Thoracic Aorta Calcification and Risk of All-Cause Mortality and Cardiovascular Outcomes: A systematic review and meta-analysis
Yasir Salah Jumah Alam, Hussein Nafakhi, Alaa Salah Jumaah, Akeel Abed Yasseen, Zahraa Alaa Salah Alam, Ali Athir Abdulraheem

TL;DR
Thoracic aorta calcification is strongly linked to increased risks of death and cardiovascular issues, with computed tomography showing the strongest associations.
Contribution
This study provides a comprehensive meta-analysis showing TAC as a significant predictor of mortality and cardiovascular outcomes across imaging methods.
Findings
TAC is associated with a 61% higher risk of all-cause mortality.
Computed tomography shows the strongest link between TAC and cardiovascular mortality.
All aortic segments show elevated mortality risks, with descending aorta having a 41% higher risk.
Abstract
This review aimed to assess thoracic aorta calcification (TAC) as a predictor of all-cause mortality, cardiovascular (CV) morbidity and mortality across various clinical settings using different imaging modalities. Medical databases were systematically searched up to mid-July 2025 for studies linking TAC with mortality and CV outcomes. A total of 43 studies involving 176,738 participants were included. TAC was associated with higher risks of all-cause mortality (hazard ratio [HR] = 1.614), CV mortality (HR = 2.130), coronary events (HR = 1.423), major adverse cardiac events (HR = 2.011) and stroke (HR = 1.450. Computed tomography showed the strongest associations (all-cause mortality HR = 1.810; CV mortality HR = 2.641), followed by chest radiography and echocardiography. Mortality risk was elevated across all aortic segments, including descending aorta (HR = 1.414), aortic arch (HR =…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
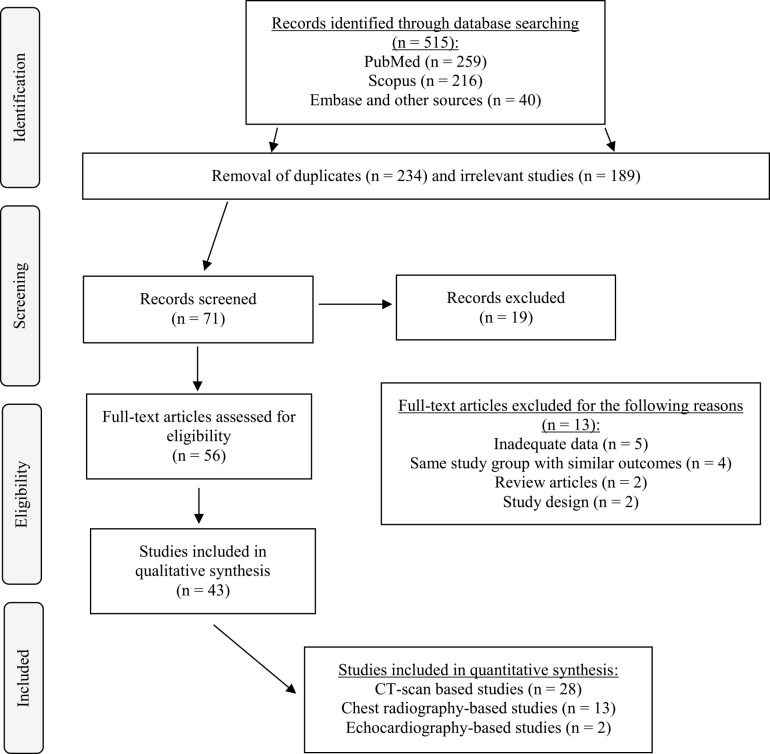 Fig. 1
Fig. 1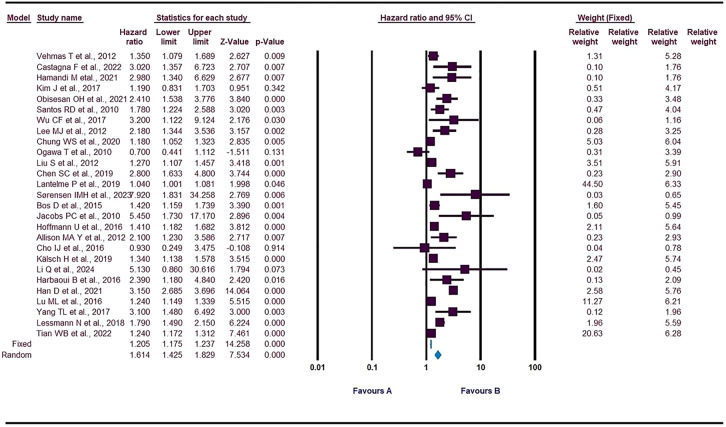 Fig. 2
Fig. 2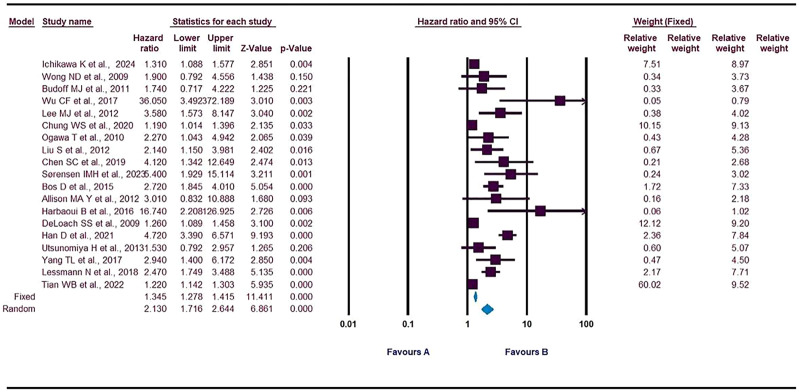 Fig. 3
Fig. 3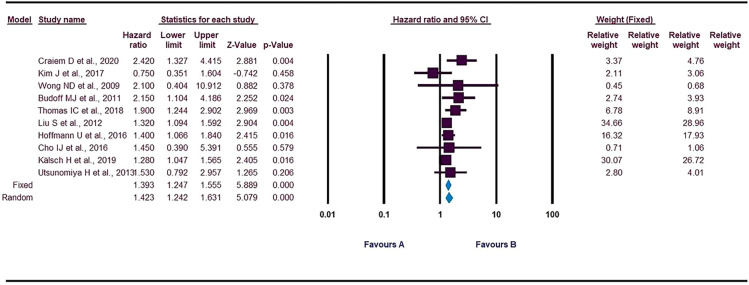 Fig. 4
Fig. 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAortic Thrombus and Embolism · Cardiac Valve Diseases and Treatments · Parathyroid Disorders and Treatments
1. Introduction
Vascular atherosclerosis is a chronic, progressive and systemic condition characterised by calcification, which can affect the entire arterial tree. This process begins when vascular smooth muscle cells transform into an osteoblastic phenotype, driven by oxidative stress and endothelial damage. Atherosclerosis is a leading cause of morbidity and mortality, contributing to 84.5% of cardiovascular (CV) deaths and 28.2% of all deaths.^12^ The progression of atherosclerotic calcification is closely linked to major CV risk factors, often beginning as early as adolescence, with lipid accumulation, inflammation and eventual vascular wall calcification occurring over time. However, the burden of calcification can vary widely across different arterial regions, which may directly impact its relationship with major adverse cardiac events (MACE).^12345^
Several imaging methods, including computed tomography (CT), echocardiography and plain X-rays, are used to measure vascular calcification.^6^ Cardiac CT is particularly useful as it allows for the detection of both coronary artery calcification (CAC) and thoracic aorta calcification (TAC), providing valuable information for risk stratification. Additionally, TAC can be measured on routine chest CT scans taken for various clinical reasons, without the need for extra radiation or electrocardiogram gating.^7^ This approach could enhance the identification of high-risk patients and, in turn, help prevent coronary events or reduce all-cause mortality.^89^ Emerging evidence also suggests that advanced CV magnetic resonance imaging may assess TAC, particularly in high-risk populations such as patients with end-stage renal disease.^6^
