Fructosamine and HbA1c for Monitoring Diabetes in Pregnancy: Complementary or competing?
Yosra Htira, Chaima Jemai, Emna Fennira, Zohra Hadj Ali, Olfa Lajili, Imen Hedfi, Jihene Bettaieb, Faika Ben Mami

TL;DR
The study compares fructosamine and HbA1c as tools for monitoring blood sugar control in pregnant women with diabetes, finding they serve complementary roles.
Contribution
The study reveals that fructosamine and HbA1c have distinct but complementary roles in monitoring glycaemic control during pregnancy.
Findings
Fructosamine levels showed significant correlations with blood glucose levels across all three trimesters.
HbA1c was significantly correlated with blood glucose only in the first trimester.
Corrected fructosamine levels correlated with blood glucose in the first and second trimesters.
Abstract
This study aimed to perform a comparative evaluation of glycaemic control using fructosamine and glycated haemoglobin (HbA1c) and to investigate the correlations between the means of these biomarkers and mean glycaemia in pregnant women. This prospective longitudinal study was conducted from January to December 2020 and included pregnant women with pregestational diabetes, recruited at the National Institute of Nutrition of Tunis, Tunis, Tunisia, before 12 weeks of amenorrhoea and followed-up until delivery. A total of 71 pregnant women were included in this study. Glycaemic values decreased over the course of pregnancy and patients achieved better adherence to target glucose ranges. This improvement was statistically significant for fructosamine (P = 0.03) but not for HbA1c. Significant correlations were identified among mean HbA1c (P <0.001), fructosamine (P <0.001) and corrected…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
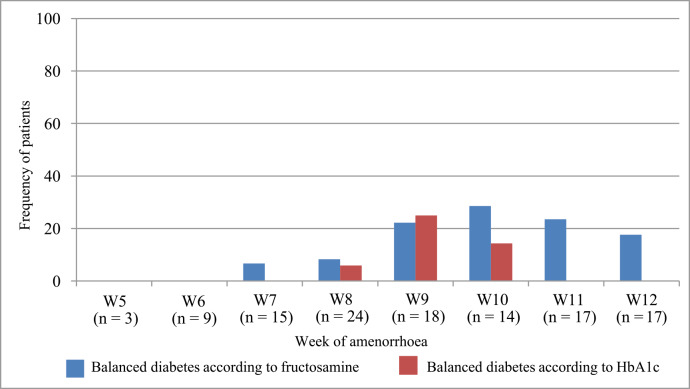 Fig. 1
Fig. 1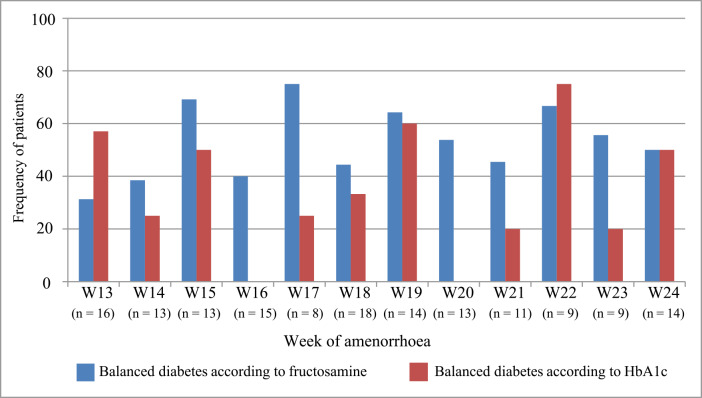 Fig. 2
Fig. 2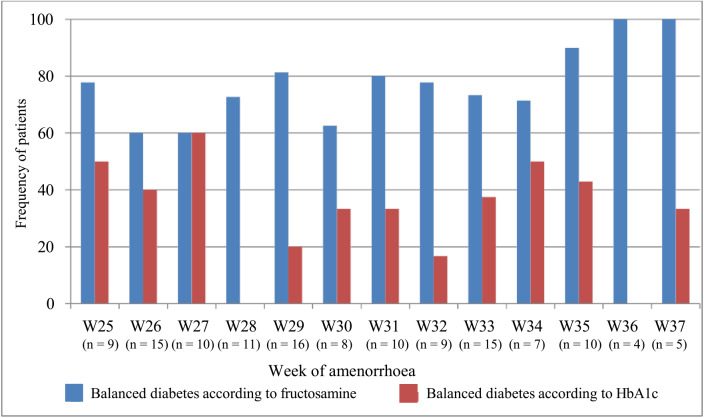 Fig. 3
Fig. 3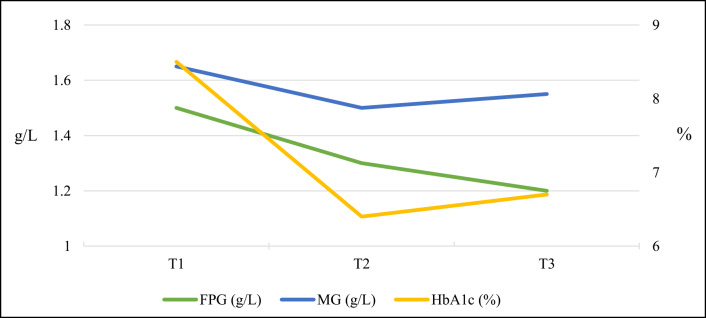 Fig. 4
Fig. 4| Variable | Mean ± SD |
|---|---|
| Age in years | 32.75 ± 4.71 |
| Frequency of patients older than 30 years | 77.4% |
| Duration of diabetes in years | 6.18 ± 6.18 |
| BMI in kg/m | 28.68 ± 5.28 |
| Frequency of type of diabetes | |
| T2DM | 55% |
| T1DM | 45% |
| Mean ± SD (range) | |||||
|---|---|---|---|---|---|
|
| |||||
| Trimester | FPG in g/L | MBG in g/L | FM in μmol/L | FMc in μmol/L | HbA1C in % |
| 1st trimester | 1.54 ± 0.53 (0.54–3.28) | 1.67 ± 0.44 (1.00–3.77) | 342.17 ± 84.85 (195–569) | 391 ± 90.79 (210.81–626.66) | 8.41 ± 1.91 (4.9–13.8) |
| 2nd trimester | 1.28 ± 0.34 (0.6–2.58) | 1.49 ± 0.35 (1.08–2.87) | 260.2 ± 49.07 (191.2–373.5) | 347.6 ± 71.5 (229.53–501.7) | 6.43 ± 1.07 (4.55–9) |
| 3rd trimester | 1.15 ± 0.33 (0.64–2.64) | 1.53 ± 0.46 (0.72–2.87) | 277.82 ± 46.85 (154.67–350) | 334.63 ± 81.89 (217.5–550.66) | 6.76 ± 1.52 (4.7–12) |
