COVID-19 vaccine uptake in US adults with respiratory diseases: A cross-sectional study
Moosa Tatar, Shahryar Karimi, Masoud Valizadeh, Abhishek Deshpande

TL;DR
This study found that prior vaccination and socioeconomic factors, not respiratory diseases, predict whether US adults get the COVID-19 vaccine.
Contribution
The study reveals that respiratory disease history is not a strong predictor of vaccine uptake, while prior vaccination and socioeconomic factors are.
Findings
Prior influenza and pneumonia vaccination are strongly linked to higher COVID-19 vaccine uptake.
Socioeconomic factors like income, education, and race significantly influence vaccination status.
Respiratory diseases alone do not predict whether individuals receive the COVID-19 vaccine.
Abstract
Despite their proven effectiveness, COVID-19 vaccination rates remain low, particularly among individuals with respiratory diseases. We aimed to examine factors associated with vaccine uptake, focusing on respiratory conditions and prior respiratory vaccination history. We conducted a cross-sectional analysis using 2022 data from the Medical Expenditure Panel Survey. We used logistic regression to examine the association between COVID-19 vaccine uptake and various socioeconomic factors, respiratory conditions, and prior influenza vaccination in US adults. Of 18,155 participants, 3083 (16.98%) were unvaccinated and 15,072 (83.02%) vaccinated. Unvaccinated individuals were more likely younger, male, non-Hispanic Black, immigrants, lower-income, less educated, Southern residents, and smokers. Prior influenza (OR = 1.82, 95% CI [1.39, 2.42]) and pneumonia vaccination (OR = 2.55, 95% CI…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
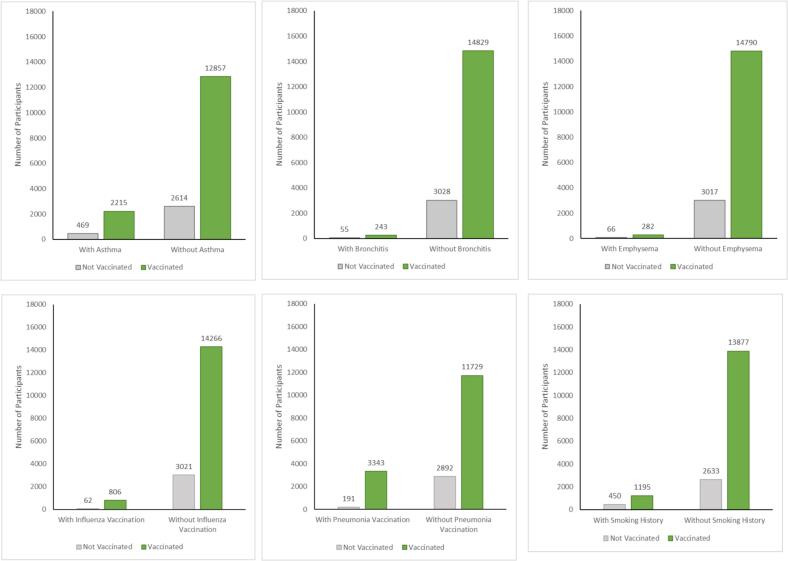 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSARS-CoV-2 and COVID-19 Research · Respiratory viral infections research · Vaccine Coverage and Hesitancy
Introduction
1
Despite the widespread availability and demonstrated effectiveness of COVID-19 vaccines in preventing severe outcomes, many individuals continue to delay or refuse vaccination, and vaccination coverage remains suboptimal (Dudley et al., 2020; Islam et al., 2021; Lazarus et al., 2023; Loomba et al., 2021; Medical Expenditure Panel Survey (MEPS), 2024). Vaccine hesitancy persists as a significant public health challenge, particularly among minority populations and those with high social vulnerability (Khan et al., 2025; Tatar et al., 2023), mainly due to concern about vaccine safety and potential side effects (Khan et al., 2025; Aw et al., 2021; Chirico et al., 2022; Soares et al., 2021; Troiano and Nardi, 2021), and also barriers to vaccination access (Abba-Aji et al., 2022; Newman et al., 2025). Patients with prior respiratory diseases are at higher risk of developing severe COVID-19 and have a higher mortality rate compared to patients without a history of respiratory illness (Beltramo et al., 2021)., (Bouloukaki et al., 2024; Liang and Sun, 2023) Despite the assumption that the most vulnerable individuals (i.e., those with cancer, autoimmune diseases, and chronic lung diseases) would automatically accept the COVID-19 vaccination, individuals with serious comorbid conditions remain hesitant about the COVID-19 vaccine (Tsai et al., 2022).