While CAC is well-established as a reliable predictor of coronary and CV events, TAC has not been studied as extensively, despite evidence suggesting that it is independently associated with increased morbidity and mortality, particularly for non-coronary conditions.^101112^ Calcification of the thoracic aorta, especially in the arch and descending segment, is considered a marker of coronary artery disease (CAD) and is strongly linked with coronary calcification, indicating a shared underlying systemic atherosclerotic process.^1314^ Several population-based studies have shown that the presence and extent of TAC correlate with higher rates of CV events.^15^
Despite these associations, neither the European Society of Cardiology nor the American College of Cardiology/American Heart Association's primary prevention guidelines include aortic calcification in their stepwise approach for preventing MACE in patients with atherosclerotic CV disease.^16^ The literature on TAC's role in long-term outcomes is inconsistent, with conflicting results from studies using the Multi-Ethnic Study of Atherosclerosis (MESA) database. This large, prospective cohort study of subclinical atherosclerosis includes participants from 4 ethnic groups who underwent baseline cardiac CT scans and were followed for incident CV and non-CV outcomes.^16^ Thomas et al., using MESA data, found that TAC is associated with an increased risk of incident CAD and non-CV disease-related adverse outcomes.^5^ In contrast, Budoff et al., in a study of 6,807 MESA participants, found that TAC independently predicted incident CAD only in women and provided no additional value if no CAC was present.^7^ Similarly, Han et al. reported that TAC is independently linked to CV mortality, suggesting that significant TAC may offer additional prognostic value beyond current guidelines.^15^ However, other studies using the MESA database failed to find a meaningful association between TAC and adverse CV morbidity or mortality.^1417^ Likewise, the Framingham Heart study did not observe a significant relationship between TAC and cardiac events, regardless of CAC status.^4^ The Heinz Nixdorf Recall trial and Early Identification of Subclinical Atherosclerosis by Noninvasive Imaging Research study also found no predictive value for TAC regarding cardiac events after adjusting for CAC.^81314^ These inconsistent findings from large-scale studies with diverse populations raise questions about the value of TAC as a predictive marker beyond CAC measurement. However, other studies have demonstrated TAC's ability to independently predict CV events and increased CV mortality in general populations, as well as in patients with end-stage renal disease or lung cancer.^3181920^
Given the conflicting results of previous studies, this review aimed to further investigate the predictive role of TAC as a marker for all-cause mortality, CV death and adverse coronary and CV events in different clinical settings, using various imaging techniques and in populations with diverse CV risk factors.
