Hydralazine-induced antineutrophil cytoplasmic antibody vasculitis with significant dermatologic manifestations
Aanal Patel, Mahroo Tajalli, Amit Singal, Lisa Zhou, Cindy Wassef

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2 Figure 3
Figure 3 Figure 4
Figure 4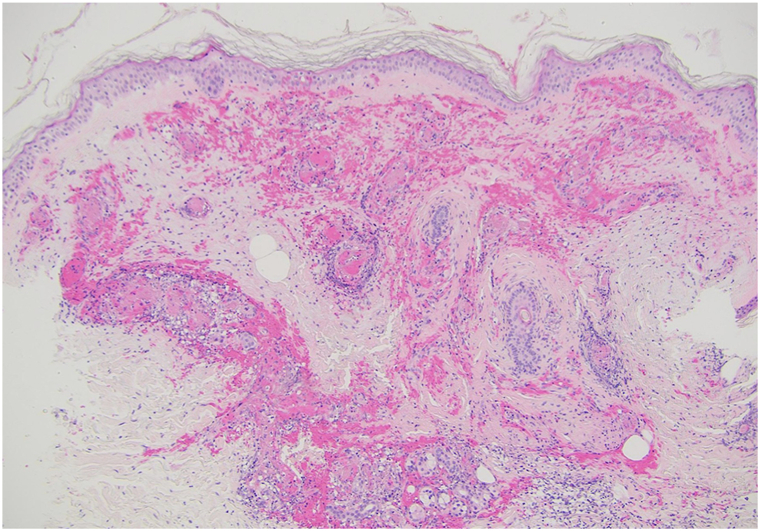 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVasculitis and related conditions · Drug-Induced Adverse Reactions · Otitis Media and Relapsing Polychondritis
Case description
Our department was consulted for a new purpuric rash in a 71-year-old woman with hypertension and heart failure with reduced ejection fraction. She had been hospitalized for angioedema of unclear etiology and subsequently developed low-grade fever, leukocytosis, and thrombocytopenia, followed by a rapidly progressive rash.
Examination revealed widespread purpuric plaques and hemorrhagic bullae affecting the eyelids, nasal tip, ears, and extremities (Fig 1, Fig 2, Fig 3 to 4). Oral examination showed erosions and hemorrhagic crusting of the palate; genital mucosa was spared.Fig 1. Hemorrhagic bullae over bilateral hands.Fig 2. Hemorrhagic bullae over left elbow.Fig 3. Hemorrhagic bullae over left ear.Fig 4. Purpuric papules, plaques and hemorrhagic bullae over lower extremities.
Laboratory studies showed elevated inflammatory markers, antinuclear antibodies 1:1280 (homogeneous), positive p-antineutrophil cytoplasmic antibody (ANCA) and c-ANCA, elevated myeloperoxidase (MPO)-ANCA (159 U) and proteinase 3-ANCA (1.1 U), and positive anti-histone antibodies. Rheumatoid factor, anticardiolipin IgM, lupus anticoagulant, and type III cryoglobulins were positive, with low C3 and undetectable C4. Anti-double-stranded DNA, anti-Smith, hepatitis B/C serologies, and protein electrophoresis were negative. Chest computed tomography revealed bilateral lower lobe atelectasis with moderate pleural effusion. A review of her home medications revealed chronic use of hydralazine 100 mg twice daily for 5-years for the management of hypertension and heart failure with reduced ejection fraction.
Skin biopsy demonstrated leukocytoclastic vasculitis with neutrophilic infiltration, vessel wall thrombosis, and extravasated erythrocytes; direct immunofluorescence supported immune-mediated vasculitis (Fig 5).Fig 5. Leukocytoclastic vasculitis, microthrombi in some vessel lumens, neutrophilic infiltrate in the dermis and upper part of the subcutis, and numerous extravasated erythrocytes.
