Secondary syphilis mimicking marginal zone B-cell lymphoma in a 70-year-old man
Hannah Gier, Shannon Trotter

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
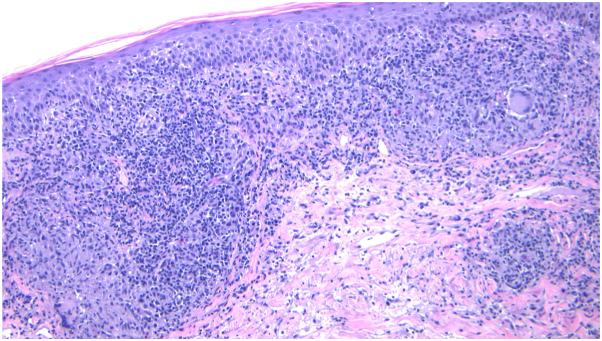 Figure 1
Figure 1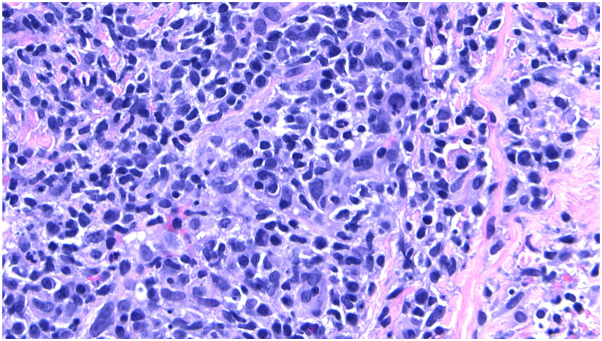 Figure 2
Figure 2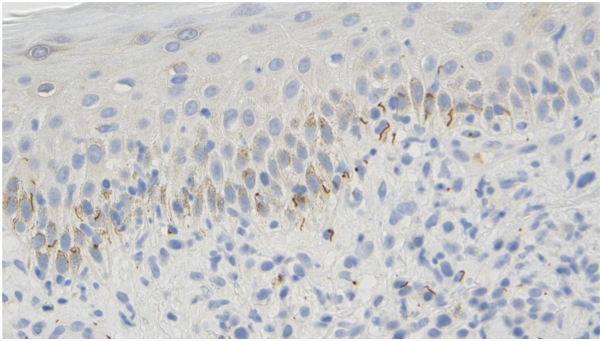 Figure 3
Figure 3 Figure 4
Figure 4 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSyphilis Diagnosis and Treatment
Case description
A 70-year-old man presents with a 4-year history of a pruritic eruption involving the trunk, head, neck, and extremities. He reports intermittent fever, chills, and fatigue. Positron emission tomography/computed tomography imaging demonstrates diffuse hypermetabolic cervical, axillary, and inguinal lymphadenopathy, raising concern for lymphoma. A bone marrow biopsy reveals clonal B cells. Skin examination shows erythematous papules and nodules with overlying scale. A skin biopsy demonstrates compact orthokeratosis, angiocentric and lichenoid lymphocytic inflammation, and granulomas with abundant plasma cells. Immunohistochemical staining for Treponema pallidum is positive, and the rapid plasma reagin (RPR) titer is 1:2048. Flow cytometry identifies low-level monoclonal B cells without atypia (Fig 1, Fig 2, Fig 3).Fig 110**×** magnification: dense superficial and deep perivascular and lichenoid lymphocytic infiltrate.Fig 240**×** magnification: prominent perivascular lymphocytic infiltrate with numerous plasma cells.Fig 3. Immunoperoxidase stain highlighting treponemal organisms within the tissue.
The patient is diagnosed with secondary syphilis. Due to a penicillin allergy, he is treated with doxycycline 100 mg twice daily for 28 days, resulting in marked clinical improvement. His papulonodular eruption significantly regresses, with decreased erythema and residual postinflammatory hyperpigmentation. The patient’s systemic symptoms also resolve, and follow-up RPR titers decrease to 1:4 (Figs 4 and 5).Fig 4. Erythematous plaques and nodules with overlying scale involving the forehead, glabella, eyebrows and scalp at initial presentation.Fig 5. Marked clinical improvement after a 28-day course of doxycycline 100 mg twice daily. Residual post-inflammatory hyperpigmentation on the forehead, glabella, eyebrows and scalp.
Question 1: Which of the following best explains the presence of clonal B cells in this patient with a reactive lymphoplasmacytic infiltrate and positive treponemal stain?
- **A.**Early marginal zone lymphoma with secondary infection
- **B.**Nodal involvement by cutaneous pseudolymphoma
- **C.**Sampling error from skin adjacent to a neoplastic focus
- **D.**Clonal B-cell expansion secondary to infection
- **E.**Technical artifact during flow cytometry
Correct answer: D. Clonal B-cell expansion secondary to infection.
Discussion
This case highlights a rare example of secondary syphilis mimicking marginal zone B-cell lymphoma. Though the presence of clonal B cells often suggests a lymphoproliferative disorder, reactive conditions like syphilis can also induce B-cell clonality.1^,^2 Clonal redemption is a process in which memory B-cell clones resurge in response to an antigenic stimulation caused by a pathogen, such as T pallidum, without malignant transformation. This phenomenon can complicate diagnosis and lead to misdiagnosis as lymphoma if proper clinicopathologic correlation is not performed.
Histologically, marginal zone B-cell lymphoma and secondary syphilis may share features, including plasma cell-rich infiltrates and dermal lymphoid aggregates.1, 2, 3, 4 However, the presence of spirochetes on treponemal immunostaining, positive RPR and treponemal antibody serologies, and clinical response to antibiotic therapy all support an infectious rather than neoplastic etiology. Additional histologic features that favor syphilis include a lichenoid band of inflammation, elongated rete ridges, and endothelial swelling.2^,^3
While secondary syphilis is a known mimic, this case shows a lesser-reported manifestation resembling cutaneous B-cell lymphoma both clinically and histologically, with reactive B-cell clonality further complicating diagnosis in an atypical demographic. It emphasizes the need to integrate histopathologic, immunohistochemical, and serologic findings, as clonal redemption remains an underrecognized mechanism that can mislead clinicians toward malignancy.
Conflicts of interest
None disclosed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Correia E.Gleason L.Krishnasamy S.Cohen A.Bhatti S.Nikbakht N.Secondary syphilis mimicking marginal zone B-cell lymphoma JAAD Case Rep 202021505310.1016/j.jdcr.2021.11.02635059487 PMC 8760404 · doi ↗ · pubmed ↗
- 2Khalil S.Donthi D.Gru A.A.Cutaneous reactive B-cell lymphoid proliferations J Cutan Pathol 4910202289891610.1111/cup.1426435656820 · doi ↗ · pubmed ↗
- 3Flamm A.Parikh K.Xie Q.Kwon E.J.Elston D.M.Histologic features of secondary syphilis: a multicenter retrospective review J Am Acad Dermatol 73620151025103010.1016/j.jaad.2015.08.06226464219 · doi ↗ · pubmed ↗
- 4Peeling R.W.Mabey D.Kamb M.L.Chen X.S.Radolf J.D.Benzaken A.S.Syphilis Nat Rev Dis Primers 320171707310.1038/nrdp.2017.73PMC 580917629022569 · doi ↗ · pubmed ↗