Risk of Breast and Ovarian Cancer After Prophylactic Mastectomy and Salpingo‐Oophorectomy in BRCA1/2 Germline Variant Carriers: A Retrospective Cohort Study From a Single German Center
Sara Mendes, Maryam Yahiaoui‐Doktor, Eva Maria Fallenberg, Marion Kiechle, Sabine Grill

TL;DR
This study examines the effectiveness of prophylactic surgeries in reducing breast and ovarian cancer risks for women with BRCA1/2 gene mutations.
Contribution
The study provides new insights into the effectiveness of mastectomy versus breast-conserving surgery in preventing ipsilateral secondary cancers in BRCA1/2 carriers.
Findings
No breast cancer cases were observed after prophylactic bilateral mastectomy.
Mastectomy showed lower rates of ipsilateral secondary cancer compared to breast-conserving surgery.
Only 2.0% of patients who underwent PBSO had incidental ovarian cancer findings.
Abstract
As the data on BRCA1/2‐associated breast and ovarian cancer prevalence after prophylactic surgery has not been exhaustively investigated yet, we aimed to evaluate the cancer prevalence in a single center cohort of BRCA1 and BRCA2 carriers after conducting prophylactic mastectomy, as well as prophylactic bilateral salpingo‐oophorectomy (PBSO) respectively. We included 875 women that were tested positive for a germline variant in the BRCA1/BRCA2 gene (gPV) between 2002 and 2022 at the Center of Hereditary Breast and Ovarian Cancer of the Technical University Munich Germany. Mean follow up was 7.2 years (range 0–44 years; 95% CI: 6.70 to 7.70). We differentiated breast and/or ovarian cancer diseased (n = 643) and non‐diseased BRCA1/2 carriers (n = 232). Our analysis confirmed the effectiveness of prophylactic surgeries in genetically predisposed women with a gPV in the BRCA1/2 gene. We…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
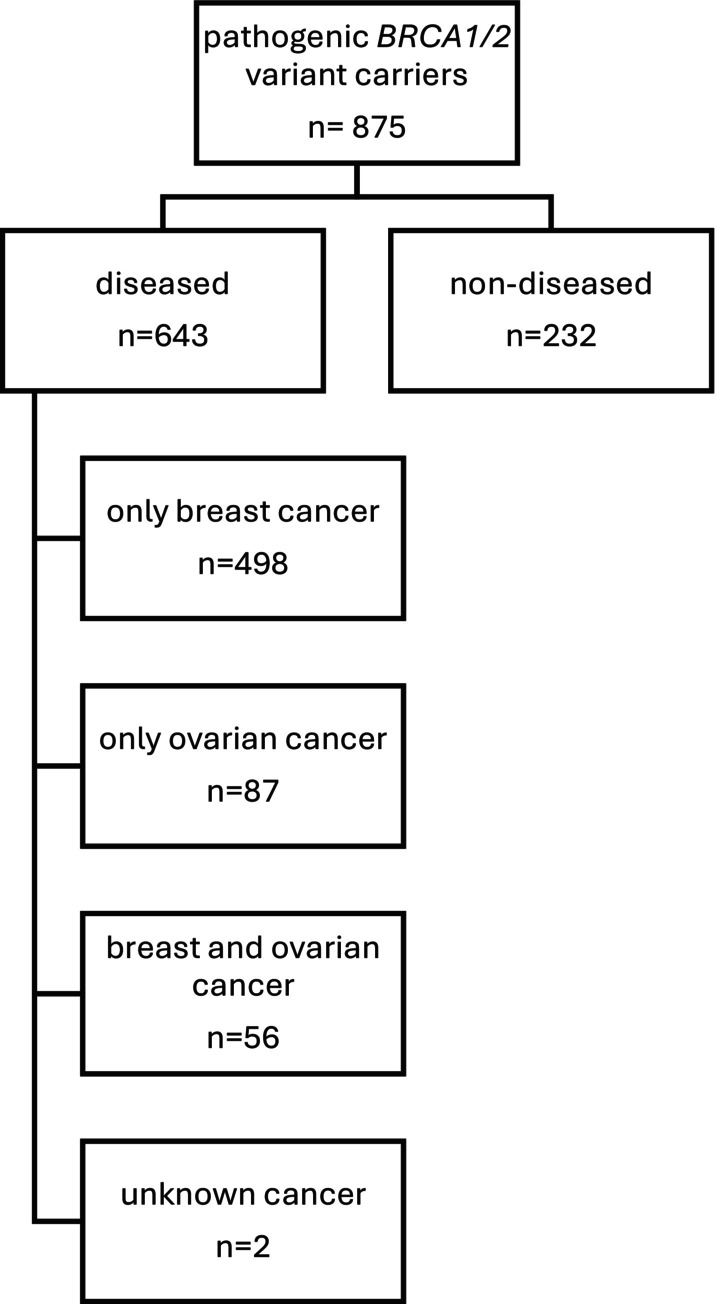 FIGURE 1
FIGURE 1| Second BC: cancer localization | Total | ||||
|---|---|---|---|---|---|
| Ipsilateral recurrence | Ipsilateral secondary cancer | Contralateral secondary cancer | |||
| First BC: type of surgery | Breast‐conserving surgery | 20 | 19 | 65 | 104 |
| 19.2% | 18.3% | 62.5% | 100.0% | ||
| Mastectomy | 11 | 2 | 34 | 47 | |
| 23.4% | 4.3% | 72.3% | 100.0% | ||
| Total | 31 | 21 | 99 | 151 | |
| 20.5% | 13.9% | 65.6% | 100.0% | ||
| PBM | PBSO | |||
|---|---|---|---|---|
|
|
| Count | 38 | 48 |
| % | 67.9% | 72.7% | ||
|
| Count | 18 | 18 | |
| % | 32.1% | 27.3% | ||
| Total | Count | 56 | 66 | |
| % | 100.0% | 100.0% | ||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBRCA gene mutations in cancer · Breast Cancer Treatment Studies · Male Breast Health Studies
Introduction
1