| % | |||||
|---|---|---|---|---|---|
|
| |||||
| Parameter | 1st trimester | 2nd trimester | 3rd trimester | OR (95% CI) | |
| HbA1c within target | 5.65 | 34.61 | 32.07 | 0.57 | – |
| FMc within target | 13.36 | 52.85 | 77.44 | 0.03 | 21.7 (7.7–61.5) |
| Biomarker | Trimester | Correlation with FPG | Correlation with MBG | ||
|---|---|---|---|---|---|
| HbA1c | 1st | r = 0.450 | 0.026 | r = 0.483 | <0.001 |
| 2nd | r = 0.279 | 0.105 | r = 0.254 | 0.14 | |
| 3rd | r = 0.120 | 0.945 | r = 0.379 | 0.09 | |
| FM | 1st | r = 0.468 | <0.001 | r = 0.523 | <0.001 |
| 2nd | – | – | r = 0.494 | <0.001 | |
| 3rd | – | – | r = 0.348 | 0.03 | |
| FMc | 1st | r = 0.482 | <0.001 | r = 0.511 | <0.001 |
| 2nd | r = 0.354 | <0.001 | r = 0.560 | <0.001 | |
| 3rd | – | – | r = 0.406 | 0.01 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGestational Diabetes Research and Management · Diet, Metabolism, and Disease · Hyperglycemia and glycemic control in critically ill and hospitalized patients
1. Introduction
Glycaemic control in pregnant women is typically monitored through regular assessment of glycaemic cycles, which enables daily therapeutic adjustments. In addition, long-term markers such as glycated haemoglobin (HbA1c) are used. Since the standardisation of its measurement, HbA1c has been regarded as the gold standard for evaluating glycaemic control.^123^ HbA1c reflects glycaemic control over the preceding 2–3 months, corresponding to the average half-life of a red blood cell.^45^
Fructosamine (FM), on the other hand, is a reflection of glycaemic control over a shorter period of time, approximately 1–3 weeks, corresponding to the half-life of serum albumin.^67^ FM, also referred to as 1-amino-1-deoxy fructose, is a collective term for glycated proteins, which limits its specificity.^8^ Albumin constitutes 60–70% of serum proteins and is the primary component of FM, resulting in shared properties.^4^ FM, or glycated albumin, is a ketoamine formed through the non-enzymatic glycation of the free amino group of proteins, predominantly albumin, by glucose. Measurement of FM has been recommended since 1982 by Johnson et al.^9^ The extent of glycation is determined by blood glucose concentration.^4^
FM measurement is considered appropriate in situations where HbA1c results are unreliable, including iron deficiency anaemia, haemoglobinopathies, haemorrhage, transfusion, liver failure, chronic renal failure and pregnancy.^10^ It is also valuable when short-term glycaemic control information is required, such as in the management of diabetic pregnancy.^111213^ However, FM measurement has not achieved the same level of adoption as HbA1c in diabetes monitoring, although several studies suggest it may offer superior performance in certain contexts.^1415^