2. Methods
This systematic review and meta-analysis were conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [Supplementary File 1].^21^ The study protocol was not registered in any database.
2.1. Search strategy
A comprehensive electronic search was conducted across PubMed Central, Scopus and EMBASE databases until mid-July 2025. Searches were performed without language restrictions, but the analysis was restricted to studies published in the English language. The search terms used included “thoracic aorta calcification”, “aortic calcification”, “aortic root calcification”, “aorta calcification”, “arch of aorta calcification”, “ascending aorta calcification”, “descending aorta calcification” combined with “death”, “cardiovascular events”, “mortality”, “prognosis,” “survival”, “coronary”, “MACE.” as well as the imaging modalities “trans-thoracic echocardiography,” “trans-esophageal echocardiography”, “CT chest”, “magnetic resonance” and “chest X-ray”. Additionally, reference lists of relevant studies were manually searched to find other pertinent articles.
2.2. Inclusion/exclusion criteria
Two researchers (HN and ASJ) independently screened studies for eligibility, resolving disagreements with a third reviewer (YA). Included studies were original cohort or case-control designs assessing TAC—overall or by segment—and its association with CV events, mortality, coronary events, or stroke, reporting risk estimates for these outcomes. For cohorts with multiple publications, only the most comprehensive study was selected, while additional articles were included only if they reported entirely distinct outcomes or analysed non-overlapping subpopulations, ensuring statistical independence of all data.
Reviews, case reports, letters to the editor, editorials, comments, cross-sectional studies, conference papers, or articles without original data were excluded. Cross-sectional studies were excluded because they lack longitudinal follow-up and cannot provide hazard ratios or time-to-event estimates required for prognostic evaluation. Additional exclusions were preprints, animal studies and non-English publications.
2.3. Definitions
TAC was defined as the presence of calcified lesions in any thoracic aortic segment, including the ascending and descending aorta, and quantified either as present/absent or using study-specific severity categories. On chest CT, TAC was assessed by calcium scoring or by visual identification of calcified plaques, providing precise localisation and quantification. For chest radiography, TAC was assessed using standard anteroposterior chest radiographs in all included studies. The extent of calcification was typically categorised qualitatively (e.g., absent, mild, moderate, severe) or semi-quantitatively, with the most severe category used for statistical analysis. The presence of calcification was identified as linear or nodular radiopaque densities along the aortic contour, particularly in the ascending and descending segments. On the echocardiography-based studies, TAC was assessed using transthoracic echocardiography. Calcifications in the aortic root (ARC), aortic valve, mitral annulus and left ventricular myocardium were identified as echogenic areas and severity was classified qualitatively. For studies reported TAC using multiple severity categories (e.g., none, mild, moderate, severe), the risk estimate was extracted comparing the most severe TAC category versus no TAC.
The primary outcomes of interest were MACE, coronary events, CV death and all-cause mortality. Given the heterogeneity in endpoint definitions across studies, outcomes were harmonised into standardised categories. MACE was generally defined as a composite endpoint comprising CV death, myocardial infarction, heart failure and stroke, and in some studies also included coronary revascularisation. Coronary events encompassed fatal or non-fatal myocardial infarction, coronary revascularisation or death attributed to CAD. CV mortality referred to deaths resulting from fatal myocardial infarction, stroke, heart failure or other CV causes, while all-cause mortality represented death from any cause. When both fatal and non-fatal events were reported separately, the composite endpoint was used to maintain consistency across analyses.