Breast cancer is the most common cancer among women with an evaluated lifetime risk of 13.2% [1]. Familial susceptibility to breast cancer thereby accounts for approximately 30%–40% of all breast cancer cases. An estimated 10% of all breast cancers are developed monogenic, meaning that a single disease‐causing (pathogenic) variant is responsible for the increased risk. The majority of the monogenic inherited breast cancer diseases is attributed to the tumor suppressor genes BRCA1 and BRCA2, which play a crucial role in DNA double‐strand repair (homologous recombination). Pathogenic germline variants (gPV) in these genes confer a high risk to breast and ovarian cancer, respectively [2]. The cumulative lifetime risk of developing breast cancer and ovarian cancer is 72% and 44% for BRCA1, as well as 69% and 17% for BRCA2, respectively [3]. Given these high cancer risks, carriers of a pathogenic (g) BRCA1/BRCA2 variant are opting to take part in an intensified breast cancer screening program or optionally undergo prophylactic surgeries, including prophylactic mastectomy (PBM) and bilateral salpingo‐oophorectomy (PBSO). The German Consortium for Hereditary Breast and Ovarian Cancer recommends that carriers of a gPV in BRCA1/2 participate in an intensified breast cancer screening program from the age of 25, or 5 years before the earliest breast cancer diagnosis in the family [2]. The screening program consists of an annual MRI and six‐monthly sonography [2]. From the age of 40, mammography can be performed additionally every 1–2 years according to physicians' choice [2]. Out of these diagnostic tools, MRI is the most sensitive screening method for early breast cancer detection [4, 5, 6].
By contrast, early detection of ovarian cancer is still insufficient [7, 8, 9]. Neither screening with serum CA125 concentration regardless of whether it is examined serially or one‐time, nor transvaginal ultrasound screening resulted in mortality reduction [7, 8, 9].
Due to the high lifetime risks of developing breast and ovarian cancer, a great share of these carriers opt for a primary preventive approach of prophylactic surgery, primarily PBSO, as effective screening options for early detection of ovarian cancer are still missing. PBSO can reduce the risk of developing ovarian cancer by 80%–90% [10, 11, 12, 13, 14]. Under consideration of the age‐dependent risk for ovarian cancer and the postoperative side effect of premature menopause, the procedure is currently recommended from the age of 40 years, or 5 years before the youngest age of onset of ovarian cancer [12, 15]. In exceptional cases carriers of a gPV in BRCA1 can undergo the procedure from the age of 35 [15]. As far as prophylactic mastectomy is concerned, several studies have shown that PBM significantly reduces the incidence of breast cancer by 90%–100% [14, 16, 17, 18, 19, 20, 21]. Once PBM is conducted, the determined residual lifetime risk for breast cancer is given 4%–6%. In light of this dramatic risk reduction, the intensified screening program will be terminated.