Although the CDC recommends vaccination for high-risk individuals, including those with asthma, lung disease, pulmonary disease, cystic fibrosis, tuberculosis, smoking history, and transplant-related immunosuppression, vaccination uptake patterns among adults with respiratory conditions remain incompletely characterized (Centers for Disease Control and Prevention, 2025). Understanding factors that influence vaccination decisions in clinically and socially vulnerable populations is important for targeted public health interventions. Previous studies have examined COVID-19 vaccine hesitancy primarily in general populations or focused on single respiratory conditions (Chang et al., 2023; Tavakol et al., 2024). The relationship between prior vaccination (influenza, pneumonia) behaviors and COVID-19 vaccine acceptance across respiratory disease populations has been previously reported (Barri et al., 2025; Saiphoklang and Phadungwatthanachai, 2022; Tang et al., 2024). It also remains unclear how socioeconomic factors interact with respiratory disease status to influence vaccination decisions.
We hypothesized that prior respiratory vaccination history would be associated with increased COVID-19 vaccine uptake, and that this relationship might vary by respiratory disease status. Using nationally representative data could inform targeted vaccination strategies. We analyzed data from the 2022 Medical Expenditure Panel Survey (MEPS) to determine factors associated with COVID-19 vaccine uptake among US adults, with particular emphasis on respiratory diseases (i.e., asthma, bronchitis, or emphysema) and prior vaccination history (i.e., influenza and pneumonia) (Medical Expenditure Panel Survey (MEPS), 2024).
Methods
2
Study design and population
2.1
This retrospective cross-sectional study analyzed data from the MEPS for 2022 (Medical Expenditure Panel Survey (MEPS), 2024), the most recent year with publicly available data. MEPS is a nationally representative survey conducted by the Agency for Healthcare Research and Quality (AHRQ) that collects data on healthcare utilization, expenditures, insurance coverage, and demographic characteristics from households, medical providers, and employers across the United States (Beltramo et al., 2021; Medical expenditure panel survey (MEPS). Medical Expenditure Panel Survey, 2025).
The study population comprised individuals aged 17 and older with complete data on COVID-19 vaccination status and relevant covariates. The original dataset included 22,431 observations. There were 1014 observations with missing data (< 5%). Participants with missing data on key variables were excluded from the analysis. We analyzed individuals aged 17–85 years, consisting of 18,155 individuals. Unweighted analyses were performed to prioritize interpretability and analytical precision in examining associations between covariates and vaccination status, rather than generating nationally representative estimates. This approach is consistent with analytical frameworks focused on identifying predictors of health behaviors rather than population-level estimates. We conducted unweighted models to prioritize interpretability and analytical precision.
This study utilized publicly available, de-identified secondary data and did not involve direct contact with human participants. Therefore, it was exempt from institutional review board oversight in accordance with federal regulations governing human subjects research (45 CFR 46.104).
Measures
2.2
The primary outcome was COVID-19 vaccine uptake, defined as a binary variable indicating receipt of at least one dose of any COVID-19 vaccine versus no vaccination. This variable indicated whether individuals ever had a COVID-19 vaccine or booster shot. The primary exposure variable was history of respiratory disease, defined as the presence of at least one of the following conditions: asthma (asthma diagnosis), bronchitis (a person has had chronic bronchitis in the last 12 months), or emphysema (emphysema diagnosis). Individual binary variables for each respiratory condition and lung cancer were also examined. Respiratory diseases were identified using International Classification of Diseases, 10th Revision (ICD-10) diagnostic codes (asthma: J45; bronchitis: J20; emphysema: J43; lung cancer: C34) as recorded in MEPS administrative data and validated through medical provider reports. Please see Table A1 in the Appendix.
Additional binary indicators were constructed for history of influenza and pneumonia vaccination based on MEPS variable definitions, defined as having ever received an influenza or pneumonia vaccination, respectively. All outcome and covariate variables were derived from MEPS documentation and represent either administrative records or validated self-reported physician diagnoses, as specified in the survey methodology.