To date, very few studies have directly compared FM and HbA1c head-to-head, highlighting a significant gap in the literature. Most of the existing research evaluating glycaemic markers such as FM and HbA1c during pregnancy has been conducted in Western populations. These studies, while informative, have inherent limitations in their generalisability to non-Western settings due to differences in genetics, ethnicity, nutritional patterns and healthcare systems. In contrast, Tunisia, as a North African country with distinct socio-economic conditions and a rising burden of diabetes and gestational diabetes, presents a unique epidemiological context. Tunisian pregnant women exhibit specific metabolic profiles influenced by local dietary habits, cultural factors and access to antenatal care, which may affect the dynamics and clinical interpretation of glycaemic biomarkers. Locally generated data are essential to accurately assess and validate the use of FM and HbA1c in monitoring diabetes during pregnancy within this population. Therefore, this study aimed to fill this critical gap by providing evidence relevant to the Tunisian context, ultimately contributing to more effective, culturally tailored diabetes management strategies.
2. Methods
This prospective longitudinal study was conducted from January to December 2020 at the National Institute of Nutrition of Tunis, Tunis, Tunisia. Pregnant women with diabetes mellitus (both type 1 and type 2) and those who provided informed consent were included; the participants were recruited before 12 weeks of gestation. Recruitment was conducted among patients presenting for medical follow-up. Patients with gestational diabetes mellitus as per the American Diabetes Association (ADA), those with conditions that could affect HbA1c or FM levels, including severe iron-deficiency anaemia (≤9 g/dL), haemolytic anaemia, haemoglobinopathies, a history of haemorrhage or transfusion, major hypertriglyceridemia (triglyceride [TG] ≥15 mmol/L), chronic renal failure or nephrotic syndrome, chronic liver disease, chronic thyroid disorders or protein-malnutrition states were excluded.^16^
Follow-up was conducted through biweekly consultations. At inclusion, all patients were interviewed to collect demographic data and diabetes history. Patients performed weekly blood glucose monitoring cycles, with 7 measurements per cycle: before and 2 hours after each main meal and at bedtime. The patients recorded blood glucose levels in a self-monitoring logbook; 2-week and quarterly averages of fasting plasma glucose (FPG) and mean blood glucose (MBG) were subsequently calculated. Glycaemic targets and insulin titration and hypoglycaemia severity were implemented in accordance with ADA guidelines;^16^ dietitians delivered individualised nutritional interventions to all included patients.