As the data on BRCA1/2‐associated breast and ovarian cancer prevalence after prophylactic surgery has not been exhaustively investigated yet, we aimed to evaluate the cancer prevalence in a single center cohort of BRCA1 and BRCA2 carriers after conducting prophylactic bilateral and contralateral mastectomy, as well as prophylactic bilateral salpingo‐oophorectomy, respectively.
Results
2
A total of 875 female patients were included in the analysis. All had been tested positive for a gPV in the genes BRCA1 or BRCA2 at the FBREK center TU Munich, Germany.
For analysis we differentiated diseased (breast and/or ovarian cancer; n = 643) and non‐diseased BRCA1/2 carriers (n = 232) (Figure 1).
Flowchart of study cohort classification. The diagram shows the distribution of 875 individuals with pathogenic BRCA1/2 variants, categorized into diseased (n = 643) and non‐diseased (n = 232). Diseased individuals were further classified based on cancer type: only breast cancer (n = 498), only ovarian cancer (n = 87), both breast and ovarian cancer (n = 56), and unknown cancer (n = 2).
Diseased Cohort
2.1
Within the cohort of diseased participants (n = 643) 61.6% were tested positive for a gPV in BRCA1 and 37.9% for BRCA2 respectively. Only 0.2% (n = 1) of study participants carried a gPV in both genes. The prevalence of breast cancer was 86.2% and 22.2% for ovarian cancer. 10.1% of patients were affected by both cancers. BRCA1 carriers were diagnosed at younger age compared to participants with a gPV in the BRCA2 gene (41.6 vs. 46.1 years for breast cancer. p < 0.001; 53.5 vs. 60.4 years for ovarian cancer, p < 0.001). The presence of multiple tumor diseases was almost doubled in gBRCA1 carriers with a rate of 10.6% compared to 5.7% in gBRCA2 carriers. All analyses in the diseased cohort refer to a mean follow up of 8.2 years (range 0–44 years).
Breast Cancer
2.1.1
Five hundred and fifty‐four study participants are breast cancer diseased with a mean age of 43.4 years at time of diagnosis. 89.3% had unilateral and 4.7% bilateral breast cancer at time of first diagnosis (6% unknown localization). Complete data on hormone receptor and Her2 status was available for 412 patients. A total of 55.3% (n = 228) demonstrated triple negative receptor status (TNBC). 85.1% of the triple negative tumors were linked to a gPV in BRCA1. As TNBC is a testing criterion for gPV BRCA1/2 in Germany and often attributed to a gPV in BRCA1, it can be expected that this number is generally overestimated. 36.4% (n = 150) of the breast cancer cases showed hormone receptor positive and Her2 negative tumor biology, mainly associated with gBRCA2 carrier status (30.0% BRCA1 and 70.0% BRCA2). The rate of Her2 positive receptor status was limited to 8.3%.
With regard to therapeutical management, data was available for 461 patients. 57.3% (n = 264) of the patients opted for a breast‐conserving surgery, and 42.7% (n = 197) for a mastectomy. 44.2% (n = 87) of the mastectomized patients chose to undergo an additional contralateral prophylactic mastectomy (CPM) in the following 5 years. The mastectomy rate was higher among BRCA1 carriers compared to patients with a gPV in BRCA2 (45.4% vs. 38.9%; p = 0.171).
Within the collective of the breast cancer diseased carriers, who initially decided on breast‐conserving surgery (n = 264), only 14.0% (n = 37) of patients chose to undergo CPM in the following 5 years. 23.1% (n = 61) subsequently opted for a secondary unilateral mastectomy. On average, this surgery was performed 5.7 years (SD = 5.80) after the initial breast cancer diagnosis at a mean age of 46.57 years (SD = 9.96).
A second breast cancer disease occurred in 30.3% of patients (n = 168) after a mean period of 7.8 years (SD = 5.67). Contralateral secondary cancer was most common with a share of 67.3%. 19.7% had an ipsilateral recurrence and 13.0% an ipsilateral secondary cancer. 65.5% were gBRCA1 and 33.9% were gBRCA2 carriers. In relation to the total diseased cohort, 17.9% of all gBRCA1 and 15.2% of all gBRCA2 carriers developed a contralateral secondary cancer. For 129 patients we had complete data on the type of surgery for secondary cancer treatment. 44.2% opted for breast‐conserving surgery, 49.6% for a mastectomy and 4.7% for a lumpectomy after a previous mastectomy (ipsilateral disease). 2 cases of contralateral breast cancer (1.4%) were reported after CPM. These cases appeared 6 and 8 years after CPM and were associated to a PV in the BRCA1 gene.
We analyzed the localization of a secondary breast cancer in relation to the type of surgery during the first breast cancer. In this cohort of patients with secondary breast cancer (n = 152), 30.9% had undergone a mastectomy and 69.1% a breast‐conserving surgery (p < 0.001). Consequently, we looked at the secondary cancer localization (ipsilateral or contralateral). In the group of patients who had breast‐conserving surgery during their first cancer treatment, 19.2% had an ipsilateral recurrence and 18.3% an ipsilateral secondary cancer with a different tumor biology. 62.5% developed a contralateral secondary cancer. Within the patients who were first treated with a mastectomy, 23.4% showed an ipsilateral recurrence, 4.3% an ipsilateral secondary cancer and 72.3% a contralateral secondary cancer. Patients who had had a breast‐conserving surgery tended to have a higher percentage of secondary ipsilateral cancer than the group who had had a mastectomy, yet statistical significance was not reached (37.5% vs. 27.7%; p = 0.255). The lower rate in contralateral secondary cancers after breast‐conserving surgery compared to mastectomy could be attributed to scattered radiation after breast‐conserving therapy, though no statistically significant difference (p = 0.239) could be found (Table 1).
A total of 31 patients (5.6%) developed a third breast cancer (n = 21 BRCA1 gPV; n = 10 BRCA2 gPV). Of these, 6 patients (1.1%) also suffered a fourth breast cancer (BRCA1 carrier: n = 4; BRCA2 carrier: n = 2). On average a third cancer appeared 11.2 years (SD = 6.68) and a fourth cancer 13.5 years (SD = 7.15) after the first cancer.
Ovarian Cancer
2.1.2
In our analysis 143 patients had ovarian cancer. The mean age at the diagnosis was 55.5 years (SD = 9.5). 71.3% were gBRCA1‐ and 28.7% g*BRCA2‐*carriers.
We noted 6 incidental findings of cancer when conducting PBSO. Out of these 6 patients, 4 patients were diagnosed with early‐stage ovarian cancer (max. pT1c), one patient with serous tubal intraepithelial carcinoma (STIC), and another one with carcinoma of unknown histopathology. Five patients carried a gBRCA1 and one patient a gBRCA2. The mean age at diagnosis was 55.0 years (range 48–60). Out of these patients, 4 had previously been diagnosed with breast cancer.
Prophylactic Bilateral Salpingo‐Oophorectomy
2.1.3
In the breast cancer diseased group (n = 554) 39.7% underwent a PBSO with no pathological result. Of these, 55.5% were carriers of a gPV in BRCA1 and 44.1% in gBRCA2 (p = 0.047). Mean age at the intervention was 48.9 years (SD = 10.10) (mean age gBRCA1 47.7 years (n = 112; SD = 9.9)), gBRCA2 50.4 years (n = 91; SD = 10.2).
Non‐Diseased Mutation Carriers
2.2
Among the non‐diseased carriers (n = 232) 59.9% carried a gPV in BRCA1 (n = 139) and 40.1% in the BRCA2 gene (n = 93). 13.4% opted for a bilateral prophylactic mastectomy exclusively (mean age 31.6 years; age range 19–44; SD = 6.4), 17.7% for PBSO (mean age 45.6 years; SD = 8.251) and 10.8% for both surgeries (mean age PBM 43.4 years; SD = 5.3; PBSO 43.0 years; SD = 7.0). Mean follow‐up was 4.4 years (range 0–19 years).