Hydralazine was promptly discontinued. Given poor response to plasmapheresis, treatment was escalated to high-dose intravenous corticosteroids and rituximab, followed by a gradual steroid taper. Shortly after tapering, the patient developed melena secondary to gastrointestinal vasculitis. Despite IR embolization and intensified corticosteroid therapy, she experienced catastrophic gastrointestinal hemorrhage with disseminated intravascular coagulation and succumbed to fulminant systemic vasculitis.
Question: A patient on chronic hydralazine presents with purpura, oral ulcerations, and positive antinuclear antibodies and antihistone antibodies. Which condition is most important to distinguish from hydralazine-induced ANCA vasculitis?
- **A.**Systemic lupus erythematosus
- **B.**Stevens-Johnson syndrome
- **C.**Cryoglobulinemic vasculitis
- **D.**Bullous pemphigoid
- **E.**Drug reaction with eosinophilia and systemic symptoms
Answer: A. Systemic lupus erythematosus.
Discussion
Hydralazine, a selective arteriolar vasodilator used to treat hypertension, hypertensive emergencies in pregnancy, and heart failure with reduced ejection fraction, is generally safe and well tolerated.1 Rarely, it can induce hydralazine-induced ANCA-associated vasculitis—a potentially life-threatening autoimmune reaction.1 This condition involves inflammation and necrosis of small blood vessels, presenting with purpura, arthralgias, myalgias, fever, and multiorgan involvement.2
Hydralazine may trigger autoimmunity through several mechanisms. It may deplete neutrophilic histones at MPO and proteinase 3 loci, causing gene demethylation and antigen expression, or inhibit DNA methyltransferase, unmasking previously hidden antigens. It may also act as a hapten, binding MPO, and eliciting an immune response.1^,^3
Hydralazine-induced ANCA vasculitis presents variably, most often affecting the kidneys, lungs, and skin. Cutaneous manifestations such as palpable purpura and urticaria result from vascular inflammation and leakage. Severe cases may lead to mucosal ulcerations, limb ischemia, or fatal multiorgan failure.2, 3, 4 Our case demonstrated rare complications, including angioedema, pleural effusion, oral ulcerations, and gastrointestinal bleeding—features infrequently reported.1^,^3
Hydralazine-induced vasculitis can mimic systemic lupus erythematosus due to overlapping clinical and serologic features. Unlike systemic lupus erythematosus, it is typically characterized by positive ANCA and antihistone antibodies with negative anti-double-stranded DNA,3 making serologic testing essential for accurate diagnosis.
There is no standardized treatment; and management depends on severity. Prompt discontinuation of hydralazine is critical, with systemic corticosteroids or immunosuppressive therapy indicated for organ-threatening disease.5 This case underscores the importance of early recognition, vigilance for atypical presentations, and the development of standardized treatment strategies to improve outcomes.
Conflicts of interest
None disclosed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Siddiqui M.N.Norris S.A case of hydralazine-induced ANCA vasculitis/lupus overlap syndrome presenting as persistent bicytopenia Case Rep Rheumatol 20252025927659210.1155/crrh/9276592 PMC 1200303740242048 · doi ↗ · pubmed ↗
- 2Gandhi P.Khurana B.Munjal R.S.Sekar A.Gandhi R.G.Hydralazine-induced vasculitis Cureus 1522023 e 3530610.7759/cureus.35306 PMC 1004250236994251 · doi ↗ · pubmed ↗
- 3Yokogawa N.Vivino F.B.Hydralazine-induced autoimmune disease: comparison to idiopathic lupus and ANCA-positive vasculitis Mod Rheumatol 193200933834710.1007/s 10165-009-0168-y 19424772 · doi ↗ · pubmed ↗
- 4Levin L.E.Magro C.Horowitz J.Harp J.Hydralazine-associated cutaneous casculitis presenting with aerodigestive tract involvement Cutis 9952017 E 25E 2928632810 · pubmed ↗
- 5Weng C.H.Liu Z.C.Drug-induced anti-neutrophil cytoplasmic antibody-associated vasculitis Chin Med J (Engl)1322320192848285510.1097/CM 9.000000000000053931856057 PMC 6940077 · doi ↗ · pubmed ↗