Robotic Conversion of Single Anastomosis Duodeno-Ileal Sleeve (SADI-S) to Roux-en-Y Gastric Bypass (RYGB): A Novel Approach
Ahmad E Al-Mulla, Abdulla Sultan, Giorgio A Barretta, Maher Elchaar

TL;DR
This paper presents a rare case of using robotic surgery to convert a SADI-S bariatric procedure to a Roux-en-Y gastric bypass, showing it is feasible and effective.
Contribution
The paper introduces a novel robotic approach for revising a SADI-S procedure to RYGB, addressing challenges in revisional bariatric surgery.
Findings
Robotic conversion from SADI-S to RYGB was successfully performed.
The robotic approach demonstrated improved precision and safety in complex revisional cases.
The patient experienced favorable outcomes following the conversion.
Abstract
The single anastomosis duodeno-ileal sleeve (SADI-S) presents a simplified alternative to the duodenal switch. However, this procedure may result in malabsorption and associated complications for some patients. Revisional bariatric surgery can be extremely challenging, particularly following a previous intervention, and conventional laparoscopy may be limited in these complex cases. The introduction of robotic surgery has improved both precision and safety in such cases. This report describes a scarce case of robotic conversion from SADI-S to Roux-en-Y gastric bypass, illustrating its feasibility and favorable patient outcomes.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
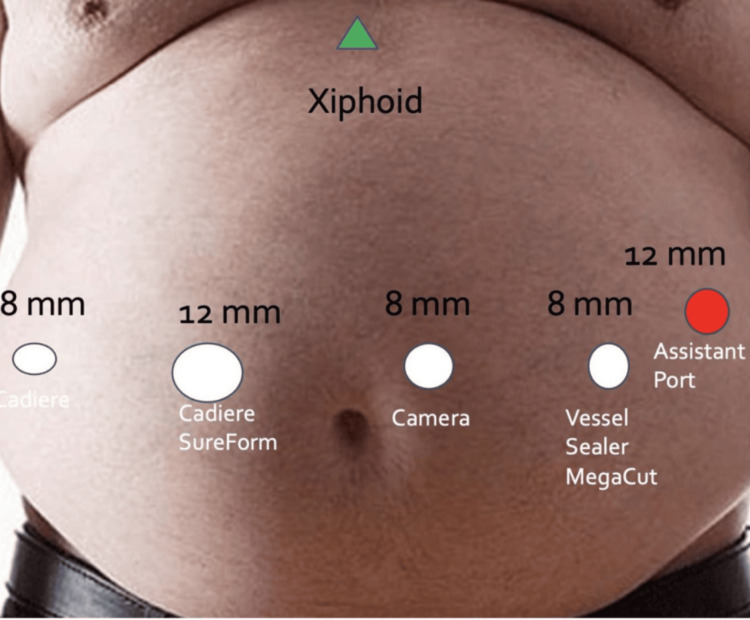 Figure 1
Figure 1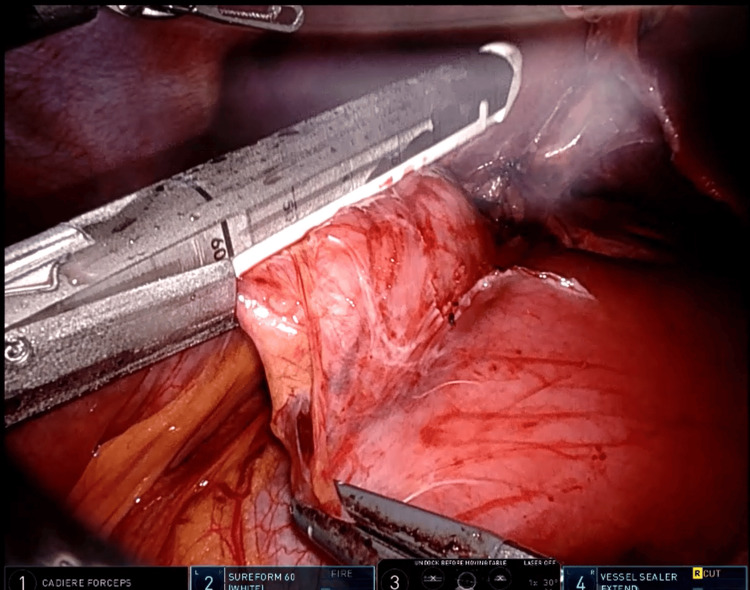 Figure 2
Figure 2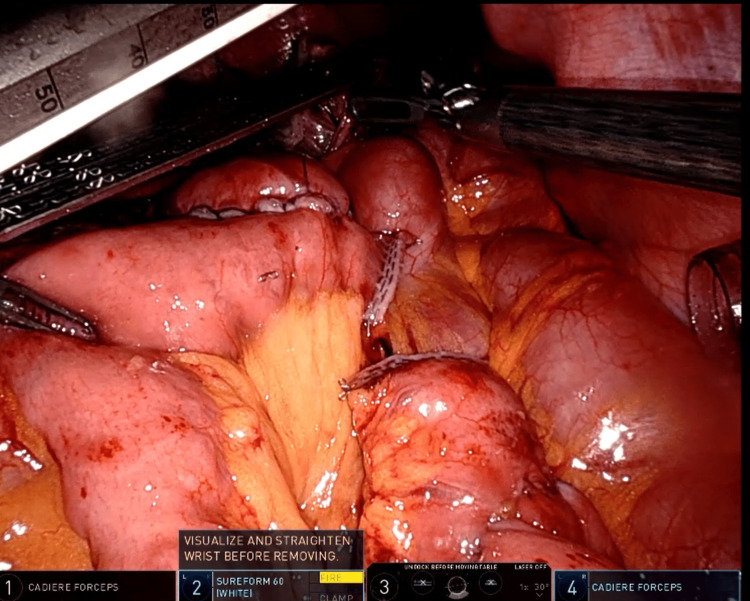 Figure 3
Figure 3| Parameter | Pre-revision value | Reference range (adult female) | Post-revision value | Interpretation |
| Total protein (g/L) | 40 | 60-80 g/L | — | Hypoproteinemia |
| Albumin (g/L) | 28 | 35-50 g/L | — | Hypoalbuminemia |
| Vitamin D, 25(OH) (ng/mL) | 22 | 30-100 ng/mL | — | Insufficiency |
| Serum calcium (mmol/L) | 1.52-1.9 | 2.1-2.6 mmol/L | 2.2-2.35 | Normalized post-revision |
| Parathyroid hormone (pmol/L) | 28.9 | 1.6-6.9 pmol/L | — | Secondary hyperparathyroidism |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBariatric Surgery and Outcomes · Minimally Invasive Surgical Techniques · Esophageal and GI Pathology
Introduction
