Chordae tendineae rupture during a helix-fixation leadless pacemaker implantation
Tomoki Fukui, Miwa Miyoshi, Nobuyuki Ogasawara

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
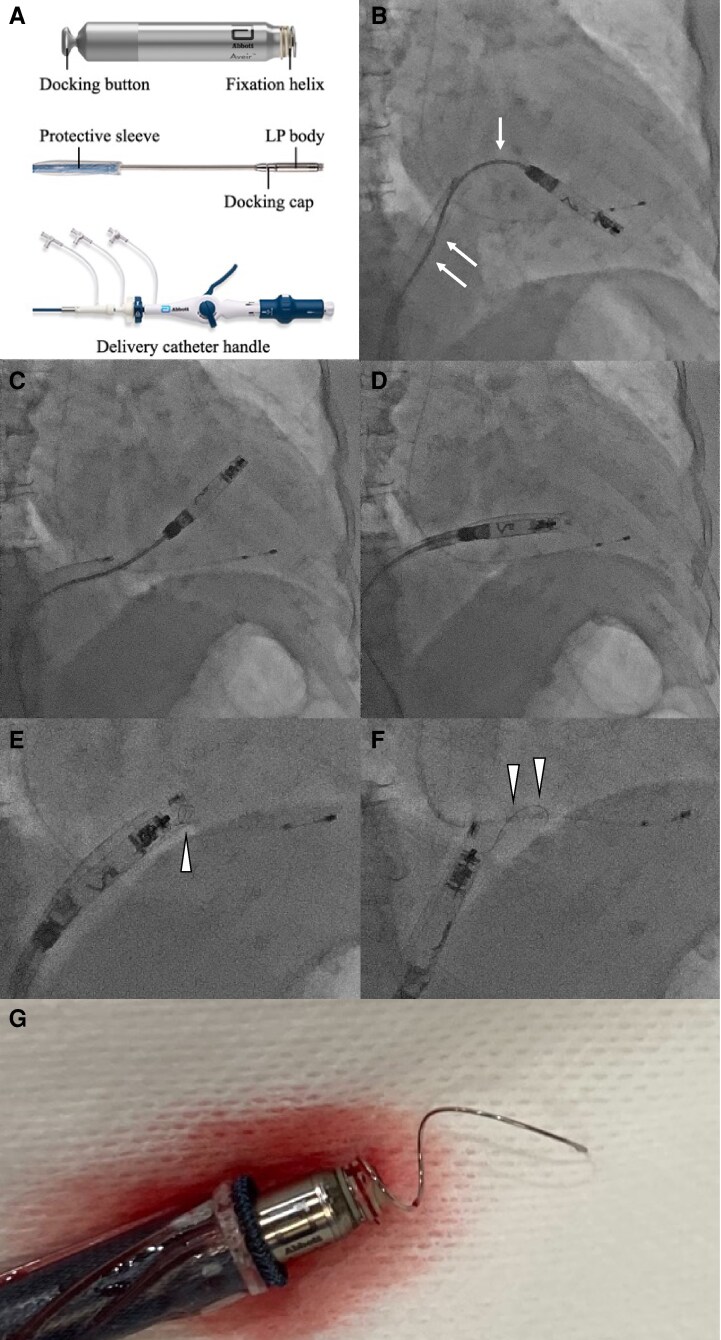 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsShoulder Injury and Treatment · Shoulder and Clavicle Injuries · Pain Management and Treatment
Case description
The Aveir™ VR single-chamber (Figure 1A) and DR dual-chamber leadless pacemakers (LPs) (Abbott, Chicago, IL) were approved in 2022 and 2025, respectively. With advantages such as a high procedural success rate, retrievability, and long battery life, this novel helix-fixation system has gained widespread adoption.^1–4^ Consequently, the incidence of device-related complications is expected to increase, including cardiac perforation, dislodgement, stretched helix, and tricuspid injury.^3–6^ To our knowledge, this is the first report describing simultaneous chordae tendineae rupture and helix stretching during implantation.
(A) The Aveir™ VR single-chamber leadless pacemaker and leadless pacemaker delivery system. (B) Sleeve-out refers to the process in which the protective sleeve covering the leadless pacemaker body is retracted, thereby exposing the leadless pacemaker body. The leadless pacemaker delivery catheter showed bending that was likely caused by accumulated catheter torque and strong backup force (arrows). (C) The leadless pacemaker was dislocated from the right ventricular apical septum to the right ventricular outflow tract. (D) The leadless pacemaker became fully covered with a protective sleeve. (E) Pulling of the leadless pacemaker and delivery catheter resulted in an elongation of the helix. Helix elongation was first observed around the right atrium and tricuspid valve (arrow). (F) Complete helix elongation was noted around the right atrium and inferior vena cava (arrows). (G) Helix elongation was confirmed.