2.4. Statistical analysis
A random-effects model was employed to calculate pooled hazard ratios (HR) and corresponding 95% confidence intervals (CI) for the association between TAC and adverse outcomes. This model accounts for variability across studies, including differences in study design, populations and methodologies. The analysis was performed using Comprehensive Meta-Analysis software (Version 3.0, 2013). To ensure comparability across studies, maximally adjusted HRs were prioritised whenever available. When adjusted HRs were not reported, unadjusted HRs were used. For studies that categorised TAC into multiple levels (e.g., none, mild, moderate, severe), the effect estimate was extracted and compared to the most severe category versus no calcification to achieve uniformity across datasets and to capture the prognostic impact of advanced TAC.
2.5. Heterogeneity assessment
Heterogeneity across studies was assessed using Cochran's Q test, the I statistic and the Tau statistic. The degree of heterogeneity was interpreted based on the I value, with 0–25% indicating low or no heterogeneity, 25–50% representing moderate heterogeneity, 50–75% denoting substantial heterogeneity and 75–100% reflecting considerable heterogeneity.
2.6. Publication bias assessment
Publication bias was evaluated using funnel plots and Egger's regression test. Publication bias occurs when studies with statistically significant results are more likely to be published compared to those with non-significant findings. Trim-and-fill test was used for analysis if there was less than 10 studies.^2223^
2.7. Study quality assessment
The methodological quality of the included cohort studies was assessed using the Newcastle-Ottawa Scale, which evaluates 3 essential domains: study group selection, cohort comparability and outcome assessment. Each study can receive up to 9 stars, with 4 for selection, 2 for comparability and 3 for result domains. Studies with 7–9 stars were regarded as good quality, 5–6 stars as moderate quality and less than 5 stars as low quality. This method enables a controlled and transparent assessment of observational study design and reporting quality. Based on the Newcastle–Ottawa Scale, the methodological quality of the included studies was generally high, with total scores ranging from 5–9. Over half of the studies (54%) were rated as high quality (≥7 points), while the remainder were of moderate quality (5–6 points); none were low quality. Overall, the evidence base supporting the prognostic role of TAC is robust and derived mainly from well-designed cohort studies [Supplementary Fig. 1].^24^
2.8. Subgroup and sensitivity analysis
Subgroup analyses were performed for each outcome based on detection methods (CT, echocardiography, chest X-ray) and population types (CAD, general population, end-stage renal disease and trans-aortic valve implantation). Segment-based subgroup analyses (root, ascending aorta, descending aorta, aortic arch) were pre-specified a priori, while modality-based and population-based subgroups were exploratory and performed post-hoc. Sensitivity analyses were also conducted based on sample size and the duration of follow-up. ^24^
3. Results
Out of the 515 potentially eligible publications, 43 studies, encompassing a total of 176,738 participants, met the inclusion criteria and provided data suitable for quantitative analysis [Fig. 1].^13457810111415171819202526272829303132333435363738394041424344454647484950515253^ Several included studies originated from the same parent cohorts. Specifically, 4 publications were derived from MESA study and 2 from Heinz Nixdorf Recall study.^578172632^ To avoid participant overlap, only 1 study per cohort was retained for each outcome, prioritising the most comprehensive or outcome-specific report. For instance, Ichikawa et al. was used for the main MESA analysis, while Kim et al. and Thomas et al. were included as non-overlapping subgroup analyses.^51726^ Similarly, Mahabadi et al. and Kalsch et al. were treated as distinct analyses due to their different methodological focus (baseline prediction versus progression).^832^ Across the 43 included studies, adverse outcomes were evaluated through predefined clinical or registry-based endpoints, including all-cause mortality (63%), CV mortality (44%), coronary events (23%), MACE (21%) and stroke (7%). MACE definitions generally encompassed CV death, myocardial infarction and revascularisation, though some variation existed across studies. The mean age of participants ranged from 49–83 years, with a substantial portion (48%) having a mean age between 55–65 years; 79% of participants had a mean age above 55 years. Follow-up assessments were primarily based on medical records, national death registries or longitudinal cohort databases. Populations including general cohorts (51%), end-stage renal disease (ESRD) patients (24%) and CAD (9%) or post–trans-aortic valve implantation (TAVI) (7%) populations. Of the included studies, 86% were published in 2011 or later, with 32% originating from the USA. The majority of the studies were prospective (53%). The weighted average percentage of male participants across all included studies was 55% (98,406 males out of 176,738 total participants). The assessment of adverse outcomes and the duration of follow-up varied considerably based on the imaging modality used to detect TAC. CT-based studies (65% of all included studies) typically provided the most comprehensive and long-term data, with follow-up durations ranging from 1.0–12.4 years, universally assessing endpoints like all-cause mortality, CV death, coronary events and stroke. In contrast, chest radiography-based studies (30% of studies) were characterised by a shorter follow-up range, spanning from a minimum of 0.1–5.7 years, often focusing on high-risk or acute clinical settings and prioritising endpoints such as MACE and all-cause mortality. The few studies relying on echocardiography reported medium-term follow-up between 2.9 and 3.8 years, focusing on a range of severe outcomes including all-cause death, CV death, MACE and stroke in specific high-risk clinical populations [Supplementary Table 1 and 2].
