Effectiveness of outdoor fitness equipment intervention on health outcomes: a systematic review and meta-analysis
Zhi-Yuan Tang, Yu-Qin Ji, Yi-Su Zhu, Hong-Bin Xiang, Qiang Ye

TL;DR
This study reviews how outdoor fitness equipment improves physical activity, fitness, and mental health, showing significant benefits across multiple health outcomes.
Contribution
The study provides a systematic review and meta-analysis of OFE interventions, revealing their effectiveness on diverse health outcomes.
Findings
OFE interventions significantly improve physical activity and physical fitness, including cardiorespiratory fitness and muscle strength.
Psychological health benefits include improved mental well-being, reduced loneliness, and better self-efficacy.
Health-related improvements include better quality of life, reduced fall risk, and improved blood lipid levels.
Abstract
Outdoor fitness equipment (OFE) is an environmental infrastructure in public areas to facilitate structured physical activity. This systematic review aims to evaluate the effectiveness of OFE intervention on health outcomes. We searched five online databases (PubMed, Scopus, Web of Science, Embase, and The Cochrane Library) from inception to Nov 3, 2025. Randomized and non-randomized controlled studies that employed OFE interventions were included. We assessed methodological quality using the modified Downs and Black checklist. Primary outcomes included physical activity, physical fitness, psychological well-being, and other health-related results. Fourteen studies underwent systematic review, of which eleventh provided sufficient data for meta-analyses, and 11 were rated as high quality. The OFE intervention notably increased physical activity. Significantly improvements were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
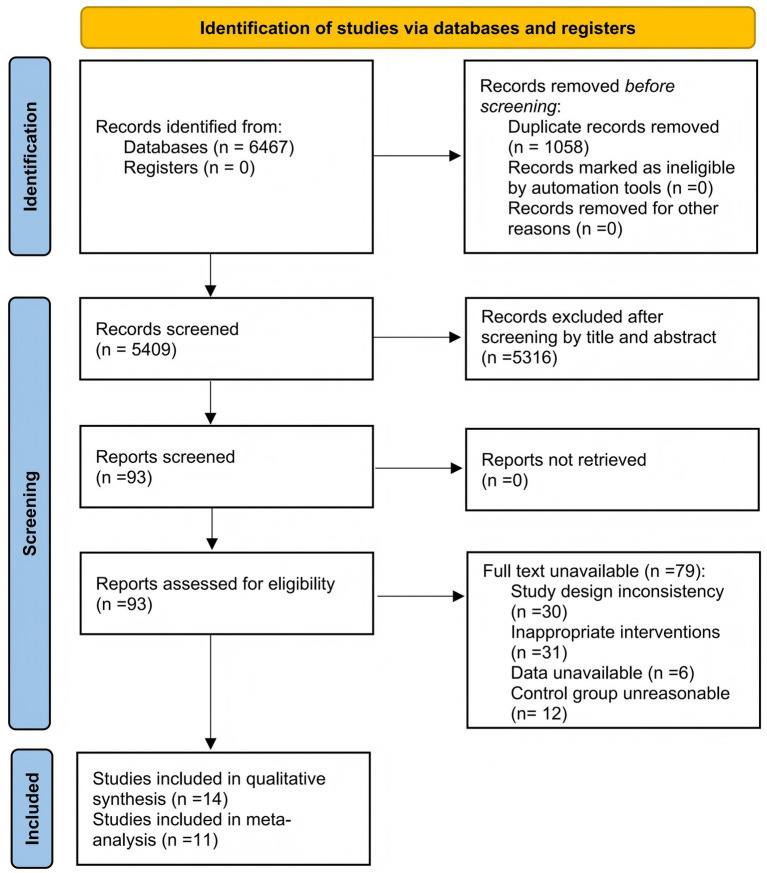 Figure 1
Figure 1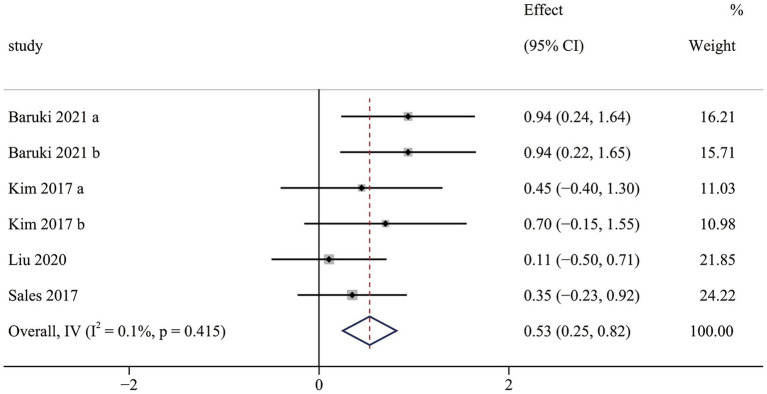 Figure 2
Figure 2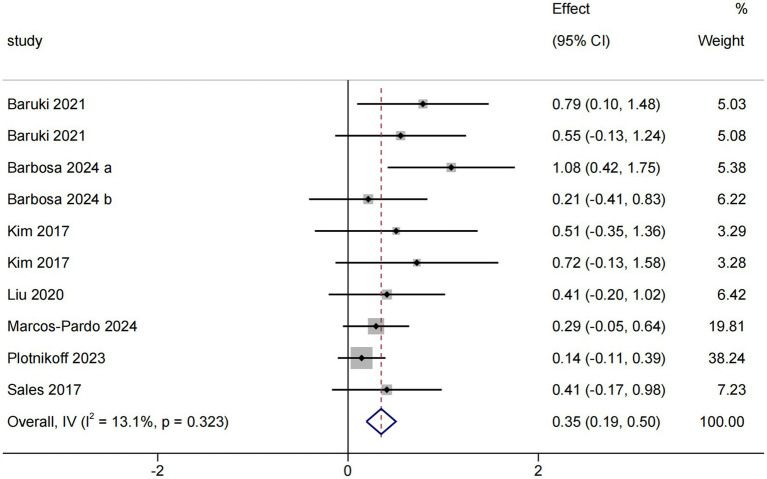 Figure 3
Figure 3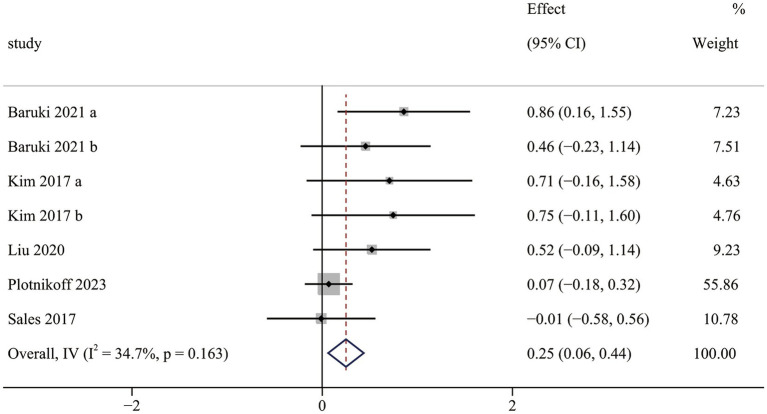 Figure 4
Figure 4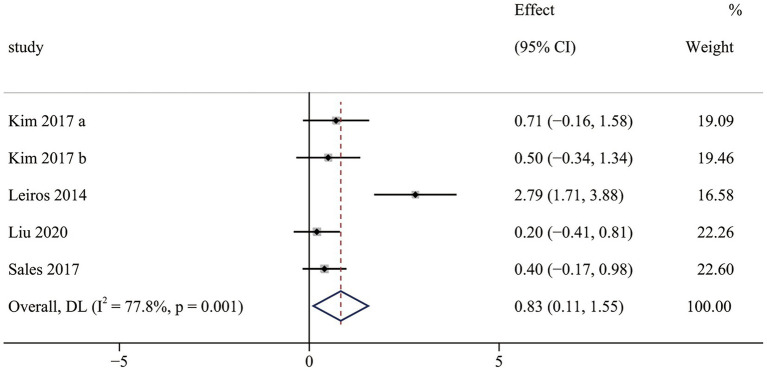 Figure 5
Figure 5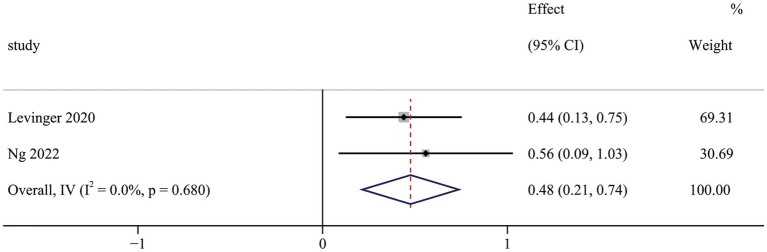 Figure 6
Figure 6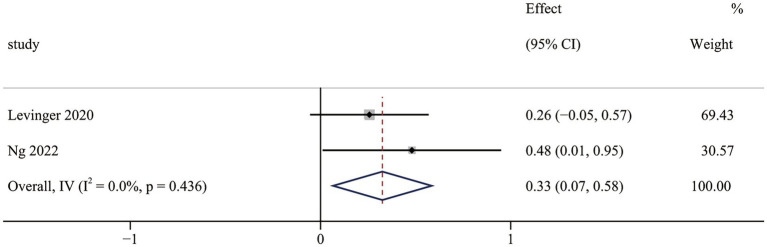 Figure 7
Figure 7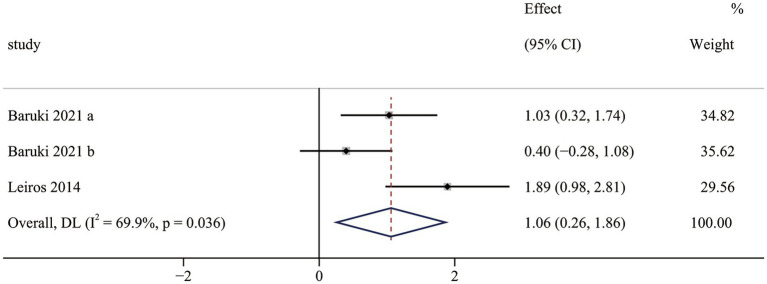 Figure 8
Figure 8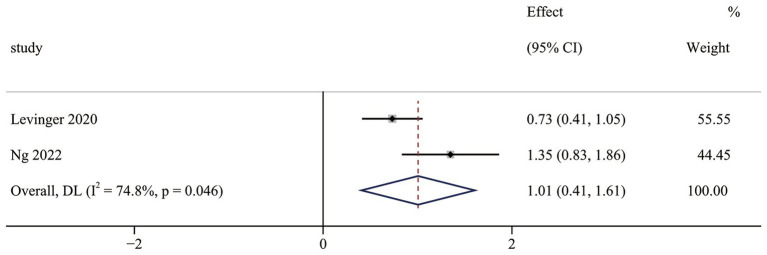 Figure 9
Figure 9| First author, year, Country | Study design | Participant characteristics | No. of OFE and type of exercise | Intervention using OFE | Supervision | Adherence | Intensity | Outcome measured | Main findings | |
|---|---|---|---|---|---|---|---|---|---|---|
| Mean age; sex-M%; | Sample size (IG/CG) | |||||||||
| Baruki et al. ( | RCT | 40–70; M-3.4% | 10/10/9 | 7 | STG and CTG: 16 × 3 × 50–60 min/ week | Researcher | NR (Dropout if >3 absences) | 40–70% HRR/RPE 11–13 | II: 6-Minute Walk Test; Sit-to-Stand; elbow flexion; Sit-and-Reach | BMI STG