An 89-year-old woman was referred for evaluation of syncope caused by an atrioventricular block lasting 8 s. Her medical history included paroxysmal atrial fibrillation and chronic kidney disease. A temporary pacing lead was emergently inserted. Considering her advanced age and frailty, LP implantation was selected for its lower complication risk.^3^ Subsequently, helix-fixation LP implantation via the femoral vein was performed. The LP was initially positioned at the apical septum and was screwed in and out twice because of unacceptable thresholds and impedance values. After a slight positional adjustment and subsequent sleeve-out, the LP drifted from the right ventricular apical septum to the right ventricular outflow tract (Figure 1B and C). The LP became fully covered with a protective sleeve; however, marked resistance was encountered during advancement and withdrawal of both the LP body and the delivery catheter (Figure 1D). Pulling of the LP and delivery catheter resulted in an elongation of the helix (Figure 1E and F; Supplementary material online, Video S1). After removal of the LP and delivery catheter from the body, helix elongation and ruptured chordae tendineae were visually confirmed (Figure 1G). A new LP was safely implanted using a different delivery catheter. Transthoracic echocardiography revealed progression of tricuspid regurgitation from moderate before the procedure to severe after the procedure. No cardiac events occurred during the 4-month follow-up. Tricuspid regurgitation improved to a moderate level over time.
A previous report described tricuspid valve entrapment by the delivery catheter, with tissue caught between the docking button and cap.^5^ In our case, the tissue was entrapped by the helix itself, leading to helix elongation and chordae tendineae rupture. The US Food and Drug Administration database reported 11 events involving stretched helices between 2022 and 2023,^6^ highlighting the clinical relevance of this complication. Movement of an exposed LP poses a risk of tricuspid valve entanglement, as seen in our case. Repositioning inherently involves multiple LP exposures during the sleeve-out process, and 16.8% of cases reportedly required at least one device repositioning during implantation.^3^ Leadless pacemaker translocation in our case was likely caused by accumulated catheter torque and strong backup force, compounded by repeated rotation and advancement of the delivery catheter, limited right ventricular space, and catheter stiffness. Avoiding excessive force during delivery catheter manipulation and minimizing sleeve-out exposure are essential to reduce such complications. This case emphasizes the importance of careful procedural planning and awareness of potential helix-related complications during helix-fixation LP implantation.
Supplementary Material
ytag090_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Morita J, Kondo Y, Kasai Y, Kitai T. Retrieval of the Aveir™ leadless pacemaker with the double-snare technique. Eur Heart J Case Rep 2024;8:ytae 267.38915739 10.1093/ehjcr/ytae 267PMC 11195313 · doi ↗ · pubmed ↗
- 2Yamamoto R, Kataoka N, Imamura T, Nakamura M, Kinugawa K. Temporary use of leadless pacemaker as a bridge to cardiac resynchronisation therapy: a case report of fulminant myocarditis. Eur Heart J Case Rep 2025;9:ytaf 316.40726613 10.1093/ehjcr/ytaf 316PMC 12301293 · doi ↗ · pubmed ↗
- 3Reddy VY, Exner DV, Doshi R, Tomassoni G, Bunch TJ, Estes NAM, et al LEADLESS II investigators. Primary results on safety and efficacy from the LEADLESS II-phase 2 worldwide clinical trial. JACC Clin Electrophysiol 2022;8:115–117.34863657 10.1016/j.jacep.2021.11.002 · doi ↗ · pubmed ↗
- 4Glikson M, Nielsen JC, Kronborg MB, Michowitz Y, Auricchio A, Barbash IM, et al 2021 ESC guidelines on cardiac pacing and cardiac resynchronization therapy. Eur Heart J 2021;42:3427–3520.34586378 10.1093/eurheartj/ehab 699 · doi ↗ · pubmed ↗
- 5Nomura T, Kumazawa D, Onodera K, Mizuno Y, Toyoda S, Yamashita K. Helix-fixation leadless pacemaker delivery catheter reeling in intracardiac tissue and becoming stuck: a case report. Heart Rhythm Case Rep 2024;10:479–482.39129731 10.1016/j.hrcr.2024.04.010PMC 11312029 · doi ↗ · pubmed ↗
- 6Garg J, Shah K, Bhardwaj R, Contractor T, Mandapati R, Turagam MK, et al Adverse events associated with Aveir TM VR leadless pacemaker: a Food and Drug Administration MAUDE database study. J Cardiovasc Electrophysiol 2023;34:1469–1471.37209414 10.1111/jce.15932 · doi ↗ · pubmed ↗