Adalimumab Therapy for Crohn's Disease and Axial Spondyloarthritis in Latent Tuberculosis: A bibliometric-systematic literature review
Nyimas Maida Shofa, Nurike Setiyari Mudjari, Rusdiyana Ekawati, Arianti Arianti, Annisa Zahra Mufida, Budi Widodo, Titong Sugihartono

TL;DR
This paper reviews the use of adalimumab for Crohn's disease and arthritis in areas with high tuberculosis risk, finding it effective but with some risk of TB reactivation.
Contribution
The study provides a bibliometric and systematic review of adalimumab's use in TB-endemic regions with concurrent TB prophylaxis.
Findings
Adalimumab achieved 60–85% clinical remission in moderate-to-severe Crohn's disease and axial spondyloarthritis.
1–3% of patients developed active TB despite screening and isoniazid prophylaxis.
Region-specific frameworks are needed for safe adalimumab use in TB-endemic areas.
Abstract
The management of Crohn's disease (CD) using anti-tumour necrosis factor therapy in tuberculosis (TB)-endemic regions poses major clinical challenges due to the risk of latent TB infection reactivation. This bibliometric–systematic literature review synthesised evidence from 17 peer-reviewed studies (2020–2025) evaluating adalimumab administered with concurrent prophylactic antitubercular therapy. Thematic synthesis and bibliometric mapping using VOSviewer demonstrated that adalimumab achieved 60–85% clinical remission in moderate-to-severe CD and axial spondyloarthritis while enhancing mucosal healing. However, 1–3% of patients developed active TB despite appropriate screening and isoniazid prophylaxis, revealing false-negative diagnostics and partial chemoprophylaxis protection. These findings highlight the need for region-specific frameworks integrating multimodal screening, targeted…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
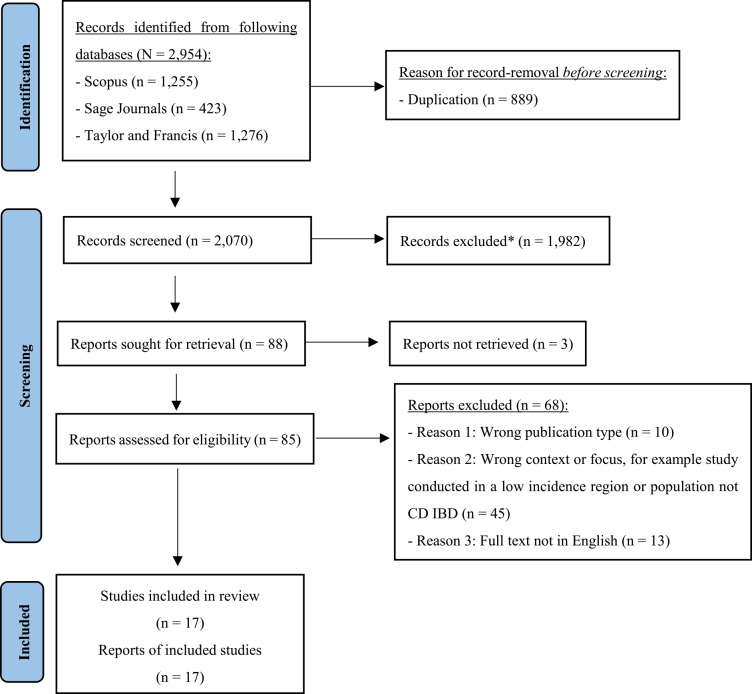 Fig. 1
Fig. 1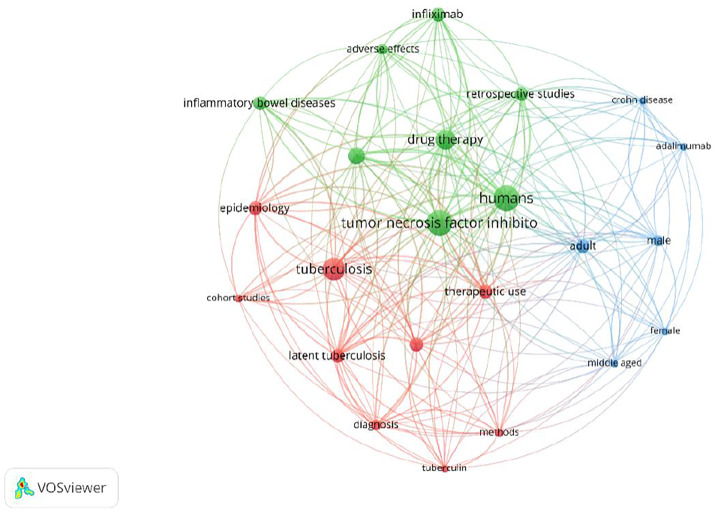 Fig. 2
Fig. 2| Framework | Inclusion criteria |
|---|---|
| Population | Patients diagnosed with CD or IBD, with or without extraintestinal manifestations like AxSpA, who also have LTBI or are at high risk for TB. |
| Intervention | Treatment with adalimumab or other anti-TNF agents, administered concurrently with or after prophylactic therapy for LTBI (e.g., INH, rifampicin). |
| Comparison | Placebo, no anti-TNF treatment, conventional IBD therapies, or alternative biologic agents. Comparisons could also be between different screening or prophylaxis strategies. |
| Outcome | Effectiveness: Clinical remission of CD and/or AxSpA, mucosal healing, reduction in inflammatory markers. Safety: Incidence of TB reactivation, adverse events related to anti-TNF therapy or INH prophylaxis, treatment discontinuation rates. |
| Context | Studies conducted in TB-endemic regions (e.g., Asia, Latin America, Africa) or involving patient populations with a high risk of TB exposure. |
| Author and year of publication | Study design, country | Population and key comorbidities | Intervention (anti-TNF & prophylaxis) | Key TB-related outcome |
|---|---|---|---|---|
| Freitas Cardoso de Azevedo | Retrospective case-control, Brazil (high TB burden) | 152 IBD patients: 38 TB cases, 114 controls; 81.6% CD | 86.1% of TB cases on anti-TNF; 71% also on thiopurines/methotrexate; some received 6–9 months INH based on TST | Anti-TNF ↑ TB risk (OR = 3.36); onset median 32 months; new TB infections may be more common than reactivation; restarting anti-TNF post-TB generally safe. |
| Barros | Case report, Brazil | 38F, 8-year fistulising ileocolonic & perianal CD, 2 prior small bowel resections | Adalimumab + azathioprine (5 years), baseline TST & CXR negative, no prophylaxis | Developed disseminated TB (tongue involvement); highlights risk of severe extrapulmonary TB despite negative screening |
| Matran | Retrospective single-centre, Romania (highest TB burden in EU) | Paediatric IBD cohort (n = 40), 55% CD, median age = 14.8 years | Infliximab (85%), adalimumab (15%); 1 case on adalimumab + azathioprine, baseline IGRA negative | Severe bronchopulmonary TB 30 months after therapy; illustrates difficulty distinguishing reactivation versus new infection in high-burden areas |