|
| Barbosa et al. ( | RCT | ≥60; M-100% | 20/20/20 | 4 | SUTG and UTG:12 × 3 × 30 min/week | STG: experienced trainers | SUTG: 100% | SUTG: Metronome (30 reps/min) | I: IPAQ - SF | W10 m SUTG
|
| Chow et al. ( | non-RCT | 66 ± 4.3; M-37.9% | 29 | 7 | aerobic Training: 0–12 weeks, 5 × 40 min/week | Coach | NR | Moderate (measures NR) | II: 2 min step test; 30s Chair stand test; handgrip strength test; Rom berg test, Single-leg stance test, 8-Foot Up- and-Go; ROM, Back Scratch | 2 min step |
| Johnson et al. ( | non-RCT | 41.2 ± 6.5; M-66.7% | 6 | 6 | 6 × 2 × 2/3/4 circuit/week | instructor | 100% | Self-selected | I: Steps | steps |
| Kim et al. ( | RCT | 73.2; M-8.57% | 10/12/13 | 5 | RTG: 6 × 3 × 50 min/week, | Researcher | RTG: 75% | moderate-vigorous (RPE 6–8) | II: 30 s chair stand, 30 s arm curl, 244 cm up and go, one-leg stand, and 2 min step; push-ups; six-min walk tests | push-up RTG
|
| Lee et al. ( | non-RCT | 75.63; M-17.4% | 46 | NR | NR | Researcher | 90.87% | Moderate (measures NR) | I: the fulfillment of the WHO PA recommendations; RAPA | balance |
| Leiros-Rodríguez et al. ( | RCT | 68.5; M-0% | 14/14 | 12 | 12 × 2 × 50 min/week, balance training based on 12 OFE | physical therapist | 66.7% | intermittent (60s Work / 60s Rest) | II: BBS, TUG | Berg Balance Scale |
| Liu et al. ( | RCT | 70; M-28.6% | 21/21 | 3 | 12 × 3 × 40-45 min, structure training | three certified athletic trainers | 100% | Aerobic: Metronome (120 bpm) | I: 2-min step test; back scratch; chair sit and reach tests; arm curl test; sit to stand test; timed up and go test | no significant improvement in all parameters |
| Levinger et al. ( | non-RCT | 72.8; M-18.7% | 80 | 22 | 18 × 2 × 45–75 min/week, structure training | 1–12 week: Accredited Exercise Physiologist or Physiotherapist 13–18 week: Unsupervised | 86% | Supervised Dynamic Adjustment | I: CHAMPS | physical activity (caloric expenditure, frequency per week, and total time) |
| Marcos-Pardo et al. ( | RCT | 50-77; M-35.9% | 64/64 | 8; | 8 × 2 × 60 min/week | Two sports scientists | 92.75% | Moderate (measures NR) | II: Body mass; MVIC elbow flexion test; MVIC leg extension | Lean mass index |
| Ng et al. ( | non-RCT | 77.8 ± 6.0; M-59% | 46 | 22 | 24 × 2 × 60 min/week, structure training | 1–18 week: physiotherapist (1:8) | 1–18 week: 90.9% | Supervised Dynamic Adjustment | I: PASE | physical activity |
| Nguyen et al. ( | non-RCT | 35.0 ± 9.0; M-0% | 6 | 6 | 6 × 3 × 60 min/week | researcher | 100% | Aerobic: Moderate (measures NR) | II: one-mile walk; push-up test, squat test, and curl-up test | muscular endurance repetitions |