Flow chart showing the study selection process.
The pooled HRs, heterogeneity assessment using I-squared test and publication bias assessment using both Egger‘s regression and Trim and fill test for various outcomes in patients with TAC are as follows: all-cause death: 1.614 (95% CI: 1.425–1.829), CV death: 2.130 (95% CI: 1.716–2.644), coronary events: 1.423 (95% CI: 1.242–1.631), major adverse CV events (MACE): 2.011 (95% CI: 1.431–2.824) and stroke: 1.446 (95% CI: 1.054–1.983) [Fig. 2,Fig. 3,Fig. 4, Supplementary Table 3, Supplementary Fig. 2 and 3]. Publication bias tested using Egger‘s regression, Funnel plot and trim-and-fill test [Supplementary Table 3 and Supplementary Fig. 4].
Forest plot displaying thoracic aorta calcification as a predictor of all-cause death.
Forest plot displaying thoracic aorta calcification as a predictor of cardiovascular death.
Forest plot displaying thoracic aorta calcification as a predictor of coronary events.
3.1. Subgroup analysis
The subgroup analyses were based on detection methods, aortic segments used for assessment, the underlying population type and clinical indications for TAC.
In terms of detection methods, for all-cause death, the pooled HR using chest radiography was 1.522 (95% CI: 1.144–2.024), CT scan 1.810 (95% CI: 1.482–2.209) and echocardiography 1.240 (95% CI: 0.628–2.450) [Supplementary Fig. 5]. In the analysis of CV death, the pooled HR for chest radiography was 2.050 (95% CI: 1.421–2.956), CT scan was 2.641 (95% CI: 1.871–3.727) and echocardiography was 1.530 (95% CI: 0.554–4.229). For coronary events, the pooled HR for chest radiography was 1.320 (95% CI: 0.922–1.889), CT scan was 1.504 (95% CI: 1.224–1.848) and echocardiography was 1.530 (95% CI: 0.740–3.163) [Supplementary Table 4].
3.2. Aortic segments
For all-cause death, the pooled HR for calcification in the ARC was 1.240 (95% CI: 0.932–1.650), the arch of the aorta was 1.362 (95% CI: 1.200–1.545), ascending aorta was 1.350 (95% CI: 0.947–1.925) and descending aorta was 1.414 (95% CI: 1.025–1.950). The greatest risk was observed in descending aorta calcification, with a 41.4% risk increase [Supplementary Fig. 6]. In the analysis of CV death, the pooled HR for calcification in the ARC was 1.530 (95% CI: 0.603–3.884), the arch of the aorta was 2.056 (95% CI: 1.522–2.779) and descending aorta was 1.905 (95% CI: 0.942–3.850). The highest risk was seen in arch of aorta, showing a 2-fold increased risk, followed by descending aorta calcification, showing a 90.5% increased risk [Supplementary Fig. 7].
In terms of population type, for all-cause death, the pooled HR for CAD was 3.100 (95% CI: 1.240–7.747), ESRD was 1.561 (95% CI: 1.189–2.050), the general population was 1.644 (95% CI: 1.391–1.944) and TAVI was 1.521 (95% CI: 1.002–2.310).
For CV death, the pooled HR for CAD was 2.940 (95% CI: 1.400–6.172), ESRD was 1.389 (95% CI: 1.201–1.608), general population was 1.342 (95% CI: 1.266–1.423) and TAVI was 16.740 (95% CI: 2.208–126.925). For coronary events, the pooled HR for CAD was 2.420 (95% CI: 1.319–4.441), ESRD was 1.320 (95% CI: 1.075–1.621) and general population was 1.400 (95% CI: 1.208–1.623) [Supplementary Table 4].
3.3. Clinical indication for TAC
In several included studies, TAC was assessed as a secondary or incidental finding rather than the primary imaging indication. To evaluate whether this influenced the results, a subgroup analysis was conducted and stratified by clinical indication (lung cancer screening, CV risk assessment or health check, CAC scoring, TAVI evaluation, ESRD or dialysis screening and high-risk patient assessment).