| Banerjee | Non-systematic literature review, TB-endemic focus (Asia) | IBD patients (CD & UC) from endemic regions | Anti-TNF (infliximab, adalimumab) & newer biologics; guidelines recommend LTBI screening & prophylaxis ≥3–4 weeks before therapy | Anti-TNF ↑ TB reactivation risk; 1–3% develop active TB, some despite negative LTBI screening |
| Kim | Multicentre retrospective, South Korea (intermediate TB burden) | 25 IBD patients with TB on anti-TNF versus 75 TB patients w/o IBD; ~⅔ had CD | Infliximab (96%); 3 LTBI+ received 9-months INH (2 completed), all developed pulmonary TB | TB outcomes similar to non-IBD TB; prophylaxis failed in all LTBI+ cases |
| Kim | Nationwide retrospective cohort, South Korea (intermediate TB incidence) | 6,123 IBD patients starting biologics; 58.9% CD | Compared anti-TNF versus non-anti-TNF (vedolizumab, ustekinumab); screening policy in place, prophylaxis data not reported | TB incidence lower with non-anti-TNF (0.37 versus 0.87/100 PY), trend toward reduced risk but not statistically significant |
| Alrajhi | Systematic review & meta-analysis (16 studies, international) | 2,488 IBD patients screened for LTBI before anti-TNF | Evaluated TST & IGRA; assessed effect of immunosuppressants (steroids, thiopurines) on sensitivity | IGRA sensitivity ↓ with immunosuppressants (OR = 0.57) → higher false-negative risk if used alone in immunosuppressed IBD patients |
| Ikuta | Case report, Japan. | 79F, RA → suspected CD | Adalimumab; LTBI+ (T-SPOT.TB); completed 6-months INH (300 mg/day) before therapy | Developed disseminated intestinal TB despite prophylaxis → shows prophylaxis may not fully prevent reactivation |
| Calzada-Hernández | Multicentre cohort, Spain (low TB burden) | 270 paediatric IMIDs: 55.9% rheumatologic, 34.8% IBD | Dual LTBI screening (TST + QuantiFERON); LTBI + received prophylaxis, incl. 1 with 9-months INH | Effective over 6.4 years; 2 probable de novo TB, 1 disseminated TB after INH due to reinfection |
| Mohagheghi Darehranj | Retrospective observational, Iran | 315 moderate-severe IBD patients; 48.9% CD, 7.3% musculoskeletal EIMs | Anti-TNF (infliximab, CinnoRA®); LTBI screening/prophylaxis not reported | No TB or serious opportunistic infections during follow-up |
| Coskunol | Retrospective, Turkey (high TB prevalence) | 520 autoimmune patients: 51% AS, 6.7% CD. 1.9% UC | Various anti-TNF; all TB cases on infliximab; 2 completed 9-months INH, 1 completed 6-months INH | TB in 0.96% (5 cases); 3 UC cases; 3 TB developed despite prophylaxis → possible prophylaxis failure |
| Hisamatsu | Multicentre post-marketing surveillance, Japan | 389 moderate-severe CD patients; 29% with EIMs | Adalimumab up to 3 years; LTBI screening/prophylaxis not reported | No de novo TB or LTBI reactivation; no hepatitis B reactivation |
| Cardoso da Silva | Case report, Brazil (high TB burden) | 38M, colonic CD, occupational TB exposure | Adalimumab; baseline CXR & TST negative; no prophylaxis | Developed pulmonary TB 3 months after therapy; shows limits of conventional LTBI screening in high-risk patients |
| Vuyyuru | Retrospective cohort, India (TB-endemic) | 59 stricturing CD patients; 69.5% ileum, 18.6% EIMs | Infliximab 84.7%, adalimumab 15.3%; all TB cases had prior LTBI screening; prophylaxis details not given | TB reactivation in 5.1% (n = 3) despite prior screening; highlights high risk in endemic settings |
| Lee | Retrospective cohort, South Korea | 1,434 IBD patients; 76.8% CD | Infliximab, adalimumab, golimumab; LTBI screening in 93%, 96% of positives got prophylaxis | B in 1.46% (n = 21), incl. 3 post-prophylaxis; older age ↑ TB risk; effective LTBI management ↓ TB incidence |
| Ye | Multicentre retrospective cohort, China (TB-endemic) | 1,968 IBD patients; 90% CD | All on infliximab; compared targeted versus universal prophylaxis (6-months INH or 3-months INH+rifampicin) | No TB incidence difference; universal strategy ↑ adverse events; 2.6% LTBI+ developed TB despite prophylaxis → incomplete protection |