Covariates identified a priori as potential confounders based on existing literature included sociodemographic characteristics: age (continuous), sex assigned at birth, race/ethnicity, immigration status, household income level, educational attainment, geographic region, and smoking status. Complete variable definitions and coding specifications are provided in the supplementary materials (Table A1, Table A2).
Statistical analysis
2.3
Descriptive statistics were used to characterize the study population. Categorical variables are presented as frequencies and percentages, while continuous variables are presented as means and standard deviations. Differences between groups were assessed using chi-square tests for categorical variables and t-tests or ANOVA for continuous variables, as appropriate. To investigate associations between prior influenza vaccination, history of respiratory disease, and COVID-19 vaccine uptake, we conducted a series of multivariable logistic regression analyses.
First, we performed the primary analysis that included all participants and examined associations between COVID-19 vaccine uptake (dependent variable) and independent variables including, influenza vaccination history, pneumonia vaccination history, respiratory diseases (asthma, bronchitis, emphysema) and lung cancer while adjusting for relevant covariates (age, sex, race/ethnicity, immigration status, income, education, geographic region, and smoking status).
Second, we performed a subgroup analysis that included 1) individuals with at least one respiratory disease 2) individuals without any respiratory diseases, to examine the association between COVID-19 vaccine uptake and influenza vaccination history, pneumonia vaccination history, and lung cancer while adjusting for relevant covariates.
Third, we performed a subgroup analysis that included 1) individuals with prior influenza vaccination history 2) individuals without influenza vaccination history, to examine the association between COVID-19 vaccine uptake and respiratory disease, pneumonia vaccination, and lung cancer, and adjusting for relevant covariates (age, sex, race/ethnicity, etc.). In all multivariable logistic regression models, we estimated odds ratios (ORs) and 95% confidence intervals (CIs). Multicollinearity was assessed using variance inflation factors (VIFs), with values >5 indicating significant multicollinearity. Model fit was assessed using measures such as the pseudo-R-squared (Nagelkerke R2), Akaike Information Criterion (AIC), and Bayesian Information Criterion (BIC). Model performance was further evaluated using Monte Carlo cross-validation. The dataset was randomly split into training (70%) and testing (30%) subsets across 10 independent iterations. In each iteration, the model was trained on the training set and evaluated on the test set. The average prediction accuracy across all 10 iterations was used to estimate accuracy and out-of-sample performance.
All statistical analyses were performed using RStudio version 4.0.2 (R Core Team, 2020). A p-value of <0.05 was considered statistically significant. Given the secondary nature of this analysis using existing survey data, no formal sample size calculation was performed.
Results
3
Among 18,155 participants, 3083 (16.98%) were unvaccinated and 15,072 (83.02%) were vaccinated against COVID-19 (Table 1). Vaccination status was significantly associated with multiple demographic and health-related variables (P < 0.01). Unvaccinated individuals were more likely to be younger, with 18.42% aged 17–25 years and 18.94% aged 26–34 years, compared with 9.42% and 11.61%, respectively, among vaccinated individuals. Similar patterns were observed in the 35–54 age group (34.19% unvaccinated vs. 29.06% vaccinated). Conversely, older age groups were underrepresented among unvaccinated individuals: 14.63% aged 55–64 years and 13.82% aged ≥65 years, compared with 17.85% and 32.06%, respectively, among vaccinated individuals.Table 1. Baseline characteristics by