| Plotnikoff et al. ( | Cluster RCT | 53.4 ± 13.9; M-28% | 123/122 | 8 Resistance and aerobic | 12 × 2 × 45-55 min/week | Unsupervised | 92% | Multi-level (Self-selected) | I: accelerometers; Godin Leisure-Time questionnaire; the Global Physical Activity Questionnaire | Self-reported total MET |
| Sales et al. ( | RCT | 71.4; M-29.0% | 21/27 | 16 | 16 × 2 × 45–75 min/week, structure training | accredited exercise physiologist | 79.6% | light to moderate | II: BOOMER; the single leg stance test, hand grip; 2-min walk test; 30-s sit-to-stand test; gait speed | single-leg stance |
| Study | Reporting | External validity | Internal validity—bias | Internal validity—confounding | Power | Total | Quality rating |
|---|---|---|---|---|---|---|---|
| 11 points | 3 points | 7 points | 6 points | 1 point | |||
| Baruki et al. ( | 9 | 1 | 7 | 6 | 1 | 24 | Good |
| Barbosa et al. ( | 9 | 1 | 6 | 6 | 1 | 23 | Good |
| Chow et al. ( | 9 | 1 | 5 | 4 | 1 | 20 | Good |
| Johnson et al. ( | 9 | 1 | 5 | 4 | 0 | 19 | Fair |
| Kim et al. ( | 9 | 1 | 6 | 5 | 1 | 22 | Good |
| Lee and Ho ( | 8 | 1 | 5 | 4 | 1 | 19 | Fair |
| Leiros-Rodríguez and García-Soidan ( | 9 | 1 | 5 | 5 | 1 | 21 | Good |
| Levinger et al. ( | 9 | 1 | 5 | 4 | 1 | 20 | Good |
| Liu et al. ( | 9 | 1 | 7 | 6 | 1 | 24 | Good |
| Ng et al. ( | 9 | 1 | 5 | 4 | 1 | 20 | Good |
| Nguyen and Raney ( | 9 | 1 | 5 | 4 | 0 | 19 | Fair |
| Plotnikoff et al. ( | 9 | 1 | 5 | 5 | 1 | 21 | Good |
| Marcos-Pardo et al. ( | 9 | 1 | 6 | 6 | 1 | 23 | Good |
| Sales et al. ( | 9 | 1 | 7 | 6 | 1 | 24 | Good |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTherapeutic Uses of Natural Elements · Outdoor and Experiential Education · Urban Green Space and Health
Introduction
1
Physical inactivity is a worldwide issue with significant health and social risks (1, 2). It causes 6–10% of non-communicable disease-related deaths (2) and higher percentages of specific illnesses (e.g., 27% of diabetes) (3). The considerable incidence of physical inactivity significantly increased the government’s financial burden, and it was reported that physical inactivity caused a $67.5 billion economic loss in 2013 (1). Considering this dire situation, the “Global Action Plan on Physical Activity 2018–2030: More Active People for a Healthier World,” which was aimed at active societies, active environments, active people, and active systems, was launched by the World Health Organization (WHO) (4). It was suggested that infrastructure, policy, advocacy, and surveillance were crucial for realizing the plan’s objectives outlined above (5, 6). Among the suggestions, facilities for physical activity were studied as the most effective strategy to combat physical inactivity at the population level (7). Therefore, accelerating infrastructure is a reasonable and feasible solution to addressing this issue.