| Üzer | Cross-sectional, Turkey | 661 patients screened for TB; ~50% pre-anti-TNF (24.2% rheumatologic, 6.6% IBD) | LTBI screening via TST and/or QuantiFERON; 28.3% got prophylaxis (mostly 9-months INH) | TB in 1.2% of pre-anti-TNF cases; >50% had anergic TST (esp. immunosuppressed) → IGRA valuable for detection |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfectious Diseases and Tuberculosis · Diagnosis and treatment of tuberculosis · Tuberculosis Research and Epidemiology
1. Introduction
Crohn's disease (CD) is a chronic, immune-mediated inflammatory disorder characterised by transmural inflammation of the gastrointestinal tract. Its pathogenesis involves a dysregulated immune response to intestinal microbiota influenced by genetic and environmental factors.^1^ The incidence of Crohn's disease continues to increase worldwide, with particularly steep upward trends reported in newly industrialised Asian countries, reflecting a broader shift in the global epidemiology of inflammatory bowel disease.^2345^ Beyond intestinal inflammation, patients frequently experience extraintestinal manifestations such as axial spondyloarthritis (AxSpA), which considerably impairs quality of life and complicates disease management.^678^
Biologic therapies, particularly tumour necrosis factor alpha inhibitors such as adalimumab and infliximab, have transformed the management of moderate-to-severe Crohn's disease by improving long-term clinical outcomes and enabling mucosal and, in some patients, histological healing.^91011^ However, because TNF alpha is pivotal for the formation and maintenance of granulomas that contain latent Mycobacterium tuberculosis, anti TNF therapy is associated with a substantially increased risk of progression from latent tuberculosis infection to active disease, a concern that is particularly salient in tuberculosis endemic settings such as Indonesia and wider Asia.^1213141516^ While international and the World Health Organization guidelines recommend comprehensive LTBI screening and prophylaxis before initiating anti-tumour necrosis factor (anti-TNF) therapy, they primarily address general population TB control and are not specifically designed for immunosuppressed patients with inflammatory bowel disease (IBD).^917^ Consequently, their applicability to clinical decision-making in this subgroup remains limited, particularly in defining optimal screening algorithms, timing of prophylaxis and management of false-negative results.
Screening tools such as interferon-gamma release assays (IGRAs) are preferred for their specificity, yet their sensitivity may be compromised in immunosuppressed individuals, leading to false-negative results and potential undetected TB reactivation.^18^ Likewise, isoniazid (INH) prophylaxis, though effective, carries hepatotoxic and possible profibrotic risks, adding uncertainty to treatment safety.^1920^ Furthermore, diagnostic overlap between CD and intestinal TB remains a persistent challenge in high-burden regions.^21^
Despite these challenges, there is a marked paucity of region-specific evidence detailing how concurrent administration of adalimumab and INH prophylaxis can be safely implemented in TB-endemic contexts. Most studies originate from Western or East Asian populations, leaving a considerable gap in data from Southeast Asia, particularly Indonesia, where both TB and IBDs are increasingly prevalent. Therefore, this review aimed to synthesise and evaluate current evidence regarding the safety and effectiveness of adalimumab therapy combined with LTBI prophylaxis in patients with CD and AxSpA in high-TB-burden settings, while proposing an evidence-based framework for safer biologic therapy in such environments.
2. Methods
This study adopted a hybrid B-SLR design, combining PRISMA-based qualitative synthesis with bibliometric mapping to capture both content-level insights and structural patterns across the included literature. The B-SLR approach was employed to systematically identify, evaluate and synthesise the most current and relevant scholarly literature on the management of CD with adalimumab in patients with LTBI, particularly within high-burden and TB-endemic regions. This review did not include any primary case report authored by the investigators; all analysed studies were previously published, peer-reviewed literature identified through systematic database searching.