COVID-19 vaccination status in US adults (Medical Expenditure Panel Survey, 2022).Table 1. VariablesNot vaccinatedVaccinatedTotalP-ValueParticipant No. (%)3083 (16.98%)15,072 (83.02%)18,155Age Group< 0.01 17–25 years, No. (%)568 (18.42%)1420 (9.42%)1988 26–34 years, No. (%)584 (18.94%)1750 (11.61%)2334 35–54 years, No. (%)1054 (34.19%)4380 (29.06%)5434 55–64 years, No. (%)451 (14.63%)2690 (17.85%)3141 ≥ 65 years, No. (%)426 (13.82%)4832 (32.06%)5258Sex< 0.01 Male, No. (%)1535 (49.79%)6856 (45.49%)8391 Female, No. (%)1548 (50.21%)8216 (54.51%)9764Race/Ethnicity< 0.01 White, non-Hispanic, No. (%)1757 (56.99%)8601 (57.07%)10,358 Black, non-Hispanic, No. (%)523 (16.96%)2101 (13.94%)2624 Hispanic or Latino, No. (%)612 (19.85%)3002 (19.92%)3614 Other/Multi-race, No. (%)191 (6.20%)1368 (9.08%)1559Immigrant (foreign-born), No. (%)< 0.01 No, No. (%)2669 (86.57%)11,904 (78.98%)14,573 Yes, No. (%)414 (13.43%)3168 (21.02%)3582Income Level< 0.01 Lower class: ≤ 30,001–58,021–94,001–153,000, No. (%)41 (1.33%)686 (4.55%)727Education Level< 0.01 No degree, No. (%)725 (23.52%)2126 (14.11%)2851 Grade school, No. (%)196 (6.36%)493 (3.27%)689 High school, No. (%)1462 (47.42%)5318 (35.28%)6780 Some college, No. (%)303 (9.83%)1461 (9.69%)1764 Bachelor's degree, No. (%)380 (12.33%)5167 (34.28%)5547 Advanced degrees, No. (%)17 (0.55%)507 (3.36%)524Region< 0.01 Midwest, No. (%)691 (22.41%)2965 (19.67%)3656 Northeast, No. (%)318 (10.31%)2542 (16.87%)2860 South, No. (%)1428 (46.32%)5584 (37.05%)7012 West, No. (%)646 (20.95%)3981 (26.41%)4627Respiratory Diseases (Asthma, Bronchitis, Emphysema)0.35 No, No. (%)2562 (83.10%)12,630 (83.80%)15,192 Yes, No. (%)521 (16.90%)2442 (16.20%)2963Asthma0.48 No, No. (%)2614 (84.79%)12,857 (85.30%)15,471 Yes, No. (%)469 (15.21%)2215 (14.70%)2684Bronchitis0.55 No, No. (%)3028 (98.22%)14,829 (98.39%)17,857 Yes, No. (%)55 (1.78%)243 (1.61%)298Emphysema0.36 No, No. (%)3017 (97.86%)14,790 (98.13%)17,807 Yes, No. (%)66 (2.14%)282 (1.87%)348Lung Cancer0.03 No, No. (%)3079 (99.87%)15,009 (99.58%)18,088 Yes, No. (%)4 (0.13%)63 (0.42%)67Smoking Status< 0.01 No, No. (%)2633 (85.4%)13,877 (92.07%)16,510 Yes, No. (%)450 (14.6%)1195 (7.93%)1645Influenza Vaccination< 0.01 No, No. (%)3021 (97.99%)14,266 (94.65%)17,287 Yes, No. (%)62 (2.01%)806 (5.35%)868Pneumonia Vaccination< 0.01 No, No. (%)2892 (93.80%)11,729 (77.82%)14,621 Yes, No. (%)191 (6.20%)3343 (22.18%)3534Chi-Square and Fisher's Exact Test are both used to analyze relationships between categorical variables.
Also, compared to the vaccinated group, unvaccinated individuals were more likely to be male, non-Hispanic Black, non-immigrants, have lower income, be less educated, reside in the South, and be smokers. Unvaccinated individuals were less likely to receive influenza vaccinations (97.99% not vaccinated vs. 94.65%) or pneumonia vaccinations (93.80% vs. 77.82%). In contrast, the prevalence of respiratory diseases (asthma, bronchitis, emphysema) and asthma alone did not significantly differ between the two groups (P > 0.05). However, a statistically significant difference was noted in the prevalence of lung cancer (P = 0.03), with a lower proportion of lung cancer reported in the unvaccinated group (0.13%) compared to the vaccinated group (0.42%). Fig. 1 also illustrates COVID-19 vaccination status among all participants by respiratory disease, influenza and pneumonia vaccination, and smoking history.Fig. 1COVID-19 Vaccination Status Among US Adults by Respiratory Disease, Vaccination History, and Smoking Status (Medical Expenditure Panel Survey, 2022).Fig. 1
Primary model validation demonstrated adequate performance with a pseudo-R^2^ of 0.13, AIC of 14,457.76, cross-validation accuracy of 83.00%, and out-of-sample error rate of 16.93% (see Table A3, Appendix). We used unweighted models and included only participants with complete data on vaccination status and key covariates. Some subgroup analyses had limited sample sizes, requiring cautious interpretation of estimates with wider confidence intervals.