The global obesity epidemic has driven the evaluation of bariatric surgery, with procedures shifting from restrictive operations to combined techniques incorporating malabsorption. Single-anastomosis duodeno-ileal sleeve (SADI-S) can be considered either a primary or a second-stage procedure, often performed after sleeve gastrectomy (SG) [1]. Despite the advantages of SADI-S, it is associated with complications such as malabsorption, weight regain, vitamin deficiency, and marginal ulcers, thus requiring revisional surgery [2]. Conversion to Roux-en-Y gastric bypass (RYGB) is often performed to reduce malabsorption, restore regular alimentary continuity, and aid weight loss. However, revisional surgery is often challenging and highly demanding, particularly when performed laparoscopically due to limited freedom in small spaces, 2D visualization, spatial disorientation, ergonomic difficulties, and difficult camera movement, leading to a high conversion rate [3].
Robotic surgery is becoming increasingly common in bariatric procedures, especially in revision surgeries, where dense adhesions and altered anatomy pose significant challenges [4]. The advantages of robotic surgery, such as 3D vision, enhanced wrist mobility, tremor reduction, and a surgeon-controlled camera, help overcome the limitations associated with traditional laparoscopic techniques [5]. In this report, we present a rare case of converting from a previous SADI-S to a RYGB in a patient who experienced prolonged hypocalcemia.
Case presentation
This case involves a 33-year-old female patient who was admitted through our outpatient department. She has a history of undergoing an SG in 2010 due to a BMI of 51 kg/m². Over the course of 10 years, she lost approximately 31 kg but subsequently regained more than 50% of that weight. In 2022, she underwent an SADI-S procedure as a revisional surgery, with resizing of the sleeve and the creation of a 270-cm common limb. After this second procedure, she experienced significant weight loss (BMI: 25 kg/m^2^) and maintained good nutritional status. However, during her recent follow-ups, she reported frequent bowel movements and episodes of dizziness that began six months before her admission. She had also been hospitalized previously for lethargy, dizziness, and frequent bowel movements. During that time, she was managed conservatively, advised to consult a dietitian, adhered to her supplement regimen, and followed up at our bariatric outpatient department.
In September 2025, she was readmitted, complaining of frequent bowel movements, vomiting, and generalized weakness. Upon examination, she was vitally stable but exhibited some physical abnormalities. Laboratory tests revealed decreased levels of protein (40 g/L), albumin (28 g/L), and vitamin D (22 ng/mL). Other investigations were unremarkable, including vitamin B_6_ and B_12_. Notably, she presented with persistent hypocalcemia (1.52-1.9 mmol/L) and elevated parathyroid hormone (28.9 pmol/L) levels (Table 1), despite efforts by her treating team and an endocrinologist to correct this condition. Further investigations, including sestamibi scans and neck ultrasounds, were performed to address her hypocalcemia. Additional investigations, such as FibroScan, abdominal ultrasound, endoscopy, and colonoscopy, revealed unremarkable findings.
The patient was initially on a clear liquid diet, which later progressed to a regular oral diet. She received vitamins and calcium supplementation through intravenous infusion; however, we were unable to maintain her calcium levels within the normal range. Additionally, she continued to experience frequent bowel movements, reporting up to 10 times a day. As a result, we decided to revise her surgical procedure to a less malabsorptive option, such as RYGB. Conceding the former bariatric history of the patient, we decided to consider a robotic revisional approach. The patient consented to the robotic surgery and was prepared for the procedure following a consultation with the anesthesiology team and signing of the consent form.
The port placement was configured in the upper abdomen, with five ports arranged along a horizontal line across the abdomen (Figure 1). Liver retraction was performed just below the xiphoid process. The procedure began with the dissection of adhesions from previous surgeries. Initially, a laparoscopic approach was used to measure the common limb length, which, surprisingly, measured 217 cm. Afterward, the robot was docked, and further dissection of the previous procedure site was performed.
Port locations for upper GI robotic surgery
The first step involved dividing the previous duodeno-ileal anastomosis using a white cartridge (Figure 2). Next, the stomach was divided, and a small pouch was created for the gastro-jejunal anastomosis using a blue cartridge. The biliopancreatic limb was constructed to be 70 cm from the Treitz ligament, while the alimentary limb was constructed to a length of 70 cm. All enterotomy openings were closed with barbed (V-Loc 3-0) sutures, potential spaces for internal hernia were closed with non-absorbable (Ethibond 2-0) sutures, and the biliopancreatic limb was divided using a white cartridge (Figure 3). The procedure lasted approximately three hours.
Duodeno-ileal anastomosis divided using a white cartridge stapler
Roux-en-Y gastric bypass with 70 cm biliopancreatic limb and 70 cm alimentary limb
The patient's post-operative course was unremarkable. Fluids were initiated on the same day, and she was encouraged to mobilize immediately upon full recovery. Calcium levels normalized (2.2-2.35 mmol/L) (Table 1) and remained stable with supplementation. The patient was discharged two days postoperatively and was advised to follow up in our outpatient department.
During her first follow-up visit after two weeks, the patient experienced mild nausea and vomiting and was reassured. All investigations were normal, showing no decrease in calcium levels (2.25 mmol/L), and she continued to be followed closely (Table 1).
Discussion
SADI-S was first described in 2007 and is known for achieving significant weight loss with a lower complication rate [6]. It accounts for 2% of metabolic bariatric surgery (MBS) procedures performed in the US [7]. Despite being considered a relatively safe procedure, it requires close patient follow-up to prevent potentially life-threatening complications. Some complications reported in the literature include marginal ulcers, bile reflux, duodenal stump blowout, and malnutrition [8].
Malnutrition is one of the most concerning long-term complications associated with bariatric surgery. It has been linked to malabsorptive procedures such as jejunoileal bypass, biliopancreatic diversion, and duodenal switch (DS). While SADI-S is an alternative, milder, and more straightforward malabsorptive procedure compared to the DS, it can still lead to malnutrition in some patients, especially if they have a shorter common channel (<250 cm) [9]. This was discussed in our previous case report; the patient required revision surgery after failing to progress and maintain their nutritional status.