We did not observe any cases of breast cancer following PBM and only one patient who had a PBSO at the age of 67 developed ovarian cancer by the age of 71 (patient who had a laparoscopic PBSO at 67 due to an ovarian cyst progressive in size and developed an extraovarian serous adenocarcinoma (G3) at the age of 71 with lymphangiosis carcinomatosa and multiple lymph node metastases).
As shown in Table 2, our results suggest that gBRCA1 carriers undergo PBSO significantly more frequently than gBRCA2 carriers (72.7% vs. 27.3%; p = 0.012). Yet no difference could be found concerning PBM rate (p = 0.164).
Cancer Screening Participation
2.3
19.3% (n = 124) of all patients in the cancer diseased group (n = 643) participated in the intensified cancer screening program at rechts der Isar hospital. 14.6% were not included into the program due to bilateral mastectomy and 66.1% did not participate at all or visited a different hospital for the diagnostics. Out of all patients who initially had a breast conserving therapy (n = 264), 26.1% participated in the intensified program and 12.1% were excluded due to secondary bilateral mastectomy, when looking at the patients who initially underwent a mastectomy (n = 197), 9.6% participated and 30.5% were excluded due to bilateral mastectomy.
In the non‐diseased group (n = 232), the participation in the intensified screening program was higher compared to the diseased group (p < 0.001). 40.9% (n = 95) of the non‐diseased carriers performed intensified breast diagnostics at the TUM. 16.4% were not included due to PBM, and the remaining 42.7% have either participated in the program at another hospital or not at all.
Discussion
3
In our study, we primarily sought to carry out a genotype–phenotype correlation in BRCA1/2 carriers and in particular to demonstrate the effectiveness of prophylactic surgery.
With regard to the gPV BRCA1 and BRCA2 distribution, our patient collective showed a very similar distribution compared to existing data sets. 61.1% were gBRCA1, 38.6% were gBRCA2 carriers (0.1% carrying both mutations; n = 1). Rebbeck et al. demonstrated almost identical prevalence rates when investigating more than 43,000 patients from the CIMBA database (Consortium of Investigators of Modifiers of BRCA1/2) [22]. When examining the higher percentage of gPV BRCA1 carriers, it is important to address a potential bias. Specifically, in Germany, TNBC serves as a testing criterion for hereditary breast and ovarian cancer. As TNBC is frequently associated with gPV BRCA1, this could lead to an overestimation of the TNBC and gPV BRCA1 rates respectively. In our study 55.3% of all breast cancer cases showed a triple negative tumor biology (85.1% associated to BRCA1), which does not reflect the normal subtype distribution.
Mean age at breast and ovarian cancer diagnosis overall correlates with other studies. In our research, breast cancer in gPV BRCA1 carriers was diagnosed at a mean age of 41.6 and 46.1 years for gPV BRCA2 carriers respectively. Very similar ages were found in other comprehensive studies [3, 23, 24]. Mean age for ovarian cancer diagnosis (n = 143) was 53.5 years for gBRCA1 and 60.4 years for gBRCA2 carriers. These ages were also very similar to a prospective cohort study [25].
We found that patients with a gPV in BRCA1 had a higher percentage for mastectomies than patients with a gPV in BRCA2 (45.4% vs. 38.9%; p = 0.171). This information should be interpreted with caution. On the one hand, the result was not statistically significant, and on the other, BRCA1 carriers are generally more prone to develop more aggressive tumor types, such as TNBC, as well as having a higher histological grade at diagnosis, which may also influence surgical decision‐making [24, 26, 27].