2.1. Search strategy and data sources
A systematic literature search was performed across 4 major academic databases: Scopus, Sage Journals, Taylor & Francis and PubMed/MEDLINE. The search strategy was designed to be comprehensive and utilised a primary Boolean search string: (“Crohn's Disease” OR “Inflammatory Bowel Disease”) AND (“Tuberculosis” OR “Latent Tuberculosis” OR “LTBI”) AND (“Adalimumab” OR “Anti-TNF” OR “TNF inhibitor”). To ensure all relevant studies on prevention were captured, a second, more focused string was also used: (“Crohn's Disease” AND “Latent Tuberculosis” AND (“Prophylaxis” OR “Isoniazid”) AND “Adalimumab”). The search was not restricted by publication date initially to include foundational studies, though priority was given to literature published between 2020 and 2025 to ensure the currency of the evidence.
2.2. Eligibility criteria
To precisely define the scope of the literature search and ensure a focused review, the study's research questions were structured using the Population, Intervention, Comparison, Outcome and Context (PICOC) framework.
Based on the PICOC framework, this review targeted studies involving patients with CD or IBD who were at high risk for or diagnosed with LTBI. The primary intervention of interest was treatment with adalimumab or other anti-TNF agents in conjunction with LTBI prophylaxis. The review was designed to assess both the therapeutic effectiveness of this strategy in managing the inflammatory disease and its safety profile, specifically the incidence of TB reactivation. Critically, the context was limited to TB-endemic regions or high-risk populations to ensure the findings would be relevant to the clinical challenges faced in these settings. Following the establishment of the conceptual scope, a formal set of inclusion and exclusion criteria was developed to guide the practical selection of articles during the screening process. Based on the PICOC framework, a formal set of inclusion and exclusion criteria was developed to guide the practical selection of articles and ensure a methodologically rigorous review. To maintain the currency of the evidence, the review prioritised studies published between 2020 and 2025; however, foundational earlier studies were considered for inclusion if they provided critical insights into TB risk or management, while those published outside this period lacking such relevance were excluded. The selection was restricted to peer-reviewed primary research (e.g., cohort, case-control, case series) and secondary research (e.g., systematic reviews, meta-analyses) to ensure a high standard of evidence. Consequently, non-peer-reviewed materials such as preprints, dissertations and editorials without original data were excluded. All publications were required to be written in English, with articles in any other language being ineligible for inclusion. Studies not involving IBD or anti-TNF therapy, not addressing TB, or conducted solely in low-incidence settings were excluded unless they specifically addressed high-risk populations [Table 1].
2.3. Study selection process
The selection of studies was conducted systematically and transparently, adhering to the 4-stage PRISMA framework. The initial database search yielded 4,454 records. After removing 1,354 duplicates, 3,100 unique articles were advanced to the screening phase. During this stage, titles and abstracts were reviewed, excluding 2,980 records that did not align with the research scope. The full texts of the remaining 120 articles were then sought for a detailed eligibility assessment. Following this rigorous review against the predefined PICOC and inclusion/exclusion criteria, 103 articles were excluded. The primary reasons for exclusion were an inappropriate study context or population (n = 45), an unsuitable publication type such as an editorial (n = 10) or the full text not being available in English (n = 13). This meticulous filtering process resulted in a final cohort of 17 studies that were deemed highly relevant for inclusion in the qualitative synthesis [Fig. 1].
*PRISMA 2020 flow diagram showing study selection.CD = Crohn's disease; IBD = inflammatory bowel disease..Records excluded at the title and abstract screening stage; no automation tools were used.
2.4. Data synthesis and thematic analysis
A thematic synthesis approach was combined with bibliometric mapping using VOSviewer (Centre for Science and Technology Studies [CWTS], Leiden University, Leiden, The Netherlands) to identify conceptual patterns across the included studies. This hybrid B-SLR design integrates qualitative synthesis with quantitative keyword co-occurrence analysis, enabling the identification of both content-based insights and structural relationships within the literature. The use of VOSviewer (CWTS) allows visualisation of key thematic domains and interconnections, thereby supporting a more comprehensive understanding of how existing evidence on adalimumab therapy, LTBI management and TB risk converges in the scientific field.
Following the final selection, data from the 17 included studies were extracted and organised for qualitative synthesis. The primary objective was to consolidate findings related to the effectiveness and safety of adalimumab, challenges in LTBI screening and outcomes of prophylactic therapy. To visually map the thematic landscape and conceptual structure of the selected literature, a co-occurrence network analysis of keywords was conducted using VOSviewer software (CWTS). A total of 3 distinct but highly interconnected thematic clusters was found [Fig. 2]. The first cluster (green) centres on the primary therapeutic intervention and disease context, linking terms such as IBDs, drug therapy and tumour necrosis factor inhibitor. The second cluster (red) represents the core safety concern of this review, with TB and latent TB as central nodes connected to diagnosis and epidemiology. The third cluster (blue) defines the patient population, focusing on terms such as ‘humans’, ‘adult’ and the specific agent adalimumab. Crucially, the analysis highlights the central, bridging role of tumour necrosis factor inhibitor, which connects the therapeutic context with the primary complication of TB, thereby validating that the selected literature is appropriately focused on the key domains of this systematic review.