Outdoor fitness equipment (OFE) is an accessible environmental infrastructure constructed in open spaces, providing free opportunities for structured physical activity. It consists of simple, durable exercise machines or stations designed to provide organized physical activity (8–10). Historically, the origins of modern OFE can be attributed to the innovative ideas of Swiss architect Erwin Weckerman in the 1960s, whose visionary approach involved incorporating simple fitness equipment into walking paths, serving as a prototype for future OFE advancements. With the increasing awareness of fitness and the urgent need for space optimization, the variability of OFE is expanding. Some were designed for a specific population (e.g., the older adult) to meet the complex demands (11). Some were combined with other facilities (e.g., walkways) to increase the diversity and intensity of physical activity (12). Thus, various terminologies are used to describe OFE, including “open gyms” (13), “golden age gym” (14), and “fitness zones” (15). For consistency, the term “outdoor fitness equipment” and the abbreviation “OFE” will be utilized throughout the text.
Early examples of research into OFE aimed to investigate its promotion of physical activity, and some utilized observational methods. The findings indicate that exercise time on moderate-to-vigorous physical activity increased after installing OFE (9, 16). Nowadays, OFE has become prevalent globally, with installations in countries including Australia (17), the United States (16), Colombia (18), and China (8). Due to the popularity and diversity of OFE, the focus of OFE research engaged in more dimensions to evaluate the efficacy of qualitative studies, such as physical fitness, psychological well-being, and other health-related outcomes. For instance, Sales et al. employed interview methods to assess the impact of OFE intervention on individuals’ health outcomes (19). The research outcomes exhibited positive effects of the intervention on the participant’s muscle strength, balance, flexibility, confidence, and social interaction. Given its wide range of health benefits, OFE is recognized by society as a health intervention.
With the growing number of studies investigating the effects of OFE, several reviews have been conducted to summarize its impacts. Initially, most studies utilized qualitative research methods, leading to an integrative synthesis in previous reviews. Lee et al. synthesized evidence from quantitative, qualitative, and mixed methods studies and found that pursuing health and socialization opportunities was the primary motivation for using OFE (20). Meanwhile, Jansson et al. noted that while OFE may enhance physical activity, fitness, and other health-related outcomes, there was a lack of experimental studies supporting these findings (21). As more randomized controlled trials (RCTs) were conducted, meta-analyses emerged to assess the effects of OFE quantitatively. Ng et al. performed a mixed-methods meta-analysis to examine the impact of OFE on health outcomes in older adults (22). The results indicated that OFE did not improve physical performance, and whether OFE effectively increased physical activity remained inconclusive. While some evidence suggests a positive influence on specific health outcomes, several unanswered questions remain.
Researchers have not treated OFE in much detail, which might be the reason for the inconclusiveness. Firstly, previous reviews included various types of studies (prospective, cross-sectional, qualitative, pre-post, and RCTs) and lacked quantitative data, making it challenging to draw clear conclusions due to the complexity of OFE. Secondly, the heterogeneity of study types has led most existing reviews to favor systematic reviews and integrative synthesis over meta-analyses, which typically provide stronger evidence. Thirdly, the limited number of RCTs has hindered comprehensive meta-analyses, as only two were included in the existing meta-analysis. Given the limitations mentioned above, and to compensate for the lack of RCTs in the meta-analysis conducted by Ng, this research provided a comprehensive screening and analysis of OFE-related quantitative studies. It was significant in discovering the effectiveness of OFE on health outcomes.
Therefore, the primary objective of this systematic review was to assess the impact of OFE intervention on various aspects of health. These include physical activity (i.e., changes in physical activity levels before and after OFE intervention), physical fitness (i.e., indicators of strength, balance, and cardiorespiratory fitness measured through tests), psychological health (i.e., indicators of depression, loneliness, and anxiety measured using scales), health-related issues (i.e., any health outcome such as diabetes, hypertension, falls risk, and quality of life). We aim to address these critical questions through a rigorous and structured analysis: Do OFE intervention effectively promote physical activity? Can they lead to significant improvements in health and well-being?
Materials and methods
2
This systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (23) and was registered in the International Prospective Register of Systematic Reviews (Prospero registration: CRD42023449759).
Search strategy
2.1
We searched five online databases (Web of Science, Scopus, PubMed, Embase, and the Cochrane Library) from inception to May 24, 2024, with an updated search conducted on November 3, 2025. In addition, a manual search of the reference lists of included studies, relevant systematic reviews, and meta-analyses was performed to identify additional eligible studies. Search terms included a combination of keywords associated with OFE (e.g., outdoor gym, fitness zone, open gym, stretch station, public fitness facility, older adult fitness corner, senior exercise park, active park) and outcomes (e.g., effect, impact, assess, measure). The entire search strategy is available in Supplementary file 1.
Eligibility criteria
2.2
Inclusion criteria:
Participants: No restrictions.
Interventions: Interventions delivered through OFE (i.e., OFE installed in outdoor community parks or Seniors Exercise Park) that aim to improve health outcomes (e.g., physical fitness and/or psychological well-being and/or health-related outcomes).
Comparison: The comparator groups were strictly defined as ‘treatment as usual’, ‘wait-listed’, or non-active controls. Participants in these groups were instructed to maintain their habitual lifestyle and did not engage in any structured physical activity or exercise. Importantly, these groups did not receive any generic physical activity advice or educational materials during the intervention period.
Outcome: Outcomes included physical activity levels with objective measures (e.g., accelerometers, step counters) or subjective assessments (e.g., the Physical Activity Scale for the Elderly Questionnaire), physical fitness (e.g., balance, strength, mobility, and endurance), psychological health (e.g., depression, loneliness, and anxiety), and health-related issues (e.g., hypertension, hypoglycemia, falls risk, and quality of life). Studies were excluded if they did not report at least one of these outcome measures.