Above all, in this study we were able to demonstrate the efficacy of prophylactic surgery in carriers with a gPV in the BRCA1 and BRCA2 gene. Over a median follow‐up period of 7 years up to a maximum of 44 years (95% CI: 6.70 to 7.70), we analyzed the prevalence of cancer after previous therapeutic and prophylactic surgery in a cohort of 875 female BRCA1/2 carriers. Despite the extremely high cancer risks that derive from a gPV in the BRCA1 and BRCA2 gene, none of the carriers who had previously undergone bilateral prophylactic mastectomy was diagnosed with breast cancer during the entire follow‐up period, emphasizing the effectiveness of prophylactic surgery. In addition to that the prevalence of breast cancer after contralateral prophylactic mastectomy was also very low, with a total of two cases. These numbers largely correlate with existing studies. In a prospective analysis by Domcheck et al., no breast cancer was detected after conducting PBM in BRCA1/2 carriers during a 3‐year follow‐up (FUP) [14]. This data has been confirmed by another prospective study. Meijers‐Heijboer et colleagues stated to not have detected any breast cancer disease in the course of PBM after a mean FUP of 2.9 ± 1.4 years [16]. Critically considering the short time of FUP, Hartmann et al. were able to confirm these findings within 13 years of FUP [21]. In another study a 10‐year disease‐free survival of 100% was observed in the PBM group [19]. Rebbeck and colleagues supported these findings by demonstrating an incidence of 1.9% of breast cancer after a median follow‐up period of 6.4 years [18].
Within our analysis 17.9% of gBRCA1 carriers and 15.2% of gBRCA2 carriers developed contralateral breast cancer (CBC). Rhiem et al. calculated a cumulative 25‐year risk of CBC of 44.1% associated with a gPV in BRCA1 and 33.5% with a gPV in BRCA2 after initial diagnosis [28]. A prospective study showed a cumulative CBC risk of 25.1% and 6.6% for gBRCA1 and gBRCA2 carriers respectively (10 years after the first breast cancer) [29]. Yet, it was noticed that the risk of contralateral secondary disease after breast‐conserving surgery was considerably lower compared to mastectomy. The lower rate following a breast‐conserving approach could be attributed to scattered radiation after breast‐conserving therapy, though no statistically significant difference (p = 0.239) was found. While the concept of prophylactic mammary irradiation is currently being investigated to reduce the long‐term risk of contralateral breast cancer, this concept uses higher doses of radiation than the scattered radiation from primary cancer treatment [30, 31].
A systematic review and meta‐analysis of 13 studies demonstrated that BRCA1/2 carriers had a significantly higher risk of ipsilateral breast cancer recurrence after breast‐conserving surgery than controls with sporadic breast cancer (RR: 1.59; p < 0.001) [32]. In our study we had data on 39 patients who developed ipsilateral breast cancer after breast‐conserving surgery (Table 1). The percentage of a second ipsilateral cancer (recurrence or secondary cancer) was lower when patients had first received a mastectomy than when patients had had a breast‐conserving surgery (27.7% vs. 37.5%; p = 0.255). Furthermore, our data suggest that mastectomy significantly lowers the rate of ipsilateral secondary carcinomas compared to ipsilateral recurrences (4.3% vs. 23.4%; p < 0.05). The oncological safety of breast‐conserving therapy in gPV BRCA1/2 carriers is currently still a controversial topic. Data on whether the risk for local recurrence after breast‐conserving therapy is elevated in comparison to mastectomy is contradictory. Shubeck et al. compared the locoregional occurrence rate among gBRCA1/2 carriers who decided for breast‐conserving therapy versus mastectomy [33]. Yet there was no statistical significance. A meta‐analysis of four studies with 1254 patients found that gBRCA1/2 carriers with breast‐conserving therapy had a significantly higher risk for local recurrence than patients with mastectomy [34].
Additionally, numerous studies have shown a reduced prevalence of ovarian cancer including secondary peritoneal carcinoma after PBSO [10, 11, 14]. However, there is still no effective measure to prevent primary peritoneal carcinoma, although the prevalence is very low. In Kauff et al., 1% of patients developed a peritoneal carcinoma after PBSO [11]. Another study registered 5 patients with intra‐abdominal carcinomatosis in 238 patients who had undergone PBSO (2.1%) [35]. The findings in our analysis were consistent with the existing data situation demonstrating a prevalence rate of 0.45% (n = 1) for carriers developing peritoneal carcinoma after PBSO.