Network visualisation of thematic keyword clusters using VOSviewer (CWTS).
3. Results
3.1. Characteristics of included studies
A total of 17 studies published between 2020 and 2025 were included, encompassing a diverse range of designs including 9 retrospective cohort analyses, 3 case reports, 2 multicentre investigations, 2 observational studies and 1 systematic review with meta-analysis. The majority of studies originated from Asia (n = 9; Japan, South Korea, China, India, Iran and Turkey) and Latin America (n = 3; Brazil), with additional contributions from Europe (n = 3; Spain, Romania). Most were conducted in countries classified as having high or intermediate TB-burden, thereby providing regionally relevant insights into the intersection between CD and LTBI.
Across all studies, the predominant study population comprised patients diagnosed with moderate-to-severe CD, frequently complicated by extraintestinal manifestations such as AxSpA. The primary therapeutic intervention evaluated was anti-TNF biologic therapy, particularly adalimumab, either as monotherapy or in combination with conventional immunomodulators (e.g., azathioprine, thiopurines). Several studies also compared adalimumab to infliximab or newer biologics such as vedolizumab and ustekinumab. Most included cohorts implemented LTBI screening using either tuberculin skin tests (TSTs) or IGRAs, with INH prophylaxis being the most common preventive regimen [Table 2].
The publication landscape demonstrates a steady increase in research output on adalimumab therapy and TB risk among CD patients over the past 5 years, reflecting a growing clinical interest in managing biologic therapy within TB-endemic contexts. Cohort sizes ranged from 54 to over 1,000 participants, while case reports and smaller observational studies contributed important real-world perspectives on treatment safety and latent TB reactivation. Collectively, this geographic and temporal diversity underscores the global relevance and contemporary nature of the evidence base, particularly for countries with high TB burdens such as Indonesia.
3.2. Effectiveness of adalimumab therapy
Across the reviewed studies, adalimumab consistently demonstrated high clinical effectiveness in inducing and maintaining remission among patients with moderate-to-severe CD, including those with concomitant AxSpA. Cohort studies from Japan, South Korea and Iran reported sustained remission rates ranging from 60% to 85%, with significant improvements in both intestinal and extraintestinal manifestations.^222324^ The therapeutic response was observed across adult and paediatric populations, suggesting comparable efficacy irrespective of age group or disease duration.^25^ Several studies highlighted the superior drug persistence and mucosal healing rates associated with adalimumab compared to conventional immunomodulators, reinforcing its role as a cornerstone biologic in complex CD management.^26^ Moreover, adalimumab was reported to contribute to reduced inflammatory biomarkers and endoscopic healing in a majority of patients, underscoring its robust anti-inflammatory potential in real-world clinical settings.
3.3. Safety and tuberculosis reactivation risk
Despite its therapeutic efficacy, anti-TNF therapy such as adalimumab poses a well-documented risk of TB reactivation, particularly in endemic regions. Across the reviewed studies, the incidence of active TB among anti-TNF users ranged between 1% and 3%, even in cohorts implementing routine LTBI screening and prophylaxis.^92728^ Cases of active TB were typically observed within 6 to 30 months after initiating biologic therapy. The use of INH prophylaxis significantly reduced the risk of TB reactivation; however, it did not fully eliminate it. For instance, Ye et al. documented that 2.6% of patients who completed INH prophylaxis still developed TB, while Ikuta et al. reported disseminated intestinal TB in a patient despite a full 6-month INH course. Hepatotoxicity associated with INH was also noted in multiple studies, emphasising the need for careful liver function monitoring.^202930^ Comparative analyses revealed that non-anti-TNF biologics such as vedolizumab and ustekinumab were associated with lower TB risk, suggesting their potential as safer alternatives in high-risk populations.^31^ Collectively, these findings highlight that while concurrent INH prophylaxis enhances the safety profile of adalimumab, vigilance for breakthrough infections remains critical throughout the treatment course.
3.4. Integrated interpretation
The synthesised findings demonstrate that adalimumab remains an effective and viable therapeutic option for inducing and maintaining remission in patients with moderate-to-severe CD, including those with coexisting AxSpA, when implemented alongside appropriate LTBI prophylaxis. The evidence base affirms that the concurrent use of adalimumab and INH prophylaxis provides substantial clinical benefit; however, it also underscores the persistent challenge of TB reactivation, particularly in high-burden settings. The observed cases of breakthrough TB despite adequate chemoprophylaxis reflect the limitations of current screening modalities, specifically the reduced sensitivity of IGRAs and TSTs in immunosuppressed individuals.