Study Design: RCTs and non-randomized controlled trials (non-RCTs) were included.
Exclusion criteria: Studies will be excluded if they meet the following criteria: unable to extract study data; a review, study protocol, case study, or conference paper; the OFE intervention group included other confounding factors such as medications; The comparison group involved some form of physical activity or exercise; non-English language studies.
Study selection and data extraction
2.3
We utilized Endnote X9 software to remove duplicates from the retrieved literature. After removing duplicates, two reviewers independently screened each article (ZY. T. and YQ. J.) for the title and abstract. Full-text versions of the remaining articles were assessed for eligibility after removing irrelevant studies.
Two reviewers (ZY. T. and YQ. J.) independently extracted data using a predesigned extraction form. Data extraction included: Basic literature details (first author name, publication year, country, and study design); participant characteristics (mean age, sex, sample population, and sample size); Characteristics of the OFE (terminology, locations, No. of OFE, and type of exercise); intervention components (type, session time, frequency, duration, outcome measured); significant findings (physical activity and/or physical fitness and/or psychological health and/or health-related issues). Disagreements were resolved by consensus or by a third reviewer (YS. Z.) at each stage of the screening process.
Risk of bias assessment
2.4
Two reviewers (ZY. T. and HB. X.) independently assessed the methodological quality of the included studies based on a modified Downs and Black checklist. The checklist demonstrated high test–retest and good inter-rater reliability for assessing the methodological quality of RCTs and non-RCTs (24, 25). Consistent with previous systematic reviews, the modified checklist consists of 27 items divided into five subscales: reporting (10 items), external validity (3 items), internal validity-bias (7 items), internal validity confounding (6 items), and statistical power (1 item) (26, 27). The checklist scores range from 0 to 28. The methodological quality of a study was classified into four levels: poor quality with a score ≤ 14; fair quality if it scored 15–19; good quality if it scored 20–25; and excellent quality if it scored 26–28 (28). Discrepancies between reviewers about the methodological quality of the included studies were resolved by a third reviewer (YS. Z.).
Data analysis
2.5
Among the inclusion, non-RCTs compared baseline and post-intervention outcomes, and RCTs compared the difference in value of pre- and post-intervention results between intervention and control groups. Data analysis was conducted using Stata 14.0 software (Stata, Texas, United States). The included data were continuous variables and effect sizes (ESs) were calculated using the standardized mean difference (SMD) with 95% confidence intervals (CI). In cases with insufficient data for meta-analyses, the magnitude of ESs was calculated using Hedges’ g (29, 30). Effect thresholds were defined as follows: 0.2, 0.5, and 0.8, representing small, medium, and large effects, respectively (31). Heterogeneity was assessed using the p-value (with a threshold of 0.1) and the I2 statistic (with points of 25, 50, and 75% representing small, medium, and large ratios of inter-study heterogeneity) (32). The fixed-effect model was applied if no statistical heterogeneity was found across studies (I^2^ ≤ 50%, p > 0.1). Otherwise, the random-effects model was utilized (33). Publication bias (e.g., Egger’s regression test) was not performed because fewer than 10 studies were included in each analysis. Sensitivity analysis was performed by excluding individual studies one by one using Stata 14.0 software. In addition, for a study that included two interventions that were distinguished by a and b.
Evidence certainty assessment
2.6
The quality of evidence for each outcome was assessed by two independent researchers (HB. X. and YQ. J.) using the Grading Recommendations to Assess Development and Evaluation System (GRADE), an internationally recognized standard for evaluating evidence quality and classifying recommendation strength (34). The quality of evidence is categorized into four levels: I (high), II (moderate), III (low), and IV (very low). Several factors can decrease evidence quality, including the risk of bias, imprecision, inconsistency, indirectness, and publication bias. Conversely, evidence quality can be increased by factors such as effect size, dose–response gradient, and control of confounding variables. For more information, please refer to Supplementary file 2.
Results
3
Literature search results
3.1
A total of 6,467 articles were identified from five databases (Web of Science: 1,323; Scopus: 3,953; PubMed: 446; Embase: 696; Cochrane Library: 49) in the initial search. After 1,058 duplicate articles were removed, 5,409 were screened by titles and abstracts. Subsequently, 93 articles were retrieved through full-text screening, of which 14 were eligible for inclusion. Finally, the systematic review included 14 articles, while the meta-analysis included 11 (35–45). Among the studies included in the meta-analysis, three non-RCTs conducted a single-arm meta-analysis (46–48). The screening process of the study is shown in Figure 1.
PRISMA flow diagram of the selection.
Description of included studies
3.2
All included studies are quantitative study with eight RCTs and six non-RCTs, the characteristics of the included literature is shown in Table 1. Four studies were conducted in Australia (40, 43–45), three in China (37, 41, 47), and the remains were from Brazil (35, 36), Sweden (46), Korea (38), Spain (39, 42), and the United States (48). Two-thirds of the studies were conducted within the past 5 years. A total of 828 participants were included, comprising 615 in the RCTs and 213 in the non-RCTs. The sample size ranged from 6 to 245, with participants aged 40 to 83. Specially, 32.6% of the participants were male.
Most OFE investigated were in public parks, and a few were in community open spaces. Given the significant variation in naming conventions across the literature, a detailed glossary listing the specific terminology (e.g., ‘fitness zones’, ‘seniors exercise parks’) and locations for each included study is provided in Supplementary file 3. Existing OFE can be categorized into several types of equipment that target various aspects of physical fitness. To provide a clearer overview of the interventions, a detailed classification of the specific equipment used in each study, including their targeted functions, adjustability, and progression features, is presented in Supplementary file 4. Cardio equipment, such as air walkers and ski machines, aim to improve cardiorespiratory fitness. Resistance equipment, such as rowing machines and Bonny riders, focuses on increasing muscular strength. Flexibility equipment, including arm stretches and shoulder wheels, promotes flexibility. Balancing equipment, such as waist twists, jumping boxes, and balance beams, seeks to enhance balance. Lastly, core equipment, such as push-up and pull-up bars, work on core skills. It is important to note that each type of equipment serves a specific purpose in overall health. OFE mentioned above has several limitations. One major limitation is the inability to adjust the equipment to fit the individual user’s needs, body shape, or size. Another limitation is the inability to modify the resistance level, which affects the ability to alter the intensity of the workout.