Within the entire study collective, a total of 293 have undergone PBSO, with 6 women having an incidental finding of ovarian cancer and STIC respectively (=2.0%; 1.7% gBRCA1 and 0.3% gBRCA2). In their analysis, Rebbeck et al. detected 8 women (3.1%) with ovarian or peritoneal carcinoma at the time of PBSO [10]. Finch et al. detected a much higher percentage of occult carcinoma findings at PBSO (6% of BRCA1 carriers and 2% of BRCA2 carriers) [36]. Currently PBSO is recommended from the age of 40, or 5 years before the youngest onset of ovarian cancer in the family [12, 15]. Emphasizing the patients with incidental findings of ovarian cancer in our study, all of them were older than 40 years when conducting PBSO (48–60 years), which raises the question of whether the findings could have been avoided by conducting prophylactic surgery earlier.
In addition to the prophylactic approaches, intensified breast cancer screening is of great importance in genetically predisposed women. In our study, only a small proportion, particularly of the breast cancer diseased BRCA1/2 carriers, have taken advantage of the intensified screening program. Nevertheless, our follow‐up data was limited. In this respect, it cannot be ruled out that the BRCA1/2 carriers of our study participated in the program at another center.
Jolie Effect
3.1
On 14.05.2013 Angelina Jolie published an article in the New York Times, where she addressed the identification of her gPV in the BRCA1 gene and the prophylactic bilateral mastectomy she had undergone since [37]. The “Jolie effect” describes the effects the article has had since that in healthcare. A few studies stated an increase in contralateral risk‐reducing mastectomies and PBM after Jolies article [38, 39]. Two other studies could not detect an increase in mastectomy rates or the rate of PBM among women who had already been tested for a gPV in BRCA1/BRCA2 [40, 41]. In correlation with the Jolie effect, we found a peak in the number of prophylactic mastectomies in 2013. After this first noticeable peak, mastectomy rates have risen since.
Limitations
3.2
As the study was executed with retrospective data over a long period of time, many patient cases were incomplete, and we did not have access to the same amount of data for each patient. We tried to obtain more current data on the patients through a follow‐up questionnaire, but even then, there were still many cases with incomplete data.
The effect of other treatments like chemotherapy or radiation was not included in the study. Especially when analyzing cancer recurrence, it should be taken into consideration that the surgical removal of the tumor is only one pillar of a systemic cancer therapy treatment.
Unfortunately, our data did not allow an analysis on the effect of PBSO on breast cancer. Further studies will have to be conducted to examine this point.
Materials and Methods
4
We included 875 women that were tested positive for gPV in BRCA1 and BRCA2 between 2002 and 2022 at the Center of Hereditary Breast and Ovarian Cancer (FBREK‐Center) of the Technical University Munich (TU Munich), Germany. The study is approved by the local Ethical Committee of the Technical University Munich (ID‐Nr. 2022‐476‐S‐KK) and written informed consent was obtained from all participants before entry into the study.
We collected retrospective data on genetic testing information and clinical data, as follows: age at diagnosis, tumor stage, tumor biology (e.g., estrogen/progesterone receptor status, Her2 status), type of surgery, previous cancer diseases and prophylactic surgeries. We also recorded age at the time of conducting prophylactic surgery (bilateral/contralateral PM; PBSO). Furthermore, we gathered information regarding the attendance at the intensified breast cancer screening program to evaluate the patients' compliance.
A follow up questionnaire was sent to 756 patients. Criteria for exclusion were death, unknown address, no consent for follow‐up questionnaires and residency in a non‐German speaking country. Response rate was 42%.
The beginning of follow‐up was marked by either a positive test for a gPV in BRCA1/2 or a related cancer disease. Patients were censored at last contact or after responding to the follow‐up questionnaire. Mean follow up was 7.2 years (range 0–44 years).
SPSS 29.0.1.0 was used for all data analysis. Independent samples t‐tests and chi‐square tests were applied where appropriate. All statistical tests were considered significant if they met the criteria of a two‐sided hypothesis test with a p‐value < 0.05.
Author Contributions
Sabine Grill: conceptualization, methodology, resources, writing – review and editing, supervision, project administration. Sara Mendes: methodology, investigation, formal analysis, writing – original draft, data curation, visualization. Marion Kiechle: conceptualization, methodology, resources, project administration, supervision. Eva Maria Fallenberg: resources, supervision. Maryam Yahiaoui‐Doktor: formal analysis.
Funding
The authors have nothing to report.
Ethics Statement
The study is approved by the local Ethical Committee of the Technical University Munich (ID‐Nr. 2022‐476‐S‐KK) and written informed consent was obtained from all participants before entry into the study.
Conflicts of Interest
Sara Mendes, Maryam Yahiaoui‐Doktor and Eva Maria Fallenberg declare no conflicts of interest. Marion Kiechle: Renumeration: Springer Press, Biermann Press, Celgene, Astra Zeneca, Myriad Genetics, TEVA, Eli Lilly, GSK, Seagen, AllergoSan, FOMF, Roche, BESINS, Bayer AG. Consultant/Advisory Role: Myriad Genetics, Bavarian KVB, DKMS Life, BLAEK, TEVA, Exeltis, Roche, BESINS, Bayer AG. Equity owner: AIM GmbH, In Manas GmbH, Therawis Diagnostic GmbH. Funding: Sphingotec, Deutsche Krebshilfe, DFG, Senator Roesner Foundation, Dr. Pommer‐Jung Foundation, Waltraut Bergmann Foundation, Bavarian State Ministry of Economy, BMBF, Innovation Fond GBA. Sabine Grill: contractual fees with Astrazeneca, Roche, Daiichi Sankyo.
Supporting information
Dataset: S1 Anonymized dataset of healthy gPV BRCA1/2 carriers. Includes clinical parameters, mutation status, and surgical history for all study participants.
Dataset: S2 Anonymized dataset of diseased gPV BRCA1/2 carriers. Includes clinical parameters, mutation status, and surgical history for all study participants.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Robert‐Koch‐Institut , “Krebs in Deutschland für 2019/2020, Brustdrüse,” 2023.
- 2J. Ettl and R. Würstlein , Manual Mammakarzinom, Empfehlungen zur Diagnostik, Therapie, Nachsorge und Begleitung (W. Zuckschwerdt, 2023), 401.
- 3K. B. Kuchenbaecker , J. L. Hopper , D. R. Barnes , et al., “Risks of Breast, Ovarian, and Contralateral Breast Cancer for BRCA 1 and BRCA 2 Mutation Carriers,” JAMA 317, no. 23 (2017): 2402–2416.28632866 10.1001/jama.2017.7112 · doi ↗ · pubmed ↗
- 4C. C. Riedl , N. Luft , C. Bernhart , et al., “Triple‐Modality Screening Trial for Familial Breast Cancer Underlines the Importance of Magnetic Resonance Imaging and Questions the Role of Mammography and Ultrasound Regardless of Patient Mutation Status, Age, and Breast Density,” Journal of Clinical Oncology 33, no. 10 (2015): 1128–1135.25713430 10.1200/JCO.2014.56.8626 PMC 5526626 · doi ↗ · pubmed ↗
- 5U. Bick , C. Engel , B. Krug , et al., “High‐Risk Breast Cancer Surveillance With MRI: 10‐Year Experience From the German Consortium for Hereditary Breast and Ovarian Cancer,” Breast Cancer Research and Treatment 175, no. 1 (2019): 217–228.30725383 10.1007/s 10549-019-05152-9 · doi ↗ · pubmed ↗
- 6F. Sardanelli , F. Podo , F. Santoro , et al., “Multicenter Surveillance of Women at High Genetic Breast Cancer Risk Using Mammography, Ultrasonography, and Contrast‐Enhanced Magnetic Resonance Imaging (The High Breast Cancer Risk Italian 1 Study): Final Results,” Investigative Radiology 46, no. 2 (2011): 94–105.21139507 10.1097/RLI.0b 013e 3181 f 3fcdf · doi ↗ · pubmed ↗
- 7I. J. Jacobs , U. Menon , A. Ryan , et al., “Ovarian Cancer Screening and Mortality in the UK Collaborative Trial of Ovarian Cancer Screening (UKCTOCS): A Randomised Controlled Trial,” Lancet 387, no. 10022 (2016): 945–956.26707054 10.1016/S 0140-6736(15)01224-6PMC 4779792 · doi ↗ · pubmed ↗
- 8S 3‐Leitlinie Diagnostik, Therapie und Nachsorge maligner Ovarialtumoren 2022. 161 p.