Moreover, the synthesis suggests that a single-test diagnostic approach is insufficient, and a comprehensive, multimodal framework integrating clinical risk assessment, dual testing (IGRA and TST) and baseline imaging is warranted to improve LTBI detection accuracy. While newer biologics such as vedolizumab and ustekinumab may offer a more favourable safety profile, adalimumab continues to demonstrate superior efficacy and treatment durability in achieving mucosal healing and long-term disease control. These findings collectively indicate that the optimal management strategy for CD in TB-endemic regions should be dynamic and individualised, balancing potent immunosuppressive therapy against a continuously monitored infection risk.
The integrated interpretation highlights that, while the therapeutic value of adalimumab is clear, its safe implementation depends on a proactive and region-specific clinical protocol. Continuous surveillance, patient education and tailored prophylactic strategies are imperative to sustain therapeutic gains while minimising infectious complications in TB-endemic contexts such as Indonesia.
4. Discussion
4.1. Efficacy and safety of anti-TNF therapy with concurrent LTBI prophylaxis
The administration of anti-TNF agents, including adalimumab, has been established as a highly effective strategy for inducing and maintaining clinical remission in patients with moderate to severe IBD.^2324^ However, the therapeutic efficacy of these agents is intrinsically linked to a significant safety concern: an increased risk of TB reactivation.^9^ The administration of anti-TNF therapy has been demonstrated to elevate this risk, particularly in TB-endemic regions significantly.^2132^
Consequently, management guidelines universally mandate screening for LTBI before initiating therapy.^929^ However, the reliability of these screening methods in the IBD population is a critical challenge. A meta-analysis revealed that the performance of IGRAs can be negatively impacted by concurrent immunosuppressive therapy, potentially leading to false-negative results.^33^ This is compounded by the high rate of anergic responses to the TST in immunosuppressed individuals, often necessitating secondary testing with IGRA.^34^ Several reports documented cases where patients developed active TB despite having negative initial screens.^3536^
The cornerstone of mitigating TB risk is chemoprophylaxis for patients diagnosed with LTBI. The evidence reviewed, however, suggests that this strategy, although essential, is not entirely protective. Multiple studies within the reviewed literature documented cases of active TB developing in patients despite the completion of standard prophylactic regimens.^17202526^ A case report from Japan detailed the emergence of disseminated intestinal TB in a patient on adalimumab who had completed a 6-month course of INH prophylaxis.^30^ Furthermore, an extensive cohort study in China found that 2.6% of patients who received chemoprophylaxis for LTBI still developed active TB.^29^
Despite the risk of reactivation, the clinical prognosis for IBD patients who develop TB while on anti-TNF therapy appears to be comparable to that of the general population, provided that the anti-TNF agent is suspended and appropriate anti-TB treatment is promptly initiated.^27^ In summary, while concurrent adalimumab and INH prophylaxis can effectively manage the underlying inflammatory disease, its safety profile is complex. The strategy's success is contingent upon a rigorous and vigilant approach that acknowledges the limitations of initial screening and chemoprophylaxis's protective efficacy.
Beyond traditional anti-TNF agents, several next-generation biologics have emerged following extensive clinical evaluation. Head-to-head and network meta-analyses published between 2023 and 2024 demonstrated that ustekinumab, vedolizumab and risankizumab achieve comparable or superior clinical and endoscopic remission rates relative to adalimumab, while exhibiting a markedly lower risk of TB reactivation.^32383940^ In the SEAVUE trial and subsequent comparative studies, ustekinumab matched adalimumab in efficacy for both induction and maintenance phases, with improved treatment persistence and fewer serious infections.^4142^ Real-world analyses further revealed that vedolizumab provided similar remission outcomes but superior safety in biologic-naive CD patients.^4344^ Meanwhile, risankizumab, an IL-23 inhibitor, showed higher induction efficacy and mucosal healing compared to ustekinumab, reinforcing its potential role as a frontline agent.^3245^ Importantly, large-scale cohort data from Japan demonstrated that active TB cases occurred exclusively in anti-TNF-treated groups, whereas no TB reactivation was reported among patients receiving ustekinumab or vedolizumab.^46^ Collectively, these findings indicate that while adalimumab remains an accessible and effective therapeutic cornerstone, alternative biologics may offer comparable efficacy with enhanced safety profiles—an important consideration for clinicians in TB-endemic regions.