The interventions in this study targeted specific functions (e.g., cardiorespiratory training, balance training, aerobic training) or comprehensive functions (i.e., containing a variety of physical fitness). The frequency of interventions ranged from 2 to 3 times/week, with sessions lasting from 45 to 75 min and duration ranging from 6 to 24 weeks. Certain studies examined intervention intensity, measuring heart rate or ratings of perceived exertion (RPE) scales.
The efficacy of OFE interventions is assessed in various ways. Physical activity is generally measured with scales such as the Physical Activity Scale for the elderly questionnaire and the Physical Activity Rapid Assessment Scale. Physical fitness is assessed with functional tests such as grip strength, 30-s arm flexion, 30-s sit-to-stand, 2-min walking, one-legged standing, and Romberg test. Psychological health is evaluated with scales such as the General Mental Health Questionnaire, the Loneliness Scale, the Geriatric Depression Assessment Scale, and the Exercise Self-Efficacy Scale. Health-related issues are assessed with scales such as the Falls Risk for Older People in the community and the 36-Item Short Form Health Survey.
Assessment of study quality
3.3
The methodological quality of the included articles was assessed by the Downs and Black checklist, as presented in Table 2 and additional information in Supplementary file 5. Scores range from 19 to 24, with most articles rated as good (11/14, 78.6%) and three as fair (3/14, 21.4%). For the subscales, most of the articles met the reporting requirements (9/11 points), while external validity (1/3 points), bias (5.6/7 points), and confounding (4.9/6 points) were more or less problematic. Twelve (12/14, 85%) articles reported power analyses. The primary issues identified were the absence of randomization and blinding procedure information.
Health outcomes
3.4
Physical activity
3.4.1
A total of five studies assessed the impact of OFE interventions on physical activity. Regarding outcomes derived from self-reported measures, three studies consistently demonstrated positive effects. Lee et al. observed a significant increase in the proportion of participants meeting WHO physical activity recommendations following the intervention (47). Similarly, Levinger et al. reported significant improvements in caloric expenditure, exercise frequency, and total exercise time using the CHAMPS questionnaire (40). Ng et al. also found a significant increase in physical activity levels assessed by the PASE questionnaire after an 18-week intervention, which was sustained at the 24-week follow-up (43).
By contrast, evidence from device-based measures employed in two studies yielded mixed findings. Johnson et al. utilized pedometers and identified a significant increase in daily step counts following a 6-week outdoor gym circuit program (46). However, Plotnikoff et al., employing accelerometers in a cluster RCT, did not observe significant changes in moderate-to-vigorous physical activity levels between the intervention and control groups (44). This discrepancy between measurement methods suggests that self-reported assessments may potentially overestimate the intervention’s impact on overall activity levels compared to objective monitoring.
Physical fitness
3.4.2
Cardiorespiratory fitness
3.4.2.1
The cardiorespiratory fitness results contained four RCTs (36, 38, 41, 45), including six pairwise comparisons. Meta-analysis results indicated that OFE intervention was effective in improving cardiorespiratory fitness compared to controls (SMD = 0.53; 95% CI (0.25 to 0.82); p < 0.001; Figure 2). No significant heterogeneity was observed in the meta-analysis results (I^2^ = 0.1%, p = 0.415). In addition, three non-RCTs (37, 40, 46) reported that OFE intervention significantly improved cardiorespiratory fitness.
The effect of OFE intervention on cardiorespiratory fitness.
Lower limb muscle strength
3.4.2.2
The lower limb muscle strength results contained seven RCTs (35, 36, 38, 41, 42, 44, 45), including 10 pairwise comparisons. Meta-analysis results indicated that OFE intervention was effective in improving lower limb muscle strength compared to controls (SMD = 0.35; 95% CI (0.19 to 0.50); p = 0.001; Figure 3). No heterogeneity was observed in the meta-analysis results (I^2^ = 13.1%, p = 0.323). In addition, five non-RCTs (37, 40, 43, 46, 48) reported that OFE interventions significantly improved lower limb muscle strength.
The effect of OFE intervention on lower limb muscle strength.
Upper limb muscle strength
3.4.2.3
The upper limb muscle strength results contained five RCTs (36, 38, 41, 44, 45), including seven pairwise comparisons. Meta-analysis results indicated that OFE intervention was effective in improving upper limb muscle strength compared to controls (SMD = 0.25; 95% CI (0.06 to 0.44); p = 0.009; Figure 4). Small heterogeneity was observed in the meta-analysis results (I^2^ = 34.7%, p = 0.163). In addition, two non-RCTs (46, 48) reported that OFE intervention significantly improved upper limb muscle strength.
The effect of OFE intervention on upper limb muscle strength.
Balance
3.4.2.4
The balance results contained four RCTs (38, 39, 41, 45), including five pairwise comparisons. Meta-analysis results indicated that OFE intervention improved balance more effectively than controls (SMD = 0.83; 95% CI (0.11 to 1.55); p = 0.024; Figure 5). Significant heterogeneity was observed in meta-analysis results (I^2^ = 77.8%, p = 0.001). Subgroup analyses were conducted to identify heterogeneity sources (Supplementary Figure 1). The subgroup analysis indicated that the choice of measurement tools significantly influenced the effect of OFE intervention. The different measurement tools might be the source of heterogeneity. In addition, three non-RCTs (37, 43, 47) demonstrated that OFE interventions significantly improved balance.
The effect of OFE intervention on balance.
Psychological health
3.4.3
Mental well-being
3.4.3.1
The mental well-being results contained two non-RCTs (40, 43). Meta-analysis results indicated that OFE intervention was effective in improving mental well-being compared to controls (SMD = 0.48; 95% CI (0.21 to 0.74); p < 0.001; Figure 6). No heterogeneity was observed in the meta-analysis results (I^2^ = 0.0%, p = 0.680).
The effect of OFE intervention on mental well-being.