In all-cause death, there is a generally consistent association TAC and all-cause mortality across different populations. The pooled HR were 1.8 (95% CI: 1.4–2.4; P <0.001) for CAC screening, 1.4 (95% CI: 1.0–2.0; P = 0.01) for ESRD screening, 1.6 (95% CI: 0.9–2.8; P = 0.07) for health check cohorts, 1.6 (95% CI: 1.1–2.4; P = 0.01) for high-risk population screening, 1.8 (95% CI: 1.1–2.8; P = 0.01) for lung cancer screening and 1.6 (95% CI: 0.9–1.9; P = 0.054) for TAVI populations [Supplementary Fig. 8].
Meanwhile, in CV death, the pooled HR were 2.5 (95% CI: 1.4–4.4; P = 0.001) for CAC screening, 2.0 (95% CI: 1.3–3.2; P = 0.001) for ESRD screening, 1.7 (95% CI: 0.8–3.5; P = 0.15) for health check cohorts, 2.1 (95% CI: 1.1–3.9; P = 0.01) for high-risk population screening and 2.4 (95% CI: 0.9–6.5; P = 0.07) for lung cancer screening. A single study in the TAVI subgroup reported a markedly elevated HR of 16.0 (95% CI: 1.8–154; P = 0.01), but with a wide confidence interval reflecting limited sample size [Supplementary Fig. 9].
While, in coronary events, in cohorts undergoing CAC screening, TAC was significantly associated with an increased risk of coronary events (random-effects HR = 1.5, 95% CI: 1.2–1.8; P <0.001). In contrast, the association was not statistically significant among patients with ESRD (HR = 1.3, 95% CI: 0.9–1.8; P = 0.12) or in high-risk populations (HR = 1.6, 95% CI: 0.8–3.1; P = 0.16) [Supplementary Fig. 5].
3.4. Sensitivity analysis
Sensitivity analyses were conducted based on sample size (less than 1,000 versus greater than 1,000 participants) and study duration [Supplementary Table 4]. No significant changes were observed in the HRs for both models.
4. Discussion
In this systematic review and meta-analysis, individuals with TAC, regardless of its severity, faced a significantly higher risk of all-cause death, CV death, coronary events, MACE and stroke. Notably, patients with CAD had a markedly higher risk of all-cause death, which was primarily attributed to a single study.^1^ On the other hand, the risk of all-cause mortality did not significantly differ across different populations. The strong association between TAC and adverse CV outcomes observed in the current analysis is consistent with the broader understanding of atherosclerosis as a systemic and progressive process. Historical and genetic studies, such as the Horus Study of ancient Egyptian mummies and the work by Elkilany et al. on nitric oxide synthase gene polymorphisms, have demonstrated that vascular and aortic calcification are long-standing biological markers of premature mortality and CV disease.^54^ These findings, although not included in the quantitative synthesis due to their non-prospective design, provide compelling contextual evidence that aortic calcification reflects chronic vascular injury and endothelial dysfunction processes deeply rooted in human pathophysiology across time and populations.^5455^
The imaging modalities utilised to assess TAC varied across the 43 included studies, depending on institutional guidelines, study objectives and patient populations. Each method offers different advantages depending on the patient's characteristics, symptoms or risk factors. However, CT scanning remains the gold standard for detecting vascular calcifications, including both CAC and TAC, as it provides superior spatial resolution and can detect minute levels of calcification compared to chest radiography and echocardiography.^1851^ Non-contrast CT remains the reference standard for detecting vascular calcification, including TAC, demonstrating sensitivity exceeding 90% and specificity approaching 100% when validated against histopathologic or high-resolution imaging reference standards.^5657^ However, the high cost and ionising radiation have limited the use of CT in large epidemiologic studies.^51^ Emerging volumetric cine-magnetic resonance techniques have also shown feasibility in detecting descending aortic calcification, although current evidence is preliminary and insufficient for quantitative synthesis.^6^
In contrast, chest radiography detects mainly moderate to severe calcifications over the aortic arch or descending aorta, with relatively low sensitivity and specificity compared to CT. Its diagnostic accuracy is limited by superimposed structures and the 2-dimensional nature of the projection.^5758^ Echocardiography, while useful for detecting ARC and proximal ascending aortic calcification, offers lower spatial resolution and limited visualisation of distal thoracic segments, with low specificity and specificity compared to CT.^57^
In the current review, CT was the most frequently employed modality, used in approximately two-thirds of the included studies (28 studies). CT-based TAC assessment was most commonly performed in cohorts undergoing CAC scoring, pre-TAVI evaluation, high-risk population screening or imaging for chronic kidney disease and lung cancer screening programmes. In these studies, TAC quantification was typically derived retrospectively from existing non-contrast chest CT scans, enabling precise volumetric or Agatston scoring of aortic calcium. Consequently, CT-based cohorts generally included middle-aged to elderly individuals with moderate to high CV risk, which may explain their higher HRs for mortality and CV outcomes.
Chest radiography was mainly used in population-based health screening, postoperative risk assessment, or initial hospital evaluation of patients with acute coronary syndrome, angina or ESRD. TAC identification relied on visual grading of calcified plaques in the aortic arch. These studies generally involved asymptomatic or community-based participants and the detection of TAC was often incidental, reflecting real-world screening practices with lower radiation exposure and cost but reduced sensitivity compared to CT. In contrast, echocardiography-based detection reflected localised calcification of the ARC or valve regions and was mainly applied in elderly or high-risk cardiac patients, serving as a complementary, radiation-free modality for assessing CV calcification burden. These differences in indication and clinical setting—CT for CV risk quantification or aortic imaging, chest radiography for screening and echocardiography for cardiac evaluation—likely contribute to the heterogeneity in predictive strength observed across modalities. The findings highlight that TAC's prognostic value depends not only on imaging resolution but also on the clinical context in which it is detected.^1851^
Beyond technique, TAC was reported to be a strong predictor of adverse outcomes across diverse clinical contexts. TAC consistently predicted all-cause and CV mortality, with the strongest associations observed in CAC screening, ESRD, high-risk and lung cancer screening cohorts. Its predictive value for coronary events was most robust in CAC screening populations, while associations were weaker or non-significant in ESRD and other high-risk groups. These findings highlight TAC as a readily obtainable imaging biomarker with important prognostic relevance across multiple clinical settings. critically, while multi-slice CT provides the most accurate quantification of TAC, it involves exposure to ionising radiation, limiting its role in population screening. Instead, TAC assessment is best leveraged opportunistically during clinically indicated scans, such as low-dose lung cancer screening or routine non-contrast CT for CAC scoring. Notably, the majority of studies (approximately 65%) included in this meta-analysis used non-gated, non-contrast CT scans to detect and quantify TAC.^1437^ These scans were often obtained as incidental findings during low-dose procedures such as lung cancer screening CT or during routine non-contrast CT scans performed for CAC scoring, as seen in several MESA studies.^205053^ This technique carries a substantially lower radiation dose compared with multi-slice CT used for primary diagnostic purposes, supporting the feasibility and safety of opportunistic TAC assessment in clinical practice.^142637^
Regarding the specific aortic segments, significant associations were found between TAC in different aortic segments and all-cause mortality. The descending aorta exhibited the highest HR (HR = 1.414) for all-cause death, followed by the aortic arch (HR = 1.36). The descending and arch segments of the thoracic aorta showed more frequent atherosclerotic calcification and had been identified as the primary regions influencing CV mortality and morbidity.^13^ Additionally, the predictive value of descending aorta calcification for future CV events has been highlighted in various studies, including a model proposed by Jairam et al., which demonstrated its strong discriminatory ability for risk assessment.^53^
Several limitations in this review must be acknowledged. First, inconsistent adjustments for confounders across studies may have slightly inflated the risk estimates. Second, the definition and quantification of TAC varied across studies, even among those using the same imaging techniques, which could contribute to heterogeneity. Nevertheless, sensitivity analyses employing random-effects models confirmed the robustness of the overall findings. Third, the included studies varied in their primary imaging indications and TAC was often assessed as an incidental or secondary finding. Although subgroup analysis was performed according to imaging indication, some residual heterogeneity in imaging purpose and methodology may persist. Fourth, limited data were available for certain outcomes, such as stroke or MACE, thereby restricting detailed subgroup analyses for these endpoints. Fifth, while several cohorts adjusted for CAC, others reported unadjusted or partially adjusted models, and the heterogeneity and incomplete reporting of covariates precluded a formal stratified or meta-regression analysis by CAC adjustment (yes/no). However, major CT-based cohorts that included CAC in multivariable models—such as MESA, Framingham and Heinz Nixdorf Recall—consistently showed that TAC remained independently predictive of mortality and CV outcomes, supporting its additive clinical utility beyond CAC. Finally, most included studies combined fatal and non-fatal CV events, consistent with standard practice in longitudinal outcome reporting. However, due to heterogeneity in endpoint definitions and incomplete reporting, competing risks were not uniformly accounted for, which may have introduced some variability into the effect estimates.