4.2. Clinical implications and risk management strategies for anti-TNF therapy in TB-endemic settings
The collective evidence drawn from recent literature presents profound clinical implications for the management of patients with CD on anti-TNF therapy in TB-endemic regions such as Indonesia. The overarching conclusion is that a direct application of Western-centric guidelines is insufficient and potentially hazardous. Instead, a more stringent, nuanced and proactive risk management framework must be adopted, tailored to the local epidemiological context. The primary challenge, as highlighted across multiple studies, lies in the inherent limitations of current screening protocols. While pre-treatment screening is mandatory, its reliability is compromised in this specific patient population. A meta-analysis by Alrajhi et al. demonstrated that the sensitivity of IGRA is significantly reduced by concurrent immunosuppressive therapy, leading to a higher risk of false-negative results.^33^ Similarly, the TST often yields anergic or indeterminate results in these patients.^34^ This diagnostic gap is critically important, as numerous case reports and cohort studies document the emergence of active TB despite negative initial screenings, underscoring that a negative test cannot be considered definitive proof of the absence of LTBI.^283536^ Consequently, the first strategic recommendation is a paradigm shift towards a multi-modal screening strategy. This approach should not rely on a single test but rather integrate a thorough assessment of clinical risk factors, baseline thoracic imaging, and the concurrent use of both TST and IGRA, a dual strategy that has been shown to identify more LTBI cases than either test alone.^47^
Furthermore, even when LTBI is correctly identified and treated, chemoprophylaxis does not confer absolute immunity, underscoring the need for ongoing risk management during anti-TNF therapy. The study by Ye et al. found that a universal prophylaxis strategy for all patients did not reduce TB incidence compared with a targeted strategy, but it significantly increased adverse events.^29^ This finding supports risk-stratified prophylaxis while reinforcing the need for sustained clinical vigilance and comprehensive patient education. The risk of TB is not confined to the initiation phase of therapy but persists over time; clinicians should recognise that new infections may occur during long-term treatment and that risk increases with age.^253648^ Patients should be educated about TB symptoms and instructed to report them promptly to facilitate early evaluation and intervention.
The collective evidence synthesised in this review carries substantial implications for clinical practice in TB-endemic countries such as Indonesia. The direct adoption of Western-centric IBD treatment guidelines may be inadequate or even unsafe without contextual adaptation. Given the limited reliability of existing screening tools and the variable success of prophylaxis, an individualised, region-specific framework is imperative. This framework should combine multimodal screening (dual IGRA/TST testing with baseline chest imaging), targeted prophylaxis based on risk stratification and continuous post-treatment surveillance. Such an approach aligns with the practical realities of healthcare infrastructure and epidemiologic risk in Southeast Asia, where latent TB remains a significant comorbidity among biologic-treated patients.
Recent advances in IBD therapeutics further reinforce the need to update clinical strategies. Emerging biologics and small-molecule agents—including IL-23 inhibitors such as risankizumab and mirikizumab, as well as Janus kinase (JAK) inhibitors such as tofacitinib and upadacitinib have demonstrated high efficacy for inducing and maintaining remission in CD and ulcerative colitis, with favourable safety profiles and rapid onset of action.^4950515253^ Meta-analyses confirm that IL-23 inhibitors achieve robust clinical and endoscopic remission while maintaining infection risks comparable to placebo, suggesting their potential suitability for TB-endemic settings.^5455^ However, access barriers, high costs and a scarcity of long-term safety data in high-burden populations currently limit their real-world implementation. In contrast, JAK inhibitors—though offering oral administration and non-immunogenic benefits carry notable risks of herpes zoster and venous thromboembolism, necessitating cautious patient selection.^56^
For TB-endemic countries, these developments underscore both opportunity and caution. While next-generation therapies hold promise for reducing infection-related complications seen with anti-TNF agents, limited pharmacovigilance data in Asian and African cohorts call for local evidence generation. Collaborative multicentre registries should be prioritised to assess TB reactivation rates and cost-effectiveness of newer biologics in high-risk populations. Ultimately, clinical decision-making must balance therapeutic innovation with contextual feasibility integrating cutting-edge therapies where possible, while reinforcing TB screening accuracy, patient monitoring and health system readiness to ensure safe and sustainable IBD management.
4.3. Limitations and strengths
This review has several methodological limitations that should be acknowledged. The heterogeneity of the included studies in terms of design, sample size and regional context restricted the possibility of quantitative pooling or meta-analytic comparison. Most studies were retrospective and small-scale, which may introduce selection and reporting biases. Additionally, the absence of standardised definitions and protocols for LTBI screening and prophylaxis across studies limits direct comparability of results. The review also relied primarily on English-language publications, which may have led to the exclusion of relevant regional data. Despite these constraints, the review has notable strengths. To the best of the authors' knowledge, this is the first B-SLR that integrates thematic synthesis with bibliometric mapping to analyse the intersection between biologic therapy, latent TB management, and CD in TB-endemic settings. The novelty of this research lies not only in its dual-method approach, which captures both conceptual patterns and clinical outcomes, but also in its emphasis on TB-endemic regions, offering contextually relevant insights that can bridge an important evidence gap for countries such as Indonesia. Furthermore, the synthesis encompasses both adult and paediatric populations and incorporates the most recent evidence (2020–2025), ensuring that conclusions reflect current clinical practices and diagnostic standards. These strengths enhance the credibility and applicability of the findings in real-world, resource-limited settings. The reliance on published literature without individual patient data also limits the capacity to evaluate confounding variables or perform subgroup analyses.
4.4. Implications and future directions
The findings of this review represent important clinical and policy implications for managing CD in TB-endemic settings. Clinicians should implement a standardised, dual-modality LTBI screening protocol that combines IGRAs and TST before initiating biologic therapy. Prophylactic INH therapy remains essential but requires close liver function monitoring to mitigate hepatotoxic risks. Policymakers in high-burden regions should adapt national guidelines to reflect these evidence-based preventive strategies, emphasising individualised patient risk assessment and multidisciplinary coordination between gastroenterology and infectious disease specialists. Future research should focus on large-scale, prospective multicentre trials to validate the safety of anti-TNF therapy under these standardised preventive frameworks. Comparative studies evaluating newer biologic agents, such as vedolizumab and ustekinumab, are also needed to establish safer long-term alternatives for patients at high risk of TB reactivation. Ultimately, collaborative research efforts that integrate regional epidemiologic data will be pivotal in refining global treatment algorithms and advancing patient safety in endemic regions.