Table 2, Table 3 present the results of the primary multivariable logistic regression model predicting COVID-19 vaccination uptake among all participants. Table 2 focuses on respiratory and vaccination history, while Table 3 details socioeconomic factors. The results showed that influenza vaccination (OR = 1.82, 95% CI [1.39, 2.42]), pneumonia vaccination (OR = 2.55, 95% CI [2.14, 3.04]), were significantly associated with higher COVID-19 vaccination uptake. Smoking was associated with lower COVID-19 vaccination uptake (OR = 0.66, 95% CI [0.58, 0.76]). Respiratory diseases (asthma, bronchitis, and emphysema) were not significantly associated with COVID-19 vaccination uptake.Table 2. Multivariable logistic regression: association of respiratory disease and prior vaccination with COVID-19 vaccine uptake among US adults (Medical Expenditure Panel Survey, 2022).Table 2. VariablesOdds Ratio95% Confidence IntervalPrior Vaccination History Influenza Vaccination1.82[1.39, 2.42] Pneumonia Vaccination2.55[2.14, 3.04]Respiratory Diseases Asthma1.06[0.94, 1.19] Bronchitis0.93[0.67, 1.30] Emphysema0.78[0.58, 1.07] Lung Cancer2.41[0.95, 8.11]Note: Model adjusted for age, sex, race/ethnicity, immigration status, income level, education level, geographic region, and smoking status.Table 3. Multivariable logistic regression: association of socioeconomic and demographic factors with COVID-19 vaccine uptake among US adults (Medical Expenditure Panel Survey, 2022).Table 3. VariablesOdds Ratio95% Confidence IntervalSmoking Status Smoking History0.66[0.58, 0.76]Age Group (Ref: 17–25) 26–340.64[0.55, 0.74] 35–540.84[0.73, 0.96] 55–641.35[1.15, 1.57] > 652.19[1.87, 2.57]Sex Female1.14[1.05, 1.24]Race/Ethnicity (Ref: White) Black1.41[1.25, 1.60] Hispanic1.58[1.39, 1.80] Other1.49[1.25, 1.78]Immigrant Status Immigrant (Foreign-born)1.68[1.47, 1.93]Income Level (Ref: Lower class) Lower Middle Class1.35[1.22, 1.50] Middle Class1.63[1.41, 1.89] Upper Middle Class2.17[1.78, 2.67] Upper Class2.54[1.83, 3.61]Education Level (Ref: No degree) Advanced Degrees7.11[4.41, 12.24] Bachelor's Degrees4.30[3.67, 5.05] Grade School1.07[0.88, 1.32] High School1.35[1.20, 1.51] Some Colleges1.71[1.45, 2.02]Region (Ref: Midwest) Northeast1.68[1.44, 1.95] South0.91[0.82, 1.02] West1.30[1.15, 1.48]Note: These Odds Ratios (ORs) are derived from the same multivariable logistic regression model as Table 2. Estimates for socioeconomic variables are adjusted for one another and for respiratory health factors (asthma, bronchitis, emphysema, lung cancer, and prior vaccination). These should be interpreted as direct associations conditional on the other covariates in the model, rather than total causal effects.
Table 4 presents the results of the logistic regression model predicting COVID-19 vaccination uptake among participants with and without respiratory disease. The model showed that among participants with at least one respiratory disease, prior influenza vaccination (OR = 1.78, 95% CI [1.05, 3.21]) and pneumonia vaccination (OR = 2.09, 95% CI [1.50, 2.94]), were significantly associated with higher COVID-19 vaccination uptake. Smoking was associated with lower COVID-19 vaccination uptake (OR = 0.53, 95% CI [0.40, 0.70]), while lung cancer was not significantly associated with COVID-19 vaccination uptake. Also, among participants without respiratory disease, influenza vaccination (OR = 1.87, 95% CI [1.37, 2.61]), and pneumonia vaccination (OR = 2.79, 95% CI [2.28, 3.44]), were significantly associated with higher COVID-19 vaccination uptake. Conversely, Smoking was associated with lower COVID-19 vaccination uptake (OR = 0.70, 95% CI [0.61, 0.82]). Lung cancer was not significantly associated with COVID-19 vaccination uptake. Table 5 presents the results of the logistic regression model for COVID-19 vaccination uptake among participants with and without prior influenza vaccine history. The model revealed that among participants with influenza vaccine history, prior pneumonia vaccination (OR = 4.79, 95% CI [2.51, 9.37]) was significantly associated with higher COVID-19 vaccination uptake. Also, among participants without influenza vaccine history, prior pneumonia vaccination (OR = 2.51, 95% CI [2.10, 3.01]) was significantly associated with higher and smoking (OR = 0.65, 95% CI [0.57, 0.64]) was significantly associated with lower COVID-19 vaccination uptake.Table 4. Multivariable logistic regression: association of respiratory disease and prior vaccination with COVID-19 vaccine uptake among US adults by respiratory disease (Medical Expenditure Panel Survey, 2022).Table 4. VariablesAt Least One Respiratory DiseaseWithout any Respiratory DiseaseOdds Ratio95% Confidence IntervalOdds Ratio95% Confidence IntervalInfluenza Vaccination Yes1.78[1.05, 3.21]1.87[1.37, 2.61]Pneumonia Vaccination Yes2.09[1.50, 2.94]2.79[2.28, 3.44]Lung Cancer Yes2.96[0.84, 18.82]2.16[0.61, 13.83]Smoking Status Smoking History0.53[0.40, 0.70]0.70[0.61, 0.82]Note: Models are adjusted for age, sex, race/ethnicity, immigration status, income level, education level, and geographic region.Table 5. Multivariable logistic regression: association of respiratory disease and prior vaccination with COVID-19 vaccine uptake among US adults by influenza vaccine history (Medical Expenditure Panel Survey, 2022).Table 5. VariablesWith Influenza Vaccine HistoryWithout Influenza Vaccine HistoryOdds Ratio95% Confidence IntervalOdds Ratio95% Confidence IntervalPneumonia Vaccination Yes4.79[2.51, 9.37]2.51[2.10, 3.01]Respiratory Diseases Asthma0.73[0.36, 1.56]1.07[0.95, 1.21] Bronchitis0.43[0.13, 1.54]0.98[0.70, 1.40] Emphysema0.78[0.25, 2.89]0.78[0.57, 1.07] Lung CancerNA*2.30[0.90, 7.78]Smoking Status Smoking History1.16[0.56, 2.57]0.65[0.57, 0.74]Note: * Estimates for Lung Cancer in the “With Influenza Vaccine History” subgroup were inflated and unstable due to small sample size; therefore, reliable Odds Ratios could not be calculated (NA). Models are adjusted for age, sex, race/ethnicity, immigration status, income level, education level, and geographic region.
Discussion
4
This nationally representative analysis of US adults shows that prior vaccination history, particularly influenza and pneumonia vaccination, was significantly associated with increased COVID-19 vaccination uptake, while respiratory disease presence was not. Socioeconomic factors such as higher income and education were strongly associated with vaccination acceptance across all subgroups. These findings highlight the importance of routine immunization programs as potential pathways to broader vaccine coverage and suggest that vaccination behavior may be more likely influenced by established health-seeking patterns than by specific disease risk factors.
Our findings are consistent with prior research investigating the effect of socioeconomic factors' effect on COVID-19 vaccination uptake (Aw et al., 2021; Soares et al., 2021). A scoping review evaluated COVID-19 vaccine hesitancy and its determinants among high-income countries and reported that younger age, being female, not being of white ethnicity, and lower education were associated with increased vaccine hesitancy (Aw et al., 2021). In addition, several factors, including being younger, loss of income during the pandemic, and having no intention of taking the influenza vaccine, were associated with both refusal and delay in COVID-19 vaccination in Portugal (Soares et al., 2021). Another study among Medicare enrollees across counties in the US found that Black/African Americans had the lowest influenza immunization rates, and also, social vulnerability (e.g., lower income, lower education levels) decreases rates of influenza vaccination in minority communities (Tatar et al., 2023).
