of how socioeconomic factors influence TKR outcomes. Because of the search being limited to studies published after 2020, studies published in Africa may have been missed. In addition, a meta-analysis of the data was not possible because of the heterogeneity in outcome measures used and the reporting methods; therefore, our study could only report on the similarities and differences between countries and reference the range of reported data.
Implications for rehabilitation and physiotherapy
The implications of our review for rehabilitation are significant, particularly with regard to enhancing individualised management and addressing health equity in individuals undergoing TKR. Our study found significant gaps in the reporting and consideration of socioeconomic and equity-related information, especially in LMIC. This highlights the need for rehabilitation professionals involved in the management of individuals undergoing TKR, such as physiotherapists, to include socioeconomic indicators in pre-operative assessment, as this will assist with the tailoring of post-operative support and enhancing in postoperative recovery (Clynes et al. 2019). These indicators could include factors such as income, education and employment status. The reporting of demographic variables is essential to illustrate how social determinants of health influence pain, function and quality-of-life outcomes after TKR and is important to inform equitable service planning in the future management of these individuals (Castro et al. 2021; O’Neill et al. 2014).
In addition, physiotherapists are well positioned to implement recommended pre-operative lifestyle interventions such as education on exercise, weight optimisation and other self-management strategies (Rice et al. 2019). Incorporating interventions into the care pathway could improve postoperative outcomes by addressing modifiable risk factors and preparing individuals for surgery and recovery within their social context. More research within the field of physiotherapy should investigate the efficacy of these pre-operative lifestyle interventions on postoperative outcomes. This could provide insights into how pre-operative health behaviours influence recovery and overall satisfaction with surgical outcomes.
Implications for physiotherapy practice, policy and research
Our review identifies critical evidence gaps with direct implications for physiotherapy practice, health equity, and service delivery for individuals undergoing TKR.
Physiotherapy practice: Equity-informed, biopsychosocial rehabilitation
The substantial underreporting of SES and equity indicators, particularly in LMICs, could potentially impact evidence-informed rehabilitation and patient outcomes for individuals awaiting or undergoing TKR.
Physiotherapists should systematically integrate socioeconomic indicators (income, education, employment status, housing stability) into pre-operative assessments to enable individualised care planning (Clynes et al. 2019). These data constitute essential clinical information, as social determinants fundamentally shape pain experiences, functional recovery and quality-of-life outcomes following TKR (Castro et al. 2021; O’Neill et al. 2014).
The findings highlight the importance of a biopsychosocial, equity-focused rehabilitation approach that explicitly accounts for socioeconomic and cultural contexts, especially in underrepresented LMIC populations, where comorbidity burdens, healthcare access barriers and socioeconomic disadvantage affect post-surgical recovery (Alvarez 2022). The observed higher baseline BMI in HICs reinforces the clinical relevance of weight optimisation, although the absence of African and broader LMIC data prevents assumptions about optimal strategies across diverse contexts.
In addition, the effectiveness of pre-operative physiotherapy interventions on post-TKR outcomes remains inadequately evaluated. Research must rigorously examine how pre-operative health behaviours, delivered within culturally appropriate frameworks, influence recovery, functional outcomes and patient satisfaction across diverse socioeconomic and geographic populations.
Policy implications: Addressing structural inequities
The geographic concentration of evidence reflects systemic research inequities requiring policy intervention. Research funding bodies must prioritise studies in LMICs and underrepresented settings to comprehensively understand TKR outcomes and develop contextually appropriate care pathways. Current evidence cannot support confident translation to populations facing substantially different socioeconomic circumstances and healthcare systems. Standardised reporting of health equity metrics should become mandatory in orthopaedic and rehabilitation research. The PROGRESS-Plus framework (place of residence, race or ethnicity, occupation, gender, religion, education, SES, social capital) provides validated structure for equity-focused data collection (O’Neill et al. 2014). Without such data, equitable service planning remains unattainable. Low-resource settings require system-wide reform where OA care remains fragmented and pharmacologically focused. Policy must support comprehensive, evidence-based care models ensuring equitable access to appropriately trained health professionals, including physiotherapists, and necessary facilities. The disproportionate disability burden in LMIC populations requires coordinated action.
Research priorities
Future studies should prospectively collect comprehensive equity indicators, employ standardised outcome measures and intentionally recruit diverse populations. Only through addressing these methodological imperatives can the evidence base support equitable, effective TKR care globally.
Conclusion
This systematic review of 101 studies (including over 3.2 million individuals) highlights that while abundant research exists on the population of patients awaiting or undergoing TKR, the evidence base remains geographically concentrated in high-income and upper-middle-income countries, with a complete absence of African representation and profound underreporting of health equity indicators across all settings. This limits the generalisability of clinical guidelines to populations with the greatest disability burden from knee OA. Addressing this disparity requires coordinated action from researchers, who should systematically collect and report equity metrics, and policymakers, who should prioritise research funding for lower-income countries and mandate standardised equity reporting. Physiotherapists should adopt biopsychosocial, equity-focused rehabilitation approaches that integrate socioeconomic indicators into clinical assessment and deliver contextually appropriate pre-operative interventions.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Al-Otaibi, M.L., 2021, ‘Total knee replacement at Southwestern Saudi Arabia: A single-center experience’, Journal of Family Medicine & Primary Care 10, 2166–2170. 10.4103/jfmpc.jfmpc_2440_20PMC 828424734322408 · doi ↗ · pubmed ↗
- 2Albright, P., Huyke-Hernandez, F.A., Ormseth, A., Doxey, S.A., Banks, E., Only, A.J. et al., 2024, ‘Preoperative function affects ability to achieve one-year minimum clinically important difference for patients undergoing total knee arthroplasty’, Arthroplast Today 27, 101377. 10.1016/j.artd.2024.10137738654887 PMC 11035092 · doi ↗ · pubmed ↗
- 3Alomran, A.S., 2022, ‘Quality of life post total knee arthroplasty: Saudi Arabian experience’, Annals of African Medicine 21, 158–160. 10.4103/aam.aam_106_2035848649 PMC 9383015 · doi ↗ · pubmed ↗
- 4Alvarez, P.M., Mc Keon, J.F., Spitzer, A.I., Krueger, C.A., Pigott, M., Li, M. et al., 2022, ‘Socioeconomic factors affecting outcomes in total knee and hip arthroplasty: A systematic review on healthcare disparities’, Arthroplasty 4(1), 36. 10.1186/s 42836-022-00137-436184658 PMC 9528115 · doi ↗ · pubmed ↗
- 5Anastasio, A.T., Farley, K.X., Boden, S.D., Bradbury, T.L., Premkumar, A. & Gottschalk, M.B., 2020, ‘Modifiable, postoperative risk factors for delayed discharge following total knee arthroplasty: The influence of hypotension and opioid use’, Journal of Arthroplasty 35, 82–88. 10.1016/j.arth.2019.07.04731500913 PMC 7194191 · doi ↗ · pubmed ↗
- 6Ashkenazi, I., Lawrence, K.W., Kaplan, M., Arshi, A., Rozell, J.C., Schwarzkopf, R. et al., 2024, ‘Demographic and socioeconomic trends of patients undergoing total knee arthroplasty from 2013 to 2022 – An analysis from an urban orthopaedic hospital’, Journal of Arthroplasty 39(9), 2158–2165. 10.1016/j.arth.2024.04.02938614359 · doi ↗ · pubmed ↗
- 7Baek, S.W., Noh, J.H. & Heo, Y.S., 2024, ‘Prevalence of adrenal insufficiency in Korean patients undergoing total knee arthroplasty’, Annals of Geriatric Medicine and Research 28, 20–26. 10.4235/agmr.23.012337984965 PMC 10982440 · doi ↗ · pubmed ↗
- 8Baghbani-Naghadehi, F., Armijo-Olivo, S., Prado, C.M., Gramlich, L. & Woodhouse, L.J., 2022, ‘Does obesity affect patient-reported outcomes following total knee arthroplasty?’ BMC Musculoskeletal Disorders 23, 55. 10.1186/s 12891-022-04997-435039019 PMC 8764810 · doi ↗ · pubmed ↗