Managing Acute Myocardial Infarction in Remote Oman: Real-world data from Al Wusta Governorate
Thuraiya Malik Abdullah Al Harthi, Ibrahim Al Mahrouqi, Amin Elbanna, Karema Hamed, Mohammed Abushilla, Venkatesh Kumar, Maryam Al Nabhani, Hasina Al Harthi, Abdulmunim Al Farsi, Adil Al Mahrouqi

TL;DR
This study examines STEMI management in a remote area of Oman, showing high success with thrombolysis but highlighting risks for patients with failed treatment.
Contribution
The study provides real-world insights into STEMI care in a resource-limited setting without advanced cardiac facilities.
Findings
Pharmacological thrombolysis had a 90.6% success rate in a remote Omani region.
Failed thrombolysis was strongly linked to alcohol consumption and anterolateral infarction.
A mortality rate over 20% was observed among patients with failed thrombolysis.
Abstract
Acute ST-segment elevation myocardial infarction (STEMI) is a time-sensitive cardiac emergency requiring prompt reperfusion therapy. Management and outcomes in remote areas are underexplored. This study explored the STEMI reperfusion network in Al Wusta governorate in Oman and evaluated the effectiveness of pharmacological thrombolysis in general practitioner (GP)-led, resource-limited hospitals. This retrospective study reviewed administrative health registries and medical records of patients presenting with STEMI to hospitals in the Al Wusta governorate between June 2017 and December 2024. Response to thrombolysis was defined as 50% resolution of ST-segment on electrocardiogram. Outcomes post-thrombolysis were prespecified. Multivariate logistic regression was used to identify predictors of thrombolysis failure. A total of 139 patients were included and received pharmacological…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
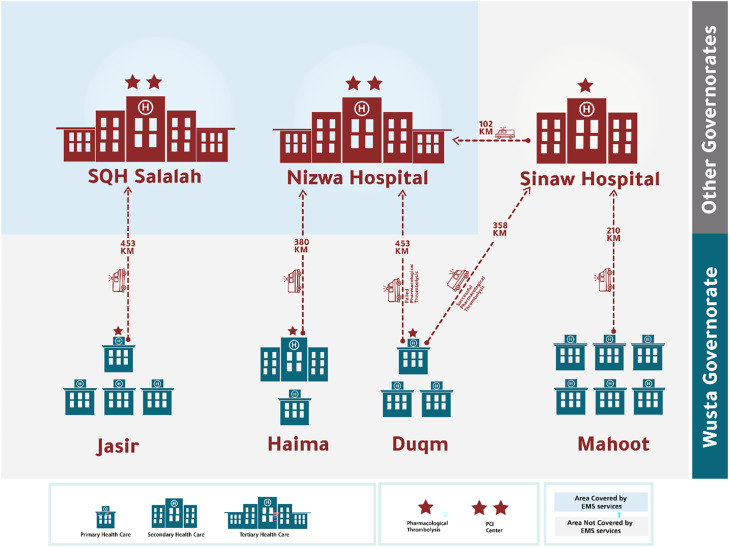 Fig. 1
Fig. 1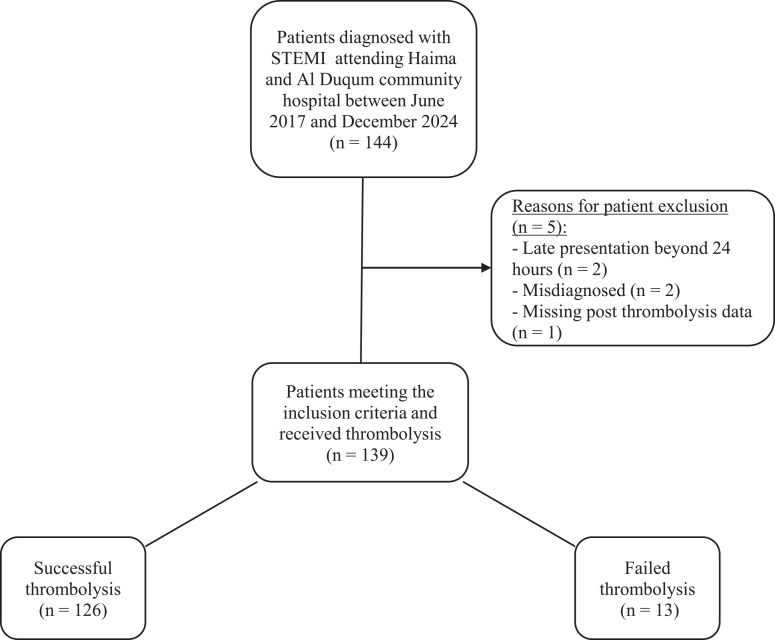 Fig. 2
Fig. 2| n (%) | ||||
|---|---|---|---|---|
|
| ||||
| Characteristic | Failed thrombolysis (n = 13) | Successful thrombolysis (n = 126) | Total (n = 139) | |
|
| 43.6 (6.1) | 48.2 (9.9) | 47.8 (9.8) | 0.95 |
|
| ||||
| Male | 12 (92.3) | 124 (98.4) | 136 (97.8) | 0.15 |
| Female | 1 (7.6) | 2 (1.6) | 3 (2.2) | |
|
| ||||
| Diabetes | 3 (23.1) | 54 (42.9) | 57 (41.0) | 0.17 |
| Hypertension | 4 (30.8) | 42 (33.3) | 46 (33.1) | 0.85 |
| Hyperlipidaemia | 3 (23.1) | 59 (46.8) | 62 (44.6) | 0.10 |
| Obesity | 1 (7.7) | 3 (2.4) | 4 (2.9) | 0.28 |
| IHD | 0 | 4 (3.2) | 4 (2.9) | 0.51 |
| Alcohol | 6 (46.2) | 7 (5.6) | 13 (9.4) | 0.00 |
| Smoking | 5 (38.5) | 49 (38.9) | 54 (38.9) | 0.98 |
| Family history of IHD or sudden death | 1 (7.7) | 4 (3.2) | 5 (3.6) | 0.41 |
|
| ||||
| Anterolateral | 4 (30.8) | 15 (11.9) | 19 (13.7) | 0.06 |
| Anteroinferior | 0 | 6 (4.8) | 6 (4.3) | 0.42 |
| Anteroseptal | 0 | 0 | 0 | - |
| Anteroposterior | 0 | 0 | 0 | - |
| Inferolateral | 1 (7.7) | 6 (4.8) | 7 (5.0) | 0.65 |
| Posteroinferior | 1 (7.7) | 6 (4.8) | 7 (5.0) | 0.65 |
| n (%) | ||||
|---|---|---|---|---|
|
| ||||
| Variable | Failed thrombolysis (n = 13) | Successful thrombolysis (n = 126) | Total (n = 139) | |
| Median time in minutes from symptoms to ER (IQR) | 280 (120–360) | 174 (60–300) | 180 (60–300) | 0.19 |
| Median time in minutes from door-to-needle (IQR) | 55 (30–60) | 42 (30–70) | 45 (30–70) | 0.44 |
| Median time in minutes from symptoms to thrombolysis (IQR) | 360 (180–420) | 212 (110–330) | 220 (115–375) | 0.11 |
| n (%) | ||||
|---|---|---|---|---|
|
| ||||
| Variable | Failed thrombolysis (n = 13) | Successful thrombolysis (n = 126) | Total (n = 139) | |
|
| 4 (30.8) | 4 (3.2) | 8 (5.8) | <0.01 |
|
| 4 (30.8) | 5 (4.0) | 9 (6.5) | <0.01 |
|
| 5 (38.5) | 13 (10.3) | 18 (12.9) | <0.01 |
|
| 2 (15.4) | 4 (3.2) | 6 (4.3) | 0.09 |
| Missing data | 0 | 8 (6.4) | 8 (5.7) | |
|
| 4 (30.8) | 7 (5.6) | 11 (7.9) | <0.01 |
|
| 9 (69.2) | 43 (34.1) | 52 (37.4) | <0.01 |
| Missing data | 0 | 7 (5.6) | 7 (5.0) | |
|
| 3 (23.1) | 0 | 3 (2.2) | <0.01 |
| Failed thrombolysis | OR (95% CI) | Standard error | t-value | |
|---|---|---|---|---|
| Alcohol consumption present | 28.9 (4.9–171.9) | 26.3 | 3.7 | <0.01 |
| Smoking status positive | 0.7 (0.2–2.8) | 0.5 | –0.5 | 0.6 |
| Hyperlipidaemia present | 0.1 (0.02–0.8) | 0.1 | –2.2 | 0.02 |
| 1.6 (0.6–3.8) | 0.7 | 0.9 | 0.3 | |
| Constant | 0.009 (0.0–1.3) | 0.02 | –1.8 | 0.06 |
| Mean dependent var | 0.094 | SD dependent var | 0.292 | |
| Pseudo r-squared | 0.256 | Number of obs | 139 | |
| Chi-square | 22.070 | Prob > chi2 | 0.000 | |
| Akaike crit. | 74.282 | Bayesian crit. | 88.955 | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAcute Myocardial Infarction Research · Cardiac Arrest and Resuscitation · Sepsis Diagnosis and Treatment
1. Introduction
Acute ST-segment elevation myocardial infarction (STEMI) is a time-sensitive cardiac emergency requiring prompt reperfusion therapy to restore coronary blood flow and reduce mortality.^1^ Primary percutaneous coronary intervention (PCI) is the gold standard for reperfusion;^2^ however, in geographically remote and resource-limited settings, timely access to PCI-capable centres is often not feasible.^3^ In such contexts, pharmacological thrombolysis remains the most accessible and practical initial reperfusion strategy, especially when administered promptly at the point of first medical contact.^4^
Although primary PCI is generally more effective than fibrinolytic therapy, its superiority diminishes when there are significant delays in performing the procedure.^56^ Evidence from randomised trials indicates that a PCI-related delay of 80 to 120 minutes omits the survival benefits of primary PCI compared to fibrinolysis.^78^ Similarly, data from the American National Registry of Myocardial Infarction registry suggest that when the delay for transfer to a PCI-capable facility approaches 120 minutes, the benefit of PCI over immediate on-site fibrinolysis is effectively lost.^9^
Oman's healthcare system faces unique challenges in ensuring equitable and timely STEMI care across its diverse regions. One such an area is Al Wusta Governorate which consists of 4 cities and is home to approximately 60,000 people.^10^ The region is geographically isolated, with distances ranging from 430 to 530 km to the nearest PCI-capable centres and lacks emergency medical services (EMS) making the management of acute STEMI particularly complex. As a result, thrombolysis is commonly administered in general practitioner (GP)-led, resource limited hospitals. Despite the efforts to reduce treatment delays, the delivery of thrombolysis requires effective coordination and reliable protocols to optimise outcomes.
While international evidence supports the feasibility of thrombolysis-based reperfusion networks in rural areas, limited data exist from the Middle East, and none to date have described or evaluated such networks in Oman.^11121314151617^ Understanding the structure, performance and clinical outcomes of STEMI care in remote settings is essential to inform national strategies and improve patient outcomes. Thus, this study aimed to describe the current reperfusion network for managing acute STEMI across healthcare levels in Al Wusta and evaluate the response and outcomes of pharmacological thrombolysis in patients presenting to resource limited hospitals in these settings.
2. Methods
This retrospective study analysed real-world data obtained from administrative health documents and the national electronic medical record system ‘Al Shifa’.^1819^ The study included 2 GP-led hospitals in Al Wusta Governorate— Haima Hospital and Al Duqm Hospital —both of which lack high-dependency units, intensive care units and specialised services such as cardiology. Al Wusta Governorate consists of 4 regions: Mahoot, Al Duqm, Haima and Al Jasir. In Mahoot, 6 primary care health centres (PCHCs) operate, none of which provide thrombolytic therapy. Al Duqm contains 3 PCHCs, with only 1 offering thrombolysis. Haima includes 1 PCHC and 1 secondary care centre that provides thrombolytic treatment. In Al Jasir, 4 PCHCs exist but thrombolysis is available at only 1 facility. The governorate lacks both EMS and PCI-capable hospitals. Consequently, patients requiring definitive care must be transferred via ambulance to central tertiary hospitals—located approximately 430 to 530 km away—for rescue PCI. To address this gap, the ‘drip and ship’ strategy has been implemented in 3 GP-led hospitals: Haima Hospital (since June 2017), Al Duqm Hospital (since February 2021), and most recently, Al Jasir (since January 2025), which started to operate after the study period. This approach involves initiating thrombolytic therapy onsite—specifically, 10 mg of reteplase administered in 3 doses 30 minutes apart before transferring patients for further evaluation and PC [Fig. 1].
Reperfusion management network for ST-segment elevation myocardial infarction within remote areas in Al Wusta Governorate in Oman.PCI = percutaneous coronary intervention; EMS = emergency medical services.
All adult patients (aged ≥18 years) who presented with a confirmed diagnosis of STEMI and received thrombolytic therapy between June 2017 and December 2024 were included. STEMI diagnosis was based on standard electrocardiographic (ECG) criteria and clinical presentation in accordance with international guidelines. Patients were excluded if they presented more than 24 hours after symptom onset, had no definitive STEMI diagnosis or had missing post-thrombolysis ECG data.
In the absence of contraindications, patients presenting with STEMI were evaluated through telephone consultation with a cardiologist from the nearest governorate. Upon confirmation of indication and safety, thrombolytic therapy is initiated. Patients were then transported by ambulance to a secondary or tertiary care facility, with an average transfer time of 4 to 5 hours. In cases of failed thrombolysis, patients were further referred to a PCI-capable centre for advanced management.
The primary outcome was the response to thrombolysis, which was classified as either successful or failed. A successful thrombolysis was defined as at least a 50% reduction in ST-segment elevation on ECG, along with clinical improvement in signs and symptoms, post-thrombolysis. Cardiac enzyme testing and imaging were not available in the study sites and therefore were not used for outcome evaluation. Post-thrombolysis outcomes were evaluated by identifying the occurrence of adverse events including cardiac-related deaths, cardiogenic shock, significant bleeding, the need for defibrillation or inotropic support and complications during ambulance transfer.
The secondary outcome was to identify predictors of failed thrombolysis. Prespecified variables included modifiable risk factors such as alcohol consumption, smoking, hyperlipidaemia diagnosis and time from symptoms to thrombolysis. This was measured using multivariable analysis.
This study adhered to the STROBE and RECORD guidelines for the reporting of observational research.^2021^ Descriptive statistics were used to summarise the data. Continuous variables were presented as mean ± standard deviation or median with interquartile range, depending on the distribution. Categorical variables were described using frequencies and percentages. Between-group comparisons were made using t-tests for continuous variables and Chi-square tests for categorical variables. Subgroup analyses were performed to explore potential confounding. Multivariable logistic regression was conducted to identify factors independently associated with failed thrombolysis. Data were entered using EpiData and analysed using STATA, (STATA Corporation, College Station, Texas, USA), Version 17.
3. Results
This study included a total 139 patients who received pharmacological thrombolysis of which 13 (9.4%) experienced failed treatment [Fig. 2]. In the sample, 97.8% were males and the mean age was 47.8±9.8 years. The majority of patients were Indian (n = 61, 43.9%) followed by Bangladeshis (n = 32, 23.0%) and Omanis (n = 25, 18.0%). A total of 13 patients (9.4%) consumed alcohol and 54 (38.9%) were smokers; More than a third of the study population had diabetes (41.0%) and hyperlipidaemia (44.6%) while few patients were obese (2.8%). Only 5 patients (3.6%) had a family history of ischaemic heart disease or sudden death. No significant correlation was found except for alcohol consumption (P <0.01) [Table 1].
Patient flow throughout study.STEMI = ST-segment elevation myocardial infarction.
Patients who experienced failed thrombolysis had longer delays at all measured time intervals compared to those with successful thrombolysis. The median time from symptom onset to emergency room arrival was 280 minutes in the failed group versus 174 minutes in the successful group, though this difference was not statistically significant (P = 0.19). Similarly, the door-to-needle time was slightly longer among those with failed thrombolysis (55 versus 42 minutes; P = 0.44). The total ischaemic time from symptom onset to thrombolysis was also higher in the failed group (360 versus 212 minutes; P = 0.11). While none of the differences reached statistical significance, the consistent trend suggests that treatment delays may contribute to thrombolysis failure [Table 2].
Patients with failed thrombolysis had significantly worse outcomes compared to those with successful reperfusion. Cardiogenic shock occurred in 30.8% of the failed group versus only 3.2% in the successful group (P <0.01) and use of a defibrillator post-thrombolysis was also more frequent in the failed group (30.8% versus 4.0%; P <0.01). The need for inotropes was significantly higher among failed cases (38.5% versus 10.3%; P <0.01) and adverse events during transport were more common (36.4% versus 5.6%; P = 0.01) compared to patients with successful reperfusion. Immediate mortality occurred only in the failed group (23.1% versus 0%; P <0.01), indicating a strong association between failed reperfusion and early death. Additionally, a higher proportion of patients with failed thrombolysis underwent rescue PCI or coronary artery bypass grafting (69.2% versus 34.1%; P <0.01) [Table 3].
After adjusting for modifiable risk factors, alcohol use was strongly associated with failed thrombolysis (odds ratio [OR] = 28.9, 95% confidence interval [CI]: 4.9–171.9; P <0.01), suggesting a potential behavioural influence on treatment response. In contrast, hyperlipidaemia showed a significant inverse association (OR = 0.1, 95% CI: 0.02–0.8; P = 0.02). Time from symptoms to thrombolysis had a large effect on thrombolysis failure, however evidence was not significant (OR = 1.6, 95% CI: 0.6–3.8; P = 0.3) [Table 4].
4. Discussion
To the best of the authors' knowledge, this study is the first to investigate the management of acute STEMI in remote areas of Oman, specifically within Al Wusta Governorate. The regional reperfusion network is steadily evolving, with thrombolytic therapy implemented in 3 GP-led, non-PCI-capable hospitals through a ‘drip and ship’ approach. Despite the absence of PCI centres and formal EMS, the network demonstrates a functional model of care adapted to the region's geographic and resource constraints. These gaps, however, highlight key opportunities for patient and system-level improvement, particularly in strengthening referral coordination, prehospital response and timely access to definitive care. Addressing geographic, infrastructural and cultural barriers could further enhance the delivery and outcomes of STEMI care in underserved areas.
In the current study 139 patients received pharmacological thrombolysis of whom 13 (9.4%) experienced failed treatment. Although time to reperfusion was longer in the failed group, the difference did not reach statistical significance—likely due to the small sample size—yet this remains clinically important. Nevertheless, clinical outcomes were significantly worse among those with failed thrombolysis, including higher rates of cardiogenic shock, inotrope use, defibrillation, transport complications and early mortality (P ≤0.01). Multivariable analysis identified alcohol use and anterolateral MI as significant predictors of thrombolysis failure, while hyperlipidaemia was inversely associated—highlighting the interplay between behavioural and clinical factors in influencing reperfusion outcomes.
International experiences provide valuable context for strengthening remote STEMI networks. For instance, the Minnesota STEMI system illustrates how structured, distance-based protocols can optimise care delivery across large geographic areas. Since 2003, hospitals up to 337 km from a central PCI centre in Minneapolis adopted a strategy where those within 96 km transferred patients for primary PCI, while more distant centres-initiated fibrinolysis followed by urgent transfer—a pharmaco-invasive approach. This model allowed patients to bypass emergency department reassessment and proceed directly to the catheterisation lab, achieving clinical outcomes comparable to those treated directly at PCI centres, despite longer transfer times.^22^ These findings affirm the potential of coordinated, protocol-driven care to ensure timely and effective reperfusion in remote settings.
Consistent with previous studies, patient-level delays in symptom recognition and failure to activate EMS remain key contributors to treatment delays in Al Wusta. Yin et al. highlighted similar barriers in rural China, including poor symptom awareness, limited EMS activation, inadequate training among non-hospital clinicians and weak interfacility communication.^23^ Likewise, Arnold et al.'s study found that most patients with STEMI presented directly to non-PCI centres rather than calling an ambulance, paralleling the situation in Al Wusta, where EMS support remains limited.^24^
The current study's findings on the rate and predictors of failed thrombolysis align with earlier reports. In a comparable study, failed thrombolysis occurred in 9.1% of patients and was strongly associated with increased mortality. Predictors of failure varied by thrombolytic agent: with tenecteplase, factors such as hypertension, prior stroke and elevated heart rate were significant; for streptokinase, Killip class ≥II and heart rate ≥100 bpm were key predictors. These patterns highlight the critical need for early risk stratification to guide treatment decisions, especially in non-PCI-capable facilities.^25^ The current study complements this evidence as it identified alcohol consumption and anterior MI location as additional predictors of thrombolysis failure.
The effect of alcohol consumption on the outcomes of pharmacological thrombolysis has been the subject of ongoing debate, with studies reporting conflicting findings.^26272829^ One study demonstrated that chronic alcohol consumption downregulates the expression of low-density lipoprotein receptor-related protein 1 in the liver, a key mediator of tissue plasminogen activator (tPA) clearance. As a result, tPA accumulates in the circulation and gains increased access to the brain parenchyma, where it may promote blood–brain barrier disruption and exert neurotoxic effects, ultimately leading to worse clinical outcomes following thrombolysis.^2627^ In contrast, other studies have failed to identify a clear detrimental effect of alcohol on thrombolysis outcomes. In fact, some findings suggested a slight benefit associated with alcohol consumption, although the results were statistically insignificant and lacked robust supporting evidence.^2829^ These inconsistencies may be attributed to variations in study design, population characteristics, duration and dose of alcohol exposure as well as differences in the underlying cardiovascular pathology.
Furthermore, the type of MI may play a role in thrombolysis outcomes. For instance, inferior MIs have been associated with more favourable responses to thrombolytic therapy compared to anterior wall MIs, a trend that was also observed in the current study. These observations highlight the need for more targeted clinical investigations to better understand the interplay between alcohol use, MI subtype and thrombolytic efficacy.^29^
In the current study, hyperlipidaemia was associated with improved thrombolysis outcomes, which may be explained by the use of statin therapy in these patients. Statins are known to exert pleiotropic effects beyond lipid lowering, including antithrombotic and pro-angiogenic properties. These effects may enhance vascular repair and improve reperfusion following thrombolytic treatment. Therefore, the observed benefit in patients with hyperlipidaemia is likely attributable to the pharmacological actions of anti-lipid therapy.^30^
In addition to geographic and infrastructural barriers, cultural and social norms play a significant role in delaying access to timely care for patients experiencing acute STEMI in remote regions. A substantial portion of the population in Al Wusta Governorate follows the Bedouin lifestyle, characterised by nomadic or semi-nomadic movement between desert areas and settlements. This transient way of living often places individuals at considerable distances from fixed healthcare facilities, making prompt recognition of symptoms and early presentation to medical services challenging. Furthermore, the absence of EMS in the region exacerbates the situation, as patients and their families must rely on self-transport over long distances, often without adequate knowledge of the urgency of cardiac symptoms. These factors contribute to significant delays in first medical contact, reduced eligibility for timely reperfusion, and ultimately suboptimal outcomes for STEMI patients in these underserved areas.
Future directions for improving STEMI care in remote regions of Oman should focus on strengthening both system- and patient-level responses. At the system level, implementing a pharmaco-invasive strategy, early thrombolysis followed by planned transfer for PCI within 3–24 hours along with regional EMS coverage and telemedicine-supported ECG consultation, could significantly reduce delays and improve outcomes. At the patient level, culturally tailored awareness campaigns targeting migrant workers and Bedouin communities may help shorten the time from symptom onset to hospital arrival. Future research should include a prospective registry of STEMI cases from remote areas, development of a risk stratification tool for failed thrombolysis and exploration of the potential protective effect of statins in reperfusion outcomes. Additionally, leveraging digital innovations such as artificial intelligence-assisted ECG interpretation, mobile applications for chest pain triage and low-cost telehealth platforms could further enhance access to timely diagnosis and treatment. The observed associations between alcohol use, infarct location and thrombolysis outcomes, as well as the potential beneficial role of statin therapy, warrant further investigation through larger, prospective studies to confirm these findings and explore their clinical implications.
The main limitation of the current study is the small subgroup of patients with failed thrombolysis, which reduces the reliability of regression analyses and results in unstable estimates (very wide CIs), thereby limiting confidence in predictors such as alcohol use. As a retrospective descriptive cohort study, it relied on routinely collected health data, which may be prone to incomplete or inaccurate documentation. Residual confounding, due to limitations in available data, may have influenced the identification of true predictors of failed thrombolysis. The classification of thrombolysis response was based on clinical and ECG criteria without confirmatory imaging or biochemical markers; while this may affect diagnostic accuracy, it reflects standard practice in rural hospitals and primary care settings where such resources may be limited. Despite these limitations, the study has several notable strengths. To the best of the authors' knowledge, this is the first real-world evaluation of a functioning STEMI reperfusion network in remote Oman. Unlike reports from central tertiary hospitals, the current study's findings reflect the realities of resource-limited practice, providing valuable insights for regions with similar geographic and infrastructural challenges. This study involved all healthcare institutions across the governorate, enhancing the generalisability of the findings within similar remote and resource-constrained settings. Beyond its clinical insights, this study offers practical evidence that can support the development of context-specific strategies to further strengthen STEMI care in Oman, particularly in regions that are geographically remote and resource-limited.
5. Conclusion
The reperfusion network in remote areas of Al Wusta Governorate continues to face geographical and social barriers that further impede optimal care for patients with acute STEMI. Despite the high rate of successful pharmacological reperfusion in GP-led hospitals, interventions at both patient and healthcare system levels are needed to reduce the incidence of delayed thrombolysis and its associated morbidity and mortality. The insights from this study can help guide practical improvements in STEMI care and shape policies that better serve remote communities.
Authors' contribution
Thuraiya Al Harthi: Conceptualization, Methodology, Formal analysis, Writing – Original draft, Writing – review and editing. Ibrahim Al Mahrouqi: Data curation, Validation, Writing – review and editing. Amin Elbanna: Data curation, Writing – review and editing. Karema Hamed: Data curation, Validation, Writing – review & editing. Mohammed Abushilla: Data curation, Validation, Writing – review & editing. Maryam Al Nabhani: Methodology, Validation, Writing – review and editing. Hasina Al Harthi: Writing – review and editing. Abdulmunim Al Farsi: Writing – review and editing. Adil Al Mahrouqi: Supervision, Conceptualization, Investigation, Data curation, Writing – review and editing.
Ethics statement
The study was approved by the Central Research and Ethics Committee at the Ministry of Health, Oman (MoH/ CSR/24/28450). As the study involved secondary analysis of routinely collected and anonymised data, informed consent was waived.
Generative AI declaration
ChatGPT was used to revise and improve the language and clarity of the written text in this manuscript.
Conflict of interest
The authors declare no conflicts of interest.
Funding
No funding was received for this study.
Data availability
Data are available upon reasonable request from the corresponding author.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Jacobs AK Ali MJ Best PJ Bieniarz MC Bufalino VJ French WJ Systems of care for ST-segment–elevation myocardial infarction: a policy statement from the American Heart Association. Circulation 2021; 144:e 310–27. https://doi.org/10.1161/CIR.0000000000001025.10.1161/CIR.000000000000102534641735 · doi ↗ · pubmed ↗
- 2Bagai A Dangas GD Stone GW Granger CB. Reperfusion strategies in acute coronary syndromes. Circ Res 2014; 114:1918–28. https://doi.org/10.1161/CIRCRESAHA.114.302744.10.1161/CIRCRESAHA.114.30274424902975 · doi ↗ · pubmed ↗
- 3Wang M Wu P Ma J Ma X Yang N Jia S Enhanced prognosis and regional cooperative rescue systems for acute myocardial infarction: insights from chest pain centers in Ningxia, China. Intern Emerg Med 2025; 20:1411–24. https://doi.org/10.1007/s 11739-025-03962-y.10.1007/s 11739-025-03962-y 40392480 PMC 12331797 · doi ↗ · pubmed ↗
- 4Gershlick AH Banning AP Myat A Verheugt FW Gersh BJ. Reperfusion therapy for STEMI: is there still a role for thrombolysis in the era of primary percutaneous coronary intervention? Lancet 2013; 382:624–32. https://doi.org/10.1016/S 0140-6736(13)61454-3.10.1016/S 0140-6736(13)61454-323953386 · doi ↗ · pubmed ↗
- 5De Luca G Suryapranata H Ottervanger JP Antman EM. Time delay to treatment and mortality in primary angioplasty for acute myocardial infarction: every minute of delay counts. Circulation 2004; 109:1223–5. https://doi.org/10.1161/01.CIR.0000121424.76486.20.10.1161/01.CIR.0000121424.76486.2015007008 · doi ↗ · pubmed ↗
- 6Terkelsen CJ Sorensen JT Maeng M Jensen LO Tilsted HH Trautner S System delay and mortality among patients with STEMI treated with primary percutaneous coronary intervention. JAMA 2010; 304:763–71. https://doi.org/10.1001/jama.2010.1139.10.1001/jama.2010.113920716739 · doi ↗ · pubmed ↗
- 7Nallamothu BK Bates ER. Percutaneous coronary intervention versus fibrinolytic therapy in acute myocardial infarction: is timing (almost) everything? Am J Cardiol 2003; 92:824–6. https://doi.org/10.1016/s 0002-9149(03)00891-9.10.1016/S 0002-9149(03)00891-914516884 · doi ↗ · pubmed ↗
- 8Betriu A Masotti M. Comparison of mortality rates in acute myocardial infarction treated by percutaneous coronary intervention versus fibrinolysis. Am J Cardiol 2005; 95:100–1. https://doi.org/10.1016/j.amjcard.2004.08.069.10.1016/j.amjcard.2004.08.06915619401 · doi ↗ · pubmed ↗