While patients with prior respiratory diseases are at higher risk of developing severe COVID-19 and negative health outcomes compared to the general population (Beltramo et al., 2021; Bouloukaki et al., 2024; Liang and Sun, 2023), the association between prior respiratory diseases and vaccine uptake appears to be mixed. We did not find a significant association between respiratory diseases and COVID-19 vaccination uptake; however, some studies reported that patients with asthma who had worse clinical status, including respiratory symptoms (e.g., cough, breathlessness, and chest tightness) and functional status (e.g., activity, sleep, and energy levels), and also patients with poorly controlled asthma, and individuals using biologic therapies were more likely to be hesitant about getting vaccinated (Bouloukaki et al., 2024; Chang et al., 2023). While immunological diseases are not a contraindication for COVID-19 vaccination, there are situations involving severe allergic reactions or acute immunological distress (e.g., acute severe illness) where physicians may suggest avoiding, delaying, or monitoring more strictly after COVID-19 vaccination (Bian et al., 2022; Yan et al., 2021). One study in China reported that the COVID-19 vaccination rate in asthmatic patients was lower than that of the general population (Chang et al., 2023). Our findings are consistent with another study in Greece that found that individuals with asthma or Chronic Obstructive Pulmonary Disease (COPD) who had previously received the influenza vaccine or more than three COVID-19 vaccine doses were positively associated with regular COVID-19 vaccinations (Beltramo et al., 2021). In addition, our results showed that individuals with a history of smoking had lower COVID-19 vaccination uptake among all participants and among participants with at least one respiratory disease. Individuals with a history of smoking are less likely to adhere to preventive measures in general and have lower adherence to other vaccines (Peña et al., 2024). Despite smokers having higher risks of COVID-19 hospitalizations and deaths (Neira et al., 2021; Patanavanich et al., 2023), the use of cigarettes, e-cigarettes, and marijuana has not been reported to be associated with COVID-19 hesitancy (Yang et al., 2021).
Despite the assumption that individuals with severe disease and underlying comorbidities (e.g., cancer, autoimmune diseases, and chronic lung diseases) would be more likely to accept the COVID-19 vaccination, these individuals remained hesitant about the COVID-19 vaccine (Tsai et al., 2022). Similarly, we did not find a significant association between lung cancer and COVID-19 vaccination uptake. COVID-19 vaccination hesitancy rates in cancer patients vary significantly cross-culturally, and cancer patients have unique concerns about vaccination, including interactions with cancer treatments (Tsai et al., 2022). Misconceptions in patients with lung cancer contribute to COVID-19 vaccine hesitancy (Zhuang et al., 2021). Even with demonstrated data on the efficacy of COVID-19 vaccines at preventing COVID-19 illness, including severe disease, and minimal safety concerns (Baden et al., 2021), some sociodemographic groups are differentially impacted by exposure to misinformation, and scientific-sounding misinformation is more strongly associated with declines in vaccination intent (Loomba et al., 2021).
This study utilizes the strength of the nationally representative MEPS dataset to better understand COVID-19 vaccination uptake in the US adult population. By incorporating socioeconomic, respiratory, and vaccination history factors, we aimed to characterize the determinants involved in COVID-19 vaccine hesitancy. Given its cross-sectional design, this study is limited to identifying associations rather than establishing causal relationships. The reliance on self-reported data, particularly self-reported vaccination status, which was not validated against medical records, introduces the potential for reporting and measurement bias. Also, the MEPS dataset does not allow us to determine the temporal order of respiratory illness diagnosis and COVID-19 vaccine uptake. Accordingly, study findings should be interpreted with caution, and we acknowledge this as a limitation of our analysis. As with all observational studies, the influence of unmeasured confounders cannot be entirely ruled out. Furthermore, some subgroup analyses had limited sample sizes, requiring cautious interpretation of estimates with wide confidence intervals. We also acknowledge that sparse data in certain subgroups may affect the precision of some estimates, particularly odds ratios. Because the MEPS focuses on the non-institutionalized population and excludes specific groups (e.g., military personnel and institutionalized populations), the findings have limited generalizability to the entire U.S. population. Its overlapping longitudinal design may also affect sample size and should be considered when interpreting results or guiding policy.
The results of this study suggest that promoting routine vaccinations, particularly influenza vaccination, may serve as a pathway to improving COVID-19 vaccine coverage. Our findings indicate that targeted outreach to individuals with lower socioeconomic status may be a more effective approach for increasing vaccine uptake than disease-specific campaigns for respiratory conditions.
Conclusions
5
Prior vaccination history appears to be a stronger predictor of COVID-19 vaccine uptake than the presence of respiratory diseases among US adults. Individuals with a history of influenza and pneumonia vaccinations were significantly more likely to accept the COVID-19 vaccine, while the presence of underlying respiratory diseases did not significantly affect COVID-19 vaccine uptake. These findings highlight the importance of routine immunization programs as a strategy for broader vaccine coverage. Finally, it appears that addressing socioeconomic disparities through targeted interventions may be a more effective strategy for improving vaccine coverage than disease-specific approaches.
Data sharing statement
No additional data are available.
Patient and public involvement statement
No patients and the public were involved in this research, and the article does not involve human participants and does not contain personal medical information.
CRediT authorship contribution statement
Moosa Tatar: Writing – review & editing, Writing – original draft, Visualization, Validation, Supervision, Project administration, Methodology, Investigation, Data curation, Conceptualization. Shahryar Karimi: Writing – review & editing, Validation, Software, Methodology, Investigation, Formal analysis, Data curation, Conceptualization. Masoud Valizadeh: Writing – review & editing, Validation, Methodology, Investigation, Formal analysis, Data curation, Conceptualization. Abhishek Deshpande: Writing – review & editing, Validation, Methodology, Investigation, Formal analysis.
Disclaimer
The views or opinions expressed herein are those of the author and shall not be attributed to and/or does not imply endorsement, recommendation or approval by the Options Clearing Corporation - a systemically important financial market utility.
Funding sources
The authors have no financial disclosures to report.
Declaration of competing interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Abba-Aji M.Stuckler D.Galea S.Mc Kee M.Ethnic/racial minorities’ and migrants’ access to COVID-19 vaccines: a systematic review of barriers and facilitators J. Migration Health 5202210008610.1016/j.jmh.2022.100086 PMC 885561835194589 · doi ↗ · pubmed ↗
- 2Aw J.Seng J.J.B.Seah S.S.Y.Low L.L.COVID-19 vaccine hesitancy—a scoping review of literature in high-income countries Vaccines 98202190010.3390/vaccines 9080900 PMC 840258734452026 · doi ↗ · pubmed ↗
- 3Baden L.R.El Sahly H.M.Essink B.Efficacy and safety of the m RNA-1273 SARS-Co V-2 vaccine N. Engl. J. Med.384520214034163337860910.1056/NEJ Moa 2035389 PMC 7787219 · doi ↗ · pubmed ↗
- 4Barri S.Al-Dahir S.Heyer K.Influence of respiratory disease experiences on COVID-19 vaccine acceptance: a study from southeastern Louisiana Front. Public Health 132025159386110.3389/fpubh.2025.1593861 PMC 1239414340893203 · doi ↗ · pubmed ↗
- 5Beltramo G.Cottenet J.Mariet A.-S.Chronic respiratory diseases are predictors of severe outcome in COVID-19 hospitalised patients: a nationwide study Eur. Respir. J.586202110.1183/13993003.04474-2020 PMC 813592734016619 · doi ↗ · pubmed ↗
- 6Bian S.Li L.Wang Z.Allergic reactions after the administration of COVID-19 vaccines Front. Public Health 10202287808110.3389/fpubh.2022.878081 PMC 915225235655467 · doi ↗ · pubmed ↗
- 7Bouloukaki I.Christodoulakis A.Papageorgakopoulou S.Tsiligianni I.The prevalence and determinants of hesitancy for regular COVID-19 vaccination among primary healthcare patients with asthma or COPD in Greece: a cross-sectional study Vaccines 12420244143867579610.3390/vaccines 12040414 PMC 11054093 · doi ↗ · pubmed ↗
- 8Centers for Disease Control and Prevention. People with Certain Medical Conditions and COVID-19 Risk Factors. COVID-19 2025; https://www.cdc.gov/covid/risk-factors/index.html#:∼:text=Like%20adults%2C%20children%20and%20teens,very%20sick%20from%20COVID%2D 19. Accessed July 11, 2015.