5. Conclusion
The evidence synthesised in this B-SLR indicates that adalimumab remains a cornerstone biologic for CD management, even in TB-endemic regions, provided that preventive measures are carefully implemented. Concurrent INH prophylaxis effectively reduces, though does not fully eliminate, the risk of TB reactivation during anti-TNF therapy. The safe and effective use of adalimumab in high-burden settings requires a region-specific clinical framework that (1) integrates multimodal LTBI screening combining clinical risk assessment, dual immunologic testing (IGRA + TST) as well as baseline imaging; (2) applies targeted prophylaxis and consistent hepatic monitoring; and (3) ensures sustained clinical vigilance and patient education throughout therapy. Ultimately, success depends on adaptive, locally contextualised strategies that balance therapeutic efficacy with infection risk mitigation. These findings reinforce the need for continued evidence generation in TB-endemic regions to support safer biologic use in complex inflammatory diseases.
Authors' Contributions
Nyimas Maida Shofa: Conceptualization, Methodology, Formal analysis, Writing – Original Draft, Writing – Review & Editing, Project administration. Nurike Setiyari Mudjari: Investigation, Data Curation, Resources, Writing – Review & Editing. Rusdiyana Ekawati: Methodology, Investigation, Data Curation, Writing – Review & Editing. Arianti Arianti: Investigation, Data Curation, Visualization, Writing – Review & Editing. Annisa Zahra Mufida: Resources, Validation, Supervision, Writing – Review & Editing. Budi Widodo: Formal analysis, Validation, Visualization, Writing – Review & Editing. Titong Sugihartono: Conceptualization, Supervision, Writing – Review & Editing.
Acknowledgement
The authors would like to thank all clinicians and researchers whose work contributed to the studies included in this review. We also acknowledge the valuable insights provided by colleagues during the manuscript preparation and revision process.
Data Availability
Data are available upon reasonable request from the corresponding author.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chen H Li P Chen J Wang Y Yu Q Wu Y Peripheral blood mononuclear cell micro RN As are novel biomarkers for diagnosing and monitoring Crohn's disease. FASEB J 2022; 36:e 22549. https://doi.org/10.1096/fj.202200452 r.10.1096/fj.202200452 R 36165177 · doi ↗ · pubmed ↗
- 2Park J Cheon JH. Incidence and prevalence of inflammatory bowel disease across Asia. Yonsei Med J 2021; 62:99–108. https://doi.org/10.3349/ymj.2021.62.2.99.10.3349/ymj.2021.62.2.9933527789 PMC 7859683 · doi ↗ · pubmed ↗
- 3Aniwan S Santiago P Loftus EV Jr.Park SH. The epidemiology of inflammatory bowel disease in Asia and Asian immigrants to Western countries. United European Gastroenterol J 2022; 10:1063–76. https://doi.org/10.1002/ueg 2.12350.10.1002/ueg 2.1235036479863 PMC 9752270 · doi ↗ · pubmed ↗
- 4Agrawal M Jess T. Implications of the changing epidemiology of inflammatory bowel disease in a changing world. United European Gastroenterol J 2022; 10:1113–20. https://doi.org/10.1002/ueg 2.12317.10.1002/ueg 2.1231736251359 PMC 9752308 · doi ↗ · pubmed ↗
- 5Heydari K Rahnavard M Ghahramani S Hoseini A Alizadeh-Navaei R Rafati S Global prevalence and incidence of inflammatory bowel disease: A systematic review and meta-analysis of population-based studies. Gastroenterol Hepatol Bed Bench 2025; 18:132–46. 10.22037/ghfbb.v 18i 2.3105.40936779 PMC 12421925 · doi ↗ · pubmed ↗
- 6Bonhomme B Nandi N Berera S Lee H Leung G Tse CS Greater fatigue and reduced neurocognitive speed with symptomatic Crohn's disease. Crohns Colitis 2024; 7:otae 069. https://doi.org/10.1093/crocol/otae 069.10.1093/crocol/otae 069PMC 1168408039742036 · doi ↗ · pubmed ↗
- 7Furfaro F Ragaini E Peyrin-Biroulet L Danese S. Novel therapies and approaches to inflammatory bowel disease (IBD). J Clin Med 2022; 11:4374. https://doi.org/10.3390/jcm 11154374.10.3390/jcm 1115437435955992 PMC 9369414 · doi ↗ · pubmed ↗
- 8Yang YJ Jeon SR. Metabolic musculoskeletal disorders in patients with inflammatory bowel disease. Korean J Intern Med 2025; 40:181–95. https://doi.org/10.3904/kjim.2024.359.10.3904/kjim.2024.35940102707 PMC 11938716 · doi ↗ · pubmed ↗