5. Conclusion
TAC, particularly in the descending aortic segment, is a significant predictor of all-cause and CV mortality, as well as coronary events, across diverse clinical settings. CT-based assessment of TAC provides valuable information for CV risk prediction and could be an essential tool for early identification of high-risk patients.
Authors' Contribution
Yasir Salah Jumah Alam: Data curation, Conceptualization, investigation. Hussein Nafakhi: Data curation, Writing- Original draft preparation, Validation. Alaa Salah Jumaah: Conceptualization, Software, Validation, Visualization. Akeel Abed Yasseen: Supervision, Writing- Reviewing and Editing. Zahraa Alaa Salah Alam: Visualization. Ali Athir Abdulraheem: Visualization.
Ethics Statement
The Ethical Committee for Clinical Studies approved this meta-analysis (MEC-95). As the study not involved data from previously published research, formal written consent from participants was not necessary. The Institutional Review Board granted a waiver for consent. The authors are committed to maintaining high ethical standards and ensuring the accuracy of the data presented.
Conflict of Interest
The authors declare no conflicts of interest.
Funding
No funding was received for this study.
Data Availability
Data is available upon reasonable request from the corresponding author.
Generative AI Declaration
ChatGPT (OpenAI) was used only for language editing and text refinement during the preparation of this manuscript. All scientific content, analyses, interpretations and conclusions were developed exclusively by the authors. The authors reviewed and revised all AI-assisted text and take full responsibility for the final manuscript.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Yang TL Huang CC Huang SS Chiu CC Leu HB Lin SJ. Aortic arch calcification associated with cardiovascular events and death among patients with acute coronary syndrome. Acta Cardiol Sin 2017; 33:241–9. 10.6515/acs 20160902 a.28559654 PMC 5445241 · doi ↗ · pubmed ↗
- 2Rodríguez-Palomares JF Evangelista Masip A. Aortic calcium score and vascular atherosclerosis in asymptomatic individuals: Beyond the coronary arteries. Rev Esp Cardiol (Engl Ed) 2016; 69:813–16. 10.1016/j.rec.2016.05.006.27422447 · doi ↗ · pubmed ↗
- 3Bos D Leening MJ Kavousi M Hofman A Franco O Hvan der Lugt A Comparison of atherosclerotic calcification in major vessel beds on the risk of all-cause and cause-specific mortality: The rotterdam study. Circ Cardiovasc Imaging 2015; 8:e 003843. https://doi.org/10.1161/CIRCIMAGING.115.003843.10.1161/CIRCIMAGING.115.00384326659376 · doi ↗ · pubmed ↗
- 4Hoffmann U Massaro JMD'Agostino RB Sr Kathiresan S Fox CSO'Donnell CJ. Cardiovascular event prediction and risk reclassification by coronary, aortic, and valvular calcification in the framingham heart study. J Am Heart Assoc 2016; 5:e 003144. https://doi.org/10.1161/JAHA.115.003144.10.1161/JAHA.115.00314426903006 PMC 4802453 · doi ↗ · pubmed ↗
- 5Thomas IC Thompson CA Yang M Allison MA Forbang NI Michos ED Thoracic aorta calcification and noncardiovascular disease-related mortality. Arterioscler Thromb Vasc Biol 2018; 38:1926–32. https://doi.org/10.1161/ATVBAHA.118.310850.10.1161/ATVBAHA.118.31085029954753 PMC 6202121 · doi ↗ · pubmed ↗
- 6Edy E Rankin AJ Lees JS Barrientos PH Woodward R Stoumpos S Cardiovascular magnetic resonance for the detection of descending thoracic aorta calcification in patients with end-stage renal disease. J Cardiovasc Magn Reson 2021; 23:85. https://doi.org/10.1186/s 12968-021-00769-6.10.1186/s 12968-021-00769-634162405 PMC 8223384 · doi ↗ · pubmed ↗
- 7Budoff MJ Nasir K Katz R Takasu J Carr JJ Wong ND Thoracic aortic calcification and coronary heart disease events: the multi-ethnic study of atherosclerosis (MESA). Atherosclerosis 2011; 215:196–202. https://doi.org/10.1016/j.atherosclerosis.2010.11.017.10.1016/j.atherosclerosis.2010.11.01721227418 PMC 4110678 · doi ↗ · pubmed ↗
- 8Kälsch H Mahabadi AA Moebus S Reinsch N Budde T Hoffmann B Association of progressive thoracic aortic calcification with future cardiovascular events and all-cause mortality: ability to improve risk prediction? Results of the Heinz Nixdorf Recall (HNR) study. Eur Heart J Cardiovasc Imaging 2019; 20:709–17. 10.1093/ehjci/jey 173.30508179 · doi ↗ · pubmed ↗