Paying the Price for Beauty Abroad: Khoula Hospital's experience with complications following aesthetic procedures performed overseas, 2013–2023
Khalifa Al Alawi, Areej Al-Mamari, Maysa Al-Maawali, Ashima Alkabi, Al-Batul Al-Mufargi, Juhaina Al Tobi, Hoor Al-Khanjari, Yasmine Al Balushi, Rawan Al Mandhari, Rafal Aljadder, Sultan Al Shaqsi

TL;DR
The study examines complications from overseas aesthetic surgeries treated at Khoula Hospital in Oman, highlighting risks like infections and the need for better regulation.
Contribution
The study provides new insights into the complications and outcomes of aesthetic tourism in Oman, emphasizing public health and regulatory implications.
Findings
Abdominoplasty was the most common overseas procedure, with wound infections being the leading complication.
Iran was the most frequent destination for these procedures, and nearly half of admitted patients required surgical intervention.
The findings suggest a hidden burden on local healthcare systems due to complications from aesthetic tourism.
Abstract
This study aimed to evaluate the types and outcomes of complications arising from aesthetic surgeries performed abroad and subsequently managed at Khoula Hospital, Muscat, Oman. This retrospective study included patients who presented with post-aesthetic surgical complications after undergoing procedures outside Oman from January 2013 to December 2023. Data were extracted from Khoula Hospital's electronic health records, focusing on demographics, procedures performed, types of complications and outcomes, including admissions and surgical interventions. A total of 191 patients with 488 recorded encounters were included. The most common procedures done overseas were abdominoplasty (50.8%), lipectomy (29.3%) and breast surgeries (17.8%); Iran was the most frequent destination (60.7%). The predominant complications included wound infections with gapping (36.1%), seromas (20.4%),…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
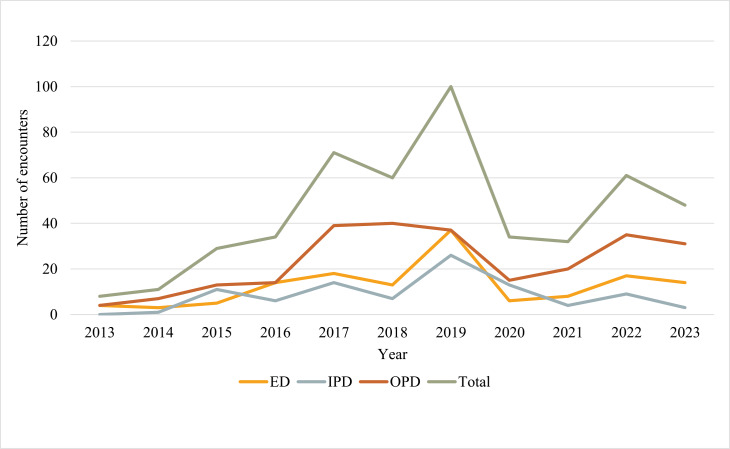 Fig. 1
Fig. 1| Characteristic | n (%) |
|---|---|
|
| 191 |
|
| 488 |
|
| |
| Female | 139 (72.8) |
| Male | 52 (27.2) |
|
| 40.2 |
|
| |
| None | 143 (74.9) |
| DM | 20 (10.5) |
| HTN | 17 (8.9) |
| Hypothyroidism | 13 (6.8) |
| Obesity | 6 (3.1) |
|
| |
| No surgical history | 67 (35.1) |
| Weight loss surgery | 17 (8.9) |
| Aesthetic procedure | 16 (8.4) |
| Other non-aesthetic procedure | 91 (47.6) |
| Characteristic | n (%) |
|---|---|
|
| |
| 1 procedure | 131 (68.6) |
| 2 procedures | 30 (15.7) |
| 3 procedures | 16 (8.4) |
| More than 3 procedures | 4 (2.1) |
|
| |
| Abdominoplasty | 97 (50.8) |
| Liposuction | 56 (29.3) |
| Breast surgery | 34 (17.8) |
| Other body contouring | 23 (12) |
| Rhinoplasty | 25 (13.1) |
| Blepharoplasty | 5 (2.6) |
| Facelift | 5 (2.6) |
| Injectables | 6 (3.1) |
| Hair transplant | 3 (1.6) |
| Scar surgery | 5 (2.6) |
|
|
|
| Country | n (%) |
|---|---|
| Iran | 116 (60.7) |
| India | 29 (15.2) |
| Thailand | 13 (6.8) |
| GCC | 10 (5.2) |
| Egypt | 12 (6.3) |
| Others | 11 (5.8) |
| Postoperative complication | n (%) |
|---|---|
| Wound infection with gapping | 69 (36.1) |
| Seroma | 39 (20.4) |
| Abscess formation | 11 (5.8) |
| Cellulitis | 21 (11.0) |
| Haematoma | 5 (2.6) |
| Major scar complication | 21 (11.0) |
| Major deformity post-rhinoplasty | 11 (5.8) |
| Sepsis | 1 (0.5) |
| Necrotising fasciitis | 1 (0.5) |
| Infected implant | 1 (0.5) |
| Epistaxis | 3 (1.6) |
| Post liposuction burn | 1 (0.5) |
| Facial palsy | 1 (0.5) |
| Capsular contracture/mismatch | 2 (1.0) |
| Lymphoedema post-brachioplasty | 1 (0.5) |
| DVT | 1 (0.5) |
| Severe post operative pain | 5 (2.6) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGlobal Healthcare and Medical Tourism · Body Image and Dysmorphia Studies · Body Contouring and Surgery
1. Introduction
Over the last few decades, there has been an increase in the demand for aesthetic surgeries worldwide.^1^ According to the American Society for Aesthetic Plastic Surgery's National Data Bank statistics, aesthetic surgical procedures increased by 54% in 2021, and are expected to grow to 3,847,929 by 2030, with an average annual growth of 7.1%.^23^ The most frequently performed procedures are lipectomy, followed by breast augmentation surgeries, abdominoplasties, facial surgeries and injectable filling materials.^45^ This trend may be influenced by social media, which has become a crucial tool in plastic surgery, for both patients' education and advertising.
Aesthetic procedures are often costly and are typically self-funded and not covered by the government or health insurance companies. The average costs of aesthetic surgical procedures reported in the literature were found to range from USD 11,900 for rhytidoplasty. The average costs of common procedures were 6,700 for breast reduction, 6,000 for lipectomy and $6,100 for rhinoplasty.^6^
The advantages of successful aesthetic procedures are substantial, yet complications are inevitable; most patients who return home seek for care in public hospitals.^47^ Commonly reported postoperative complications include infections, haematoma formation, wound complications, pain and aesthetic dissatisfaction.^589^ Whereas immediate postoperative complications might be directly addressed by the surgeon in-charge, late complications might be devastating, especially for patients who sought surgical treatment abroad and have no direct access to the treating surgeon.^8^
The healthcare system in Oman was established in 1970 and is publicly funded, with all Omani citizens receiving medical services free of charge. While the Ministry of Health serves as the primary healthcare provider, other governmental entities operate their own tertiary institutions, including the Royal Court Medical Services, the Armed Forces Hospital and the Royal Oman Police Hospital. Healthcare delivery is organised into primary, secondary and tertiary levels, with patients triaged according to the complexity of their medical conditions. In addition, specialised care is provided through dedicated institutions such as cancer, endocrine and gynaecology centres. The government also maintains a sponsored overseas treatment programme for selected complex cases; however, reliance on overseas care has declined substantially with the expansion of national healthcare services. Overseas treatment referrals decreased from 59 per 100,000 population in 1977 to 20 per 100,000 in 2010, with patients historically referred to countries such as India, Germany and the United Kingdom.^10^
In Oman, aesthetic procedures represent a growing trend. Additionally, many patients seek these procedures abroad, largely driven by lower costs and attractive treatment packages offered overseas. Consequently, despite the increasing local demand for aesthetic surgery, a substantial number of Omani patients continue to travel abroad to undergo aesthetic procedures. This practice has led to a rising number of patients presenting with postoperative complications, requiring evaluation and management within the public healthcare system. As a result, the management of complications following aesthetic procedures performed overseas constitutes an increasing burden on national health services, particularly at tertiary care centres.
In the local context, complications arising from aesthetic procedures performed within Oman are typically managed by the primary operating surgeon in the private sector. Referral to a public tertiary care centre is reserved for cases involving life-threatening complications or those exceeding the management capacity of private facilities, at which point patients are admitted to Khoula Hospital in the capital city Muscat. All complications resulting from aesthetic procedures performed overseas are managed within the public healthcare system.
To date, no published studies have evaluated the impact of managing complications from overseas aesthetic surgery within Oman. Therefore, this retrospective study aimed to investigate complications arising from aesthetic procedures performed outside Oman and subsequently treated at Khoula Hospital, with analysis of the types of complications encountered and the treatments required.
2. Methods
This retrospective study included patients who underwent aesthetic procedures abroad and subsequently presented to Khoula Hospital with complications between January 2013 and December 2023. For the purposes of this study, a patient was defined as an individual seeking medical care, whereas an encounter was defined as any healthcare interaction, including emergency visit, inpatient admissions and outpatient visits. All aesthetic surgical and non-surgical procedures were included. Cases with complications not related to aesthetic procedures were excluded. Data was extracted from Khoula Hospital's electronic database, Al Shifa 3 Plus, using search terms related to aesthetic procedures (such as abdominoplasty, brachioplasty, fillers, rhinoplasty, facelift, etc.) and common aesthetic surgery destinations (abroad, overseas, Iran, Turkey, Egypt, etc.). Two independent research assistants reviewed the initial patient list to exclude non-relevant cases.
The medical records of patients meeting the inclusion criteria were reviewed to extract relevant variables, which were recorded in a prepopulated Excel sheet (Microsoft Corp., Redmond, Washington, USA). All data were anonymised and coded for analysis. Variables with missing data were assessed on a case-by-case basis. Records with missing key outcome variables were excluded from the relevant analyses, while available data were retained for analyses in which missing values did not affect the outcome of interest. No imputation methods were applied due to the retrospective nature of the study. Descriptive statistics (percentages, means and standard deviations) summarised the study population.
3. Results
A total of 191 patients had a total of 488 encounters at Khoula Hospital due to post-aesthetic complications from procedures conducted overseas. Most of the study cohort were females (n = 139, 72.8%). The average age of the patients was 40 years (range: 17–72). Most patients (74.9%) had no comorbidities, while 25.1% had comorbidities such as diabetes mellitus (10.5%), hypertension (8.9%), hypothyroidism (6.8%) and obesity (3.1%). Additionally, 35.1% of patients had no previous surgical history, while 8.4% had undergone previous aesthetic procedures, 8.9% had bariatric surgery and 47.6% had other procedures such as appendectomy, C-section and herniorrhaphy [Table 1].
Among the 191 patients, 259 aesthetic procedures were done and most of the cohort underwent a single aesthetic procedure (68.6%), while 15.7% had two procedures performed in the same setting and 8.4% underwent three procedures. Of these, 50.8% had abdominoplasty, 29.3% had lipectomy and 17.8% underwent breast surgery [Table 2]. The most popular destinations for aesthetic surgery tourism were Iran (60.7%), followed by India (15.2%) and Thailand (6.8%) [Table 3].
The 191 patients had a total of 488 encounters at Khoula Hospital. Emergency visits accounted for 28.0% of all visits, admissions for 19.0% and outpatient visits for 52.0%. Emergency visits that resulted in admission were counted as admission episodes only, while any follow-up visits for admitted patients were included in the outpatient category. Regarding the timing of presentations, 39.0% of patients presented to Khoula Hospital within two weeks of their surgery, 29.0% presented between the second and fourth week postoperatively and 32.0% presented after the fourth week postoperatively. The number of encounters at Khoula Hospital due to post- aesthetic complications from overseas procedures increased significantly from 2013 to 2019, peaked, then dropped sharply in 2020 before partially increasing in 2021–2023 [Fig. 1].
Encounters at Khoula Hospital due to post-aesthetic complications from procedures conducted overseas from 2013–2023. ED = emergency department; IPD = inpatient department; OPD = outpatient department.
In terms of intraoperative and immediate postoperative complications (<3 days), 3 patients experienced major intraoperative complications and a further 3 patients experienced major postoperative complications. The first patient who had intraoperative complications was a female who underwent abdominoplasty in Egypt and suffered massive blood loss, leading to perioperative heart arrest, renal failure, prolonged intensive care unit admission and later, a wound gap. The second patient was also a female who underwent a dimple creation procedure, which was complicated by a buccal region haematoma. The third patient was a female who underwent rhinoplasty and experienced an undocumented major anaesthesia-related complication, requiring prolonged intensive care unit admission and tracheostomy, followed by the development of a tracheocutaneous fistula and subglottic constriction. Of the 3 patients who experienced severe postoperative complications with devastating outcomes, one developed complete facial palsy following a rhytidoplasty, another suffered from sepsis after abdominoplasty, leading to 20-day hospital stay, and the third developed necrotising fasciitis post-abdominoplasty. Additionally, many postoperative complications included wound infection with gapping (36.1%), seroma (20.4%), abscess formation (5.8%), cellulitis (11.0%), major scar complications such as contracture (11.0%) and haematoma (2.6%). Furthermore, 5.8% of patients developed significant post-rhinoplasty complications, including saddle nose deformity and nasal obstruction due to a deviated septum [Table 4].
A total of 94 patients were admitted due to complications following aesthetic surgery. The average length of stay was 10 days, with the longest stay lasting 40 days and the shortest lasting 1 day. All patients required intravenous anti-bacterial agents and regular wound dressings. Among them, 41 (43.6%) patients underwent a total of 108 surgical procedures. Of these, 18 required multiple procedures, with the highest number of visits to the operating theatre being 9. Additionally, 15 patients underwent reconstructive surgery, such as skin grafting or flap procedures. Overall, 18.0% of admitted patients required a blood transfusion and 20.0% required admission to a critical care unit or to a high dependency bed. Following discharge from their initial admission, 37.0% of patient required readmission for further management.
4. Discussion
This study aimed to evaluate the complications that occurred to patients who underwent aesthetic surgeries abroad. These complications ranged from simple complications such as wound infection and dehiscence to more serious outcomes leading to admission to the intensive care unit and prolonged hospital stays. The study included different cohorts of patients presenting to Khoula Hospital with diverse backgrounds.
Most patients in the present study (n = 116, 60.7%) travelled to Iran to undergo their aesthetic procedures. Patients favoured developing countries as their destination. During the period between 1967–1977, Iran was the top tourist destination for people from the Middle East. Since then, receiving treatment during a trip abroad has become quite popular, especially among families from Gulf countries. Shiraz and Mashhad were found to be the top two Iranian cities to provide such medical treatment. In one narrative review article, opportunities in Iran's medical tourism were summarised as push and pull factors.^11^ Examples of pull factors offered in Iran and relevant to the Omani tourist include the cultural similarities, religious affinity, low-cost and the geographical vicinity. Similarly, push factors in nearby countries involved the relatively high costs of private treatment, lack of advanced health facilities and low-quality health system.^11^ India, on the other hand, is also considered one of the largest providers of medical tourism services in the world. Another study was conducted in Al Dakhiliyah region of Oman, surveying the pattern of medical tourism among 40 patients.^10^ Surprisingly enough, the majority travelled upon the advice of a friend and only a few used medical tourism offices or the internet; most of the survey participants went to Thailand.^10^
Despite the variety of medical tourism categories, seeking medical care abroad, in general, has many shared socioeconomic advantages. For instance, the affordability of medical services in comparison to the relatively high costs in the private sector, avoidance of long waiting lists for elective procedures, better access to banned procedures in the public sector, combination of treatment and leisure as well as the availability of advanced and well-trusted healthcare systems. Other driving factors can extend to involve cultural reasons, family pressures and the travellers' perceptual beliefs related to the local healthcare services.^12^ Meanwhile, aesthetic procedures done aboard have some risks such as medical protocols mismatching those in the home country, thus thereby exposing patients to unknown risks, absence of pre-surgical assessment, inadequate post-operative care, lack of follow-ups, communication barriers, limited malpractice legislations and capacity to complain, restricted health insurance and the psychological distress of being far from home. These risks can affect the course of treatment and its quality.
Medical tourism obstacles are not limited to the patients but extend beyond that to indirectly impact the home country's healthcare system. The more a source country sends its citizens abroad for treatment, the less the tendency of the source country to develop a particular healthcare service which can be found elsewhere.^12^ For example, the very first positron emission tomography/computed tomography scan was performed in Muscat in 2015.^13^ In addition, financially covered medical tourism can also drain a home country of its will and obligations to improve essential healthcare services.^12^
With the currently enhanced pace of medical tourism and aesthetic surgeries being among the most performed procedures abroad, it is only foreseeable that more patients will be victims of post-operative complications. The most common procedures that presented with complications in the present study are abdominoplasty, lipectomy and breast surgeries. This group of aesthetic surgeries are not dissimilar to the most common destination procedures at a global level. Those consist of abdominoplasty, breast and gluteal augmentation and lipectomy.^14^ It is worth noting that from the previously studied population, the highest frequency of their post-operative presentation with complications to Khoula hospital was after 2 weeks followed by 4 weeks. The most frequent complications reported in emergencies were wound infection with gapping (36.0%), seroma (20.4%), cellulitis (11.0%), abscess formation (5.8%) and haematoma (2.6%). Other literature has demonstrated similar outcomes with predominant complications being infections followed by wound dehiscence and seroma or haematoma.^15^ Although the leading cause of morbidity and mortality following aesthetic surgeries is thromboembolism.
In the present study, all 94 patients were admitted and required intravenous anti-bacterial agents with regular wound dressings, suggesting that wound infection was a major indication for hospital admission. However, types of infection and anti-bacterial agent choices were not included, which represents an important limitation. This aspect is crucial in approaching patients with a history of operation done abroad as it carries difficulties in targeting atypical organisms. A systematic review done by Padilla et al. reported a high incidence of rapidly growing mycobacterial infections in patients who underwent plastic surgery abroad.^16^ In such a scenario, physicians should maintain a high suspicion dealing with such cases.^1617^ It is important to emphasise that there are no official guidelines for the perioperative use of prophylactic anti-bacterial agents for aesthetic surgeries except for breast surgeries.^18^ Breast surgeries have a 35.0% risk of developing wound infection. The rate varies with abdominoplasty and decreases in lipectomy alone.
Infection risk is not limited to aesthetic surgeries; in Khoula Hospital an audit was done by the Spine Team to evaluate the rate of surgical wound infections in patients who underwent spine surgeries abroad. A total of 12.0% of patients (15 out of 125) developed surgical wound infection. In contrast to local cases, Khoula Hospital recorded 2.7% of surgical wound infections post-spine surgical procedures from 2013 to 2015.^19^ This supports that surgeries conducted abroad carry a higher complication risk of wound infection.
Surgeons should care for and follow-up with their patients accordingly, a principle often neglected in medical tourism. There is a need to further analyse the influence of this movement on the patient and the healthcare system. Every patient traveling abroad is entitled to receive comprehensive prior advice, including the fact that aesthetic surgeries are universally regarded as invasive procedures in all aspects. Dismissing the risks associated with aesthetic surgeries, especially in aesthetic tourism, is often a common behaviour seen among patients. Therefore, medical tourists should be aware of the possibility of malpractice complications and the need to navigate the country's laws and cultures when pursuing legal action.
Data from the present study supports the need for regulatory oversight by relevant national health authorities to guide patients seeking aesthetic procedures abroad. These efforts should be supported by national awareness campaigns, particularly prior to peak travel and holiday seasons as well as the introduction of a standardised pre-travel safety checklist to promote informed decision-making and patient safety. In addition, these study's findings can be used to advocate for international collaboration through agreements with accredited overseas healthcare providers as well as the establishment of a national registry to monitor complications related to aesthetic procedures performed abroad. Such measures would provide essential data, enable trend detection and support policies aimed at reducing the burden on the public healthcare system. It is imperative that medical tourism services are overseen through appropriate regulation or accreditation pathways, while public awareness is enhanced regarding the verification of institutional credentials and the importance of establishing postoperative follow-up plans.^20^
This study was subject to certain limitations. It did not include Omani patients who underwent surgery in the private sector, as it is mandatory to follow-up with the private sector-surgeon. This was a single centre study and data were extracted using a limited set of search terms related to aesthetic procedures and only the most common aesthetic surgery destinations were included; this may have led to the omission of less common procedures or destinations. Moreover, the correlation between the type of complications and the need for hospital admission was not investigated. Finally, the financial stress on patients or the source country was not formally examined, as there was insufficient data on the exact costs involved. Further studies should be conducted to explore the financial stress on the healthcare system and relation between the variants such as diabetes mellites and the complication outcomes.
5. Conclusion
This study highlights the significant burden of complications from aesthetic procedures performed abroad, as observed in patients treated at Khoula Hospital between 2013 and 2023. Infections, implant-related issues and poor surgical outcomes were the most common complications, often requiring corrective interventions. With the global rise in demand for aesthetic surgery, there is a growing need for patient education on the risks of undergoing procedures in unregulated healthcare systems. Strengthening preoperative counselling by primary care health personnel, implementing standardised follow-up protocols, conducting awareness campaigns before holiday seasons and on world plastic surgery day to help citizens plan their destination and aftercare in home country and fostering international partnerships can help ensure safer, high-quality care. This study underscores the importance of informed decisions and regulatory oversight to reduce the hidden costs of medical tourism.
Authors' contribution
Khalifa Al Alawi: Conceptualization, Methodology, Investigation, Data Curation, Writing - Original Draft, Writing - Review & Editing, Visualization, Project administration. Areej Al-Mamari: Investigation, Data Curation, Writing - Original Draft. Maysa Al-Maawali: Investigation, Data Curation, Writing - Original Draft. Ashima Alkabi: Investigation, Data Curation, Writing - Original Draft. Al-Batul Al-Mufargi: Investigation, Data Curation, Writing - Original Draft. Juhaina Al Tobi: Investigation, Data Curation, Writing - Original Draft. Hoor Al-Khanjari: Investigation, Data Curation. Yasmine Al Balushi: Investigation, Data Curation. Rawan Al Mandhari: Investigation, Data Curation. Rafal Aljadder: Investigation, Data Curation. Sultan Al Shaqsi: Conceptualization, Writing - Review & Editing, Supervision.
Ethics statement
This study was approved by the Khoula Hospital Ethics Committee (PRO052022134) and conducted in accordance with the Declaration of Helsinki. Participant consent was waived by the Khoula Hospital Ethics Committee due to this study's retrospective nature.
Conflict of interest
The authors declare no conflicts of interest.
Funding
No funding was received for this study.
Data availability
Data is available upon reasonable request from the corresponding author.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hartmann D Ruzicka T Gauglitz GG. Complications associated with cutaneous aesthetic procedures. J Dtsch Dermatol Ges 2015; 13:778–86. 10.1111/ddg.12757.26177157 · doi ↗ · pubmed ↗
- 2The Aesthetic Society. Procedural statistics. From: Accessed: Dec 2022. https://www.theaestheticsociety.org/media/procedural-statistics.
- 3Broer PN Levine SM Juran S. Plastic surgery: Quo Vadis? Current trends and future projections of aesthetic plastic surgical procedures in the United States. Plast Reconstr Surg 2014; 133:293e–302e. https://doi.org/10.1097/01.prs.0000438053.21634.84.10.1097/01.prs.0000438053.21634.8424572874 · doi ↗ · pubmed ↗
- 4Gupta V Yeslev M Winocour J Bamba R Rodriguez-Feo C Grotting JC Aesthetic breast surgery and concomitant procedures: incidence and risk factors for major complications in 73,608 cases. Aesthet Surg J 2017; 37:515–27. https://doi.org/10.1093/asj/sjw 238.10.1093/asj/sjw 23828333172 · doi ↗ · pubmed ↗
- 5Montrief T Bornstein K Ramzy M Koyfman A Long BJ. Plastic surgery complications: A review for emergency clinicians. West J Emerg Med 2020; 21:179–89. https://doi.org/10.5811/westjem.2020.6.46415.10.5811/westjem.2020.6.4641533207164 PMC 7673892 · doi ↗ · pubmed ↗
- 6Domanski MC Cavale N. Self-reported 'worth it' rating of aesthetic surgery in social media. Aesthetic Plast Surg 2012; 36:1292–5. https://doi.org/10.1007/s 00266-012-9977-z.10.1007/s 00266-012-9977-z 23052381 · doi ↗ · pubmed ↗
- 7Ross KM Moscoso AV Bayer LR Rosselli-Risal L Orgill DP. Plastic surgery complications from medical tourism treated in a U.S. academic medical center. Plast Reconstr Surg 2018; 141:517e–23e. https://doi.org/10.1097/PRS.0000000000004214.10.1097/PRS.000000000000421429595725 · doi ↗ · pubmed ↗
- 8Klein HJ Simic D Fuchs N Schweizer R Mehra T Giovanoli P Complications after cosmetic surgery tourism. Aesthet Surg J 2017; 37:474–82. 10.1093/asj/sjw 198.28364525 · doi ↗ · pubmed ↗