Revisions in bariatric surgery are generally more complex than primary surgeries. Factors such as adhesions and altered anatomy contribute to an increased risk of blood loss, longer operative times, extended hospital stays, admission to the intensive care unit, post-operative complications, and early readmissions to the hospital [10]. Approximately 28% of patients undergoing MBS may require revision. In 2019, 16.8% of MBS patients underwent revisional surgery [11].
Robotic revisional bariatric surgery (R-RBS) is gaining popularity, especially in cases where precise suturing, detailed dissection, and enhanced visualization are crucial. Studies show that R-RBS results in better outcomes and shorter hospital stays than traditional laparoscopic surgery [12,13]. This success can be attributed to the standardization of techniques in practice and in the operating theater, which leads to shorter operative times and higher turnover rates [14].
In our case report, we chose the RYGB procedure, which offers a balance between restriction and malabsorption while minimizing the risks of severe protein deficiency and bile reflux. These complications may arise with other surgical options. RYGB was deemed a better choice than revising the common limb, as re-anastomosing the duodenum can be technically challenging [1].
The use of R-RBS in our case represents a novel approach and has not been described in the literature to date. While there have been instances of converting a SADI-S to either RYGB or one anastomosis gastric bypass, these procedures were performed laparoscopically [1,15]. Thus, this specific conversion is rare and has not been documented in the literature, underscoring the significance of our case report.
Conclusions
Revisional robotic bariatric surgeries are becoming increasingly popular due to their high precision and low complication rates. Many complex cases have been completed using robotic surgery, which can be challenging with traditional laparoscopy. Converting from SADI-S to RYGB is feasible and can be safely performed in experienced centers. This case contributes to the limited literature on the subject and highlights the potential of robotic platforms in managing severe complications.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Laparoscopic conversion from single anastomosis duodeno-jejunal bypass with sleeve gastrectomy (SADJ-S) to Roux-en-Y gastric bypass (GBP): improving unsatisfactory outcomes Obes Surg Vilallonga R Curbelo Y Sanchez-Cordero S Roriz-Silva R Bademci R Torres AJ 3653683020203118378610.1007/s 11695-019-03994-2 · doi ↗ · pubmed ↗
- 2Revisional surgery for malnutrition after SADI-S: prevalence, indications, techniques and outcomes Updates Surg Sánchez-Pernaute A Lasses B Antoñanzas LL 187918857620243880517310.1007/s 13304-024-01900-9PMC 11455684 · doi ↗ · pubmed ↗
- 3Outcomes of robotic surgery in revisional bariatric cases: a propensity score-matched analysis of the MBSAQIP registry J Robot Surg El Chaar M King K Pastrana M Galvez A Stoltzfus J 2352391520213247479510.1007/s 11701-020-01098-z · doi ↗ · pubmed ↗
- 4Outcomes of robotic-assisted bariatric surgery compared to standard laparoscopic approach using a standardized definition: first look at the 2020 Metabolic and Bariatric Surgery Accreditation Quality Improvement Project (MBSAQIP) data Obes Surg El Chaar M Petrick A Clapp B Stoltzfus J Alvarado LA 202520393320233718482710.1007/s 11695-023-06585-4 · doi ↗ · pubmed ↗
- 5Robot-assisted hysterectomy compared to open and laparoscopic approaches: systematic review and meta-analysis Arch Gynecol Obstet O'Neill M Moran PS Teljeur C 90791828720132329192410.1007/s 00404-012-2681-z · doi ↗ · pubmed ↗
- 6Laparoscopic conversion of single-anastomosis duodenal switch (SADI-S) to Roux-en-Y gastric bypass with concurrent paraesophageal hernia repair for refractory biliary reflux and paraesophageal hernia Cureus Wargel ZM Ritchie TW Shapera E Wheeler AA 015202310.7759/cureus.36205 PMC 1010500637069860 · doi ↗ · pubmed ↗
- 7A matched cohort analysis of single anastomosis loop duodenal switch versus Roux-en-Y gastric bypass with 18-month follow-up Surg Endosc Cottam A Cottam D Medlin W Richards C Cottam S Zaveri H Surve A 395839643020162669418210.1007/s 00464-015-4707-7 · doi ↗ · pubmed ↗
- 8American Society for Metabolic and Bariatric Surgery 2020 estimate of metabolic and bariatric procedures performed in the United States Surg Obes Relat Dis Clapp B Ponce J De Maria E 113411401820223597074110.1016/j.soard.2022.06.284 · doi ↗ · pubmed ↗