All assays were performed on fasting whole venous blood samples collected after an 8-hour fast at the laboratory of the same institution. Glycaemic monitoring encompassed quarterly HbA1c determination, with therapeutic targets aligned to the ADA 2024 criteria, namely HbA1c <6% in the absence of clinically relevant hypoglycemia.^16^
The HbA1c measurement was performed using the Adams® A1C system (ARKRAY, Inc., Kyoto, Japan). The assay employed ion-exchange high-performance liquid chromatography (HPLC) on a Tosoh G8 analyzer (Tosoh Bioscience, Inc., Grove City, Ohio, USA). According to the International Federation of Clinical Chemistry (IFCC), the reference method combines reverse-phase HPLC with mass spectrometry or capillary electrophoresis following enzymatic hydrolysis of haemoglobin. This rigorous analytical method provides a more specific measurement of HbA1c, with reduced interference from other glycated haemoglobins, resulting in generally lower values. The IFCC method has been endorsed by several professional organisations, including the ADA, European Association for the Study of Diabetes and National Glycohemoglobin Standardization Program and is recommended as the calibration standard for devices from different manufacturers. However, its implementation still raises questions and concerns.^17^
FM was assayed at bimonthly intervals. In non-diabetic pregnant women, the reference concentration is 2.20 ± 0.19 mmol/L. Accordingly, the study threshold was established at ≤2.58 ± 2 SD mmol/L.^18^
The FM assay was performed on a Cobas 6000 analyzer (Roche, Basel, Switzerland) using the automated colorimetric method originally described by Johnson.^19^ This technique is based on the reducing properties of Amadori rearrangement products in an alkaline medium. Under alkaline conditions, FMs are converted into eneaminols, which subsequently reduce the chromogen nitroblue tetrazolium (NBT) to a purple formazan. The rate of colour formation, measured spectrophotometrically, is directly proportional to the concentration of ketoamines.
This method was further optimised following the work of Siedel et al. (Fructosamine Plus).^20^ The incorporation of surfactants and the enzyme uricase substantially reduced analytical interferences from TGs and uric acid. Additional modifications compared to the earlier technique include: the use of a 0.2 mol/L carbonate buffer instead of 0.1 mol/L; an improved NBT reagent supplemented with uricase and a detergent; spectrophotometric reading at 550 nm instead of 530 nm; and replacement of the former calibrator (40 g/L albumin + DOMF) with secondary protein standards traceable to in vitro–glycated albumin and polysilane.
Major sources of analytical error include significant haemolysis or elevated bilirubin concentrations (>34 μmol/L). Overall, this method is readily adaptable to a wide range of automated biochemical analyzers.^21^
Serum albumin was measured fortnightly. Albumin concentrations were measured on a UniCell® DxC 600 analyzer (Beckman Coulter, Brea, California, USA) using a standard colorimetric assay. In this study, albumin (Alb) quantification was used to derive corrected FM (FMc) from measured FM (FMm), thereby enabling evaluation of the impact of haemodilution on FM values. FMc was calculated according to the following formula:^22^
Mean values of FM, FMc and HbA1c were calculated for each trimester of pregnancy.
Data entry and analysis were performed using Statistical Package for Social Sciences (SPSS) software, Version 23 (IBM Corp., Armonk, New York, USA). The distributions of continuous variables were assessed with the Kolmogorov–Smirnov and Shapiro–Wilk tests. Data were presented as percentages for categorical variables and as means with standard deviations for continuous variables. Comparisons of means were performed using Student's t-test for independent samples, and comparisons involving more than two groups were conducted using the non-parametric Kruskal–Wallis test. Percentages were compared using Pearson's Chi-square test and when its assumptions were not met, Fisher's exact two-tailed test was applied.
Associations between FPG, mean glucose (MG), FM, FMc and HbA1c levels were assessed using Spearman's non-parametric correlation coefficient. For all statistical analyses, P ≤ 0.05 was considered statistically significant.
3. Results
A total of 71 pregnant women were included in this study. The mean age was 32.75 ± 4.71 and 77.4% of the participants were older than 30 years [Table 1]. Glycaemic control improved from the first to the third trimester with decreases in fasting glucose (1.54 ± 0.53 versus 1.15 ± 0.33 g/L), FM (342.17 ± 84.85 versus 277.82 ± 46.85 μmol/L) and HbA1c (8.41 ± 1.91 versus 6.76 ± 1.52%). It appears to be due to intensive management by lifestyle and drugs/insulin [Table 2]. The proportion of patients achieving HbA1c targets increased from the first to later trimesters but without statistical significance (5.65 versus 32.07%; P = 0.57). FM target achievement improved significantly from 13.36% in the first trimester to 77.44% in the third trimester (P = 0.03), with a high odds ratio (odds ratio = 21.7, 95% confidence interval: 7.7–61.5) [Table 3]. Significant correlations were identified among mean HbA1c (P <0.001), FM (P <0.001) and FMc levels (P <0.001). Trimester-specific analyses indicated that mean HbA1c was significantly correlated with fasting and mean blood glucose levels exclusively in the first trimester. FM levels exhibited significant positive correlations with fasting and mean blood glucose levels during the first trimester (r = 0.468 and r = 0.523, respectively; P <0.001) as well as with mean blood glucose levels in the second (r = 0.494; P <0.001) and third trimesters (r = 0.348; P = 0.03). FMc levels were significantly positively correlated with mean fasting and mean blood glucose levels in the first (P <0.001) and second trimesters (P <0.001) and with mean blood glucose levels in the third trimester (P = 0.01) [Table 4]. Fig. 1,Fig. 2,Fig. 3 This study also illustrated diabetes control based on FM levels and HbA1c across weeks of amenorrhoea in each trimester [Fig. 1,Fig. 2,Fig. 3]. Furthermore, the overall trends of HbA1c, fasting plasma glucose and mean blood glucose throughout pregnancy are shown, highlighting changes in glycaemic markers as gestation progresses [Fig. 4].
Diabetes control according to fructosamine levels and glycated haemoglobin per week of amenorrhoea in the first trimester. W = week of amenorrhoea; HbA1C = glycated haemoglobin
Diabetes control according to fructosamine levels and glycated haemoglobin per week of amenorrhoea in the second trimester. W = week of amenorrhoea; HbA1C = glycated haemoglobin
Diabetes control by fructosamine levels and glycated haemoglobin per week of amenorrhoea in the third trimester.W = week of amenorrhoea; HbA1C = glycated haemoglobin.
Trends in glycated haemoglobin, fasting plasma glucose and mean blood glucose per trimester during pregnancy.T = trimester; FPG = fasting plasma glucose; MG = mean blood glucose; HbA1c = glycated haemoglobin.
4. Discussion
This study showed that FPG, MBG, FM and FMc levels decreased progressively from the first to the third trimester. HbA1c values also declined after the first trimester, indicating improved glycaemic control during pregnancy. FM and HbA1c levels correlate closely with glycaemic control throughout pregnancy. Both markers decrease progressively from the first to the third trimester, reflecting improved glucose regulation. These trends highlight their usefulness in monitoring diabetes during pregnancy and likely reflect metabolic adaptations and effective diabetes management across gestation. Overall, the data suggest better glucose regulation as pregnancy advances. FM target achievement improved significantly from the first trimester to the third trimester but HbA1c target rates increased modestly. These results suggest that FM is a more sensitive marker of glycaemic control during pregnancy.
These patterns are consistent with previous studies by Seddik and Pasi et al.^2324^ While HbA1c did not change significantly, FM markers (FM and FMc) showed clearer improvement, with a significant rise in the proportion of FM values within target ranges. This aligns with Parfitt et al. and Roslic et al., who reported that FM responds more rapidly to short-term glycaemic fluctuations than HbA1c.^825^ The current study also found strong correlations between HbA1c, FM and FMc throughout pregnancy, consistent with earlier findings in diabetic pregnancies.^182427^ However, HbA1c correlated with fasting and mean glucose only in the first trimester, in line with observations by Parfitt et al. and Kennedy et al.^2528^ In contrast, FM and FMc maintained significant correlations with glucose measures across trimesters, supporting evidence that FM-based markers offer better short-term glycaemic assessment, particularly when HbA1c becomes less reliable later in pregnancy.
Across pregnancy trimesters, this study found that FM and FMc consistently demonstrated stronger and more significant correlations with both FPG and MG levels compared to HbA1c. In the first trimester, all 3 biomarkers were significantly correlated with glycaemic measures, but from the second trimester onward, HbA1c lost its association with both FPG and mean glucose. In contrast, FM and FMc maintained significant positive correlations with mean glucose in both the second and third trimesters, with FMc showing the strongest associations (up to r = 0.560; P <0.001). Additionally, HbA1c remained strongly correlated with FM and FMc throughout pregnancy. These findings highlight the superior sensitivity of FM-based markers for reflecting short-term glycaemic changes, particularly in late pregnancy when HbA1c becomes less reliable.
In fact, during pregnancy, several physiological changes can affect the reliability of HbA1c as a marker of glycaemic control. Increased red blood cell turnover and a shortened erythrocyte lifespan reduce the time available for haemoglobin glycation, potentially leading to an underestimation of average blood glucose levels by HbA1c. Additionally, plasma volume expansion causes haemodilution, which lowers haemoglobin concentration and may distort HbA1c measurements. Iron deficiency anaemia, common in pregnancy, further alters erythropoiesis and haemoglobin glycation dynamics, thereby influencing HbA1c values independent of glycemia. Moreover, rapid fluctuations in glucose metabolism during gestation can limit HbA1c's capacity to reflect short-term glycaemic changes accurately.^10111213^ These factors highlight the potential benefit of alternative biomarkers, such as FM, which reflects glycaemic control over a shorter period and is less affected by erythrocyte turnover and plasma volume changes.^29^
The current study provides valuable insight into the complementary roles of FM and HbA1c in monitoring glycaemic control during pregnancy, a period marked by significant physiological changes that may affect biomarker reliability. The finding that FM showed statistically significant improvement over pregnancy while HbA1c did not aligns with evidence that HbA1c may be less sensitive to short-term glycaemic fluctuations due to altered red blood cell turnover and haemodilution in pregnancy. The significant correlations of FM with mean blood glucose across all trimesters reinforce its utility as a short-term glycaemic marker, consistent with studies suggesting FM better reflects recent glycaemic status compared to HbA1c during gestation. The limited correlation of HbA1c with glycemia beyond the first trimester underscores its potential limitations during later pregnancy stages.
Despite notable limitations in this study, including a small sample size, the absence of control subjects and the adjustment of FM for albumin levels, this inaugural prospective longitudinal study conducted in Tunisia demonstrates the potential value of FM in monitoring diabetic pregnancies. The findings indicate that FM and HbA1c capture different time frames of metabolic control. Therefore, the selection between HbA1c and FM should be guided by the specific need to evaluate either short-term or long-term glycaemic control. The implementation of FM may improve adherence among diabetic patients, leading to a reduction in the frequency of capillary blood glucose tests required and resulting in substantial healthcare cost savings.
5. Conclusion
FM and HbA1c provide complementary information for assessing glycaemic control during pregnancy in women with diabetes. Given the physiological changes that can affect HbA1c reliability, FM may serve as a useful adjunct marker, particularly for short-term monitoring. Further research is warranted to validate these findings in larger, diverse populations and to establish standardised guidelines for integrating FM into routine prenatal diabetes care.
Authors' contribution
Yosra Htira: Conceptualization, Methodology, Resources, Writing - Original Draft, Review & Editing. Chaima Jemai: Conceptualization, Methodology, Resources, Writing - Original Draft, Review & Editing. Emna Fennira: Conceptualization, Methodology, Resources, Writing - Original Draft, Review & Editing. Olfa Lajili: Resources, Writing - Original Draft. Jihene Bettaieb: Methodology, Resources, Writing - Original Draft. Zohra Hadj Alif: Resources, Writing - Original Draft. Imen Hedfi: Resources, Writing - Original Draft. Faika Ben Mami: Conceptualization, Supervision, Review & Editing.
Ethics statement
The National Institute of Nutrition of Tunis approved this study (code: N02/24). Written informed consent was obtained from all patients prior to participation. The study was conducted in accordance with the principles of the Declaration of Helsinki.
Conflict of interest
The authors declare no conflicts of interest.
Funding
No funding was received for this study.
Data availability
Data is available upon reasonable request from the corresponding author.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hoelzel W Weykamp C Jeppsson JO Miedema K Barr JR Goodall I IFCC reference system for measurement of hemoglobin A 1c in human blood and the national standardization schemes in the United States, Japan, and Sweden: a method-comparison study. Clin Chem 2004; 50:166–74. https://doi.org/10.1373/clinchem.2003.024802.10.1373/clinchem.2003.02480214709644 · doi ↗ · pubmed ↗
- 2Little RR. Glycated hemoglobin standardization-National Glycohemoglobin Standardization Program (NGSP) perspective. Clin Chem Lab Med 2003; 41:1191–8. https://doi.org/10.1515/CCLM.2003.183.10.1515/CCLM.2003.18314598869 · doi ↗ · pubmed ↗
- 3Radin MS. Pitfalls in hemoglobin A 1c measurement: when results may be misleading. J Gen Intern Med 2014; 29:388–94. https://doi.org/10.1007/s 11606-013-2595-x.10.1007/s 11606-013-2595-x 24002631 PMC 3912281 · doi ↗ · pubmed ↗
- 4Hashimoto K Koga M. Indicators of glycemic control in patients with gestational diabetes mellitus and pregnant women with diabetes mellitus. World J Diabetes 2015; 6:1045–56. https://doi.org/10.4239/wjd.v 6.i 8.1045.10.4239/wjd.v 6.i 8.104526240701 PMC 4515444 · doi ↗ · pubmed ↗
- 5Makris K Spanou L. Is there a relationship between mean blood glucose and glycated hemoglobin? J Diabetes Sci Technol 2011; 5:1572–83. https://doi.org/10.1177/193229681100500634.10.1177/19322968110050063422226280 PMC 3262729 · doi ↗ · pubmed ↗
- 6Armbruster DA. Fructosamine: structure, analysis, and clinical usefulness. Clin Chem 1987; 33:2153–63. https://doi.org/10.1093/clinchem/33.12.2153.10.1093/clinchem/33.12.21533319287 · doi ↗ · pubmed ↗
- 7Kondaveeti SB Ivvala AS Chidambaram R. “Glycated albumin” a new paradigm in better monitoring Type 2 diabetes complications as a short-term glycemic index. J Invest Biochem 2014; 3:85–91. 10.5455/jib.20140718044724. · doi ↗
- 8Rosić B Sulović V Lazarević B Jevremović M Gligorović S Spasić S The estimation of fructosamine and Hb Alc in pregnant women with diabetes mellitus. Clin Exp Obstet Gynecol 1993; 20:189–91.8403429 · pubmed ↗