Loneliness
3.4.3.2
The loneliness results contained two non-RCTs (40, 43). Meta-analysis results indicated that OFE intervention was effective in improving loneliness compared to controls (SMD = 0.33; 95% CI (0.07 to 0.58); p = 0.014; Figure 7). No heterogeneity was observed in the meta-analysis results (I^2^ = 0.0%, p = 0.436).
The effect of OFE intervention on loneliness.
Four non-RCTs (40, 43, 44, 47) examined the effect of OFE intervention on individual self-efficacy. Of those, three studies reported that OFE interventions significantly improved self-efficacy in individuals. In contrast, one study reported that OFE interventions did not improve the individuals’ self-efficacy. In addition, three studies reported that OFE interventions significantly improved depression, stress symptoms, autonomous motivation, and enjoyment in individuals.
Health-related issues
3.4.4
Quality of life
3.4.4.1
Quality of life results contained two RCTs (36, 39), including three pairwise comparisons. Meta-analysis results indicated that OFE intervention improved quality of life more effectively than controls (SMD = 1.06; 95% CI (0.26 to 1.86); p = 0.010; Figure 8). Significant heterogeneity was observed in meta-analysis results (I^2^ = 69.9%, p = 0.036). Subgroup analyses were conducted to identify heterogeneity sources (Supplementary Figure 2). The subgroup analysis indicated that the choice of measurement tools significantly influenced the effect of OFE intervention. The different measurement tools might be the source of heterogeneity. In addition, two non-RCTs (40, 43) reported that OFE interventions significantly improved the quality of life.
The effect of OFE intervention on quality of life.
Falls risk
3.4.4.2
The fear of falls results contained two non-RCTs (40, 43). Meta-analysis results indicated that OFE intervention was effective in improving fear of falls compared to controls (SMD = 1.01; 95% CI (0.41 to 1.61); p = 0.001; Figure 9). Significant heterogeneity was observed in meta-analysis results (I^2^ = 74.8%, p = 0.046). The results include only two trials that were not analyzed in subgroups, so the reasons for the heterogeneity remain unknown.
The effect of OFE intervention on falls risk.
In addition, some studies have found that OFE interventions can positively affect hypertension, hypoglycemia, and blood lipid levels (38, 47).
GRADE quality evaluation
3.5
The GRADE evidence profile for RCT outcomes is presented in Supplementary file 6. Evidence quality ranges from moderate to high. Specifically, there is high evidence that OFE intervention significantly affects cardiorespiratory fitness and balance. In addition, there is moderate evidence that OFE intervention significantly affects lower limb muscle strength, upper limb muscle strength, and quality of life.
Sensitive analysis
3.6
To test the results’ stability and whether the heterogeneity is due to a single study. We used the one-to-one exclusion method for studies with high heterogeneity to analyze the combined effect sizes. Sensitivity analyses indicated that no single research influenced the combined effect estimate, affirming the robustness of our findings. For specific information, refer to Supplementary Figures 3–5.
Discussion
4
The current study aims to examine the effectiveness of OFE intervention on overall health. OFE interventions appear to positively affect physical activity, physical health, mental health, and health-related outcomes as assessed by validated measures.
Participant
4.1
It was found that users of OFE exhibit a distinctive age distribution. The subjects in previous research were exclusively middle-aged and older adults, ranging in age from 40 to 83, with a majority being older adult. OFE is typically uncomplicated in structure, adaptable in form, easy to use, and economical. It is likely due to such qualities that OFE has been widely embraced as a workout option for older adults. According to the World Health Organization, the global population of individuals aged 60 and above is expected to reach 2.1 billion by 2050 (49). Population aging and age imbalances will become significant global social issues. Given the rapid growth of aging populations, international experience indicates a transition in health management from a biomedical paradigm focused on disease treatment to a preventive medicine model emphasizing proactive intervention. As individuals age, vital bodily functions gradually deteriorate in motor, cognitive, and sensory capacities (50). As a result, a wide range of chronic diseases associated with aging arise. Therefore, establishing a health-focused exercise setting is critical to advancing healthy aging. This meta-analysis revealed that interventions based on OFE could considerably enhance physical performance, mental well-being, and quality of life. OFE was proved to be an efficient approach for cultivating healthy habits among older adults.
Physical activity
4.2
The benefits of OFE can be seen in increased physical activity time and considerably higher physical activity levels. Lee et al. employed a scale to evaluate the degree to which participants met WHO’s physical activity recommendation standards after OFE intervention (47). The results revealed a noteworthy rise in the number of participants who achieved the standards after the intervention. In addition, various studies have utilized the System for Observing Play and Recreation in Communities to assess the impact of installing OFE into parks on the population’s physical activity levels (16, 51). The findings demonstrated that combining OFE resulted in a rise in total METs compared to the baseline levels among park users. Moreover, there was a marked increase in moderate to vigorous intensity physical activity, coupled with a significant decrease in sedentary behavior (15). However, many physical activity measures presently used depend on self-reports or scales. These are likely to overestimate physical activity levels when contrasted to objectively measured levels. More significantly, OFE interventions also promote exercise habits and healthy lifestyles. The study revealed that 6 and 9 months after OFE intervention, participants’ physical activity remained significantly higher than baseline and exceeded the WHO recommendation of 150 min of moderate-intensity physical activity per week (47). Evidence indicates that individuals who participate in outdoor physical activity may be more compliant with regular exercise habits (52). In addition, it has been demonstrated that engaging in outdoor activities within green or natural environments can enhance the personal sense of vitality and active participation (53). Subsequently, OFE interventions can encourage individual physical activity and develop long-term healthy habits.
Physical fitness
4.3
The meta-analysis results demonstrate that OFE intervention has a small positive effect on upper limb muscle strength (SMD = 0.25) and lower limb muscle strength (SMD = 0.35), moderate positive effect on cardiorespiratory fitness (SMD = 0.53), and large positive effect on balance (SMD = 0.83). This finding contradicts previous meta-analyses, which concluded that OFE did not improve physical health (22). This may be due to the fact that the previous study limited the number of studies it analyzed, only calculating effect sizes for two. There were substantial differences between these two studies regarding session length, total duration, and exercise load. Moreover, the number of OFEs utilized and how outcome indicators were measured were inconsistent. Compared to prior research, the current meta-analysis expanded the number of studies analyzed and categorized them based on distinct aspects of physical health. The surveyed literature consists solely of high-quality randomized controlled trials, thereby strengthening the credibility and persuasiveness of the findings in this study. In addition, we also found that the OFE intervention was most effective in improving balance. OFE is often designed to promote functional training, which involves the coordinated use of different body parts (54). This integrated training method can be used to practice activities of daily living such as walking, standing, and turning. Therefore, balance and coordination skills may be challenged more often for people using OFE, contributing to improvements in balance skills. Cardiorespiratory fitness and muscular strength also improved but may have been influenced by the type and intensity of exercise, which was not as pronounced in the OFE intervention. More research may be needed to gain specific insights into the exact impact of OFE on these health outcomes.
Psychological health
4.4
This review indicates that OFE interventions have a beneficial impact on mental well-being. The OFE interventions positively affect mental health indicators, such as mental well-being, depression, stress symptoms, self-efficacy, and enjoyment. The meta-analysis results reveal that OFE interventions have a slight but positive effect on mental well-being (SMD = 0.48). The possible reason is that exercise modifies brain-derived neurotrophic factor (BDNF) levels, which can lead to improved mental health and brain plasticity (55). Furthermore, exercise forward endorphins release, which has been shown to alleviate symptoms of depression and anxiety (56, 57). Consistent with these findings, the present study revealed that the OFE intervention positively affected depression. Since exercising in a green or natural environment was proven to improve negative emotions in numerous studies, such as tension, anger, and depression (58), the placement of OFE in such settings may offer added value (59). As a result, stress symptoms of the OFE intervention are significantly reduced while both self-efficacy and enjoyment increased. Meanwhile, studies investigating the effects of natural environments on stress-related brain mechanisms suggest that exposure to nature can decrease amygdala activity (60). This suggests that the outdoor setting of OFE might act synergistically with physical exertion to enhance individuals’ mental health (61). The multiple merits of OFE intervention for personal mental health make it a powerful adjunct to mental health prevention.
At the same time, the OFE interventions improve psychosocial well-being, including reducing loneliness and enhancing interpersonal and communicative interactions. The meta-analysis results show a small positive effect of the OFE intervention on Loneliness (SMD = 0.33). This can be attributed to the fact that the OFE intervention increases opportunities for social engagement and the provision of social support. Previous studies confirmed that social support was significantly negatively correlated with loneliness (62, 63). And people with high self-efficacy received more social support and recognition (64). The evidence presented provides a potential explanation for why OFE interventions may reduce feelings of loneliness. Overall, OFE offers a green space for residents to exercise, promoting mental relaxation and stress relief and a daily space for socialization to enhance social interactions and improve residents’ quality of life and well-being.
Health-related issues
4.5
The meta-analysis results show that the OFE intervention has a large positive effect on fear of falls (SMD = 1.01). Falls have emerged as a prevalent health issue among seniors across the globe, according to the WHO. Every year, roughly 20–35% of people aged 62 and above suffer from falling incidents, and over 50% of these cases lead to injuries such as fractures, bleeding, and even death (65). Falls seriously impact patients’ physical and mental health and increase the healthcare burden on society. Healthcare expenditures increase with the frequency and severity of fall-related injuries (66). Falls risk factors include loss of balance, decreased muscle strength, and unsteady gait caused by reduced neurological control, which are primary triggers among older adults. Walking is the primary form of exercise for older adults, but it is ineffective in improving balance and strength and preventing falls. Combined exercise improved balance and muscle strength in older adults (67). This study’s results align with this finding. OFE interventions offer structured exercises that include various forms of exercise via diverse equipment, resulting in notable advancements in balance (SMD = 0.83) and lower body strength (SMD = 0.35). In this way, the OFE intervention can assist in preventing falls among older adults and promoting healthy aging.
The meta-analysis results indicate that the OFE intervention positively affects blood pressure, blood sugar, and lipids. There is substantial evidence showing that aerobic exercise may decrease blood pressure (68) and blood glucose levels (69), improve blood lipid profile (70), and lower the incidence of various diseases. Moreover, a study by the American Medical Association study found that moderate-intensity aerobic exercise has a practical antihypertensive effect with a maximum safety margin (71). It is more effective than low-intensity and vigorous-intensity exercise in preventing and reducing blood pressure. Studies, including this one, have found that the OFE intervention mainly involves moderate-intensity physical activity. Chow et al. employed a portable metabolic system to quantify the intensity of physical activity in older adults who used OFE (72). The range of metabolic equivalents for the air walkers was 2.81 to 3.55 METs, while the range for the ski machine was 3.02 to 4.05 METs. Studies have also measured metabolic equivalents, heart rate, and oxygen uptake during aerobic combined with resistance exercise with OFE. Results indicate that during bodyweight exercise, subjects had a mean metabolic equivalent of 4.6 METs, a mean heart rate of 64.1% of their maximum heart rate, and a mean oxygen uptake of 51.5% (73). Thus, the effectiveness of the OFE intervention in preventing and reducing blood pressure cannot be ignored.
Study limitations
4.6
This systematic review substantiates the effectiveness of OFE intervention on health outcomes but has several limitations. Firstly, the strength of the evidence is constrained by methodological limitations. Some included studies were non-RCTs, and nine RCTs contained a high or unclear risk of bias in certain domains. Furthermore, due to the limited number of studies included for each outcome (n < 10), we could not reliably assess publication bias using funnel plots or Egger’s tests. Consequently, the potential for small-study effects cannot be ruled out, and the reported aggregate effect sizes might be subject to overestimation. Secondly, the predominance of older female participants and the reliance on aggregated data from mixed-sex cohorts prevented the execution of stratified analyses by age or sex. Consequently, it is imperative to exercise caution when generalizing these findings to male populations or younger adults. Thirdly, using multiple assessment tools for a single outcome indicator in studies may lead to potentially bias effect size estimations, which complicate result interpretation in meta-analysis. Fourthly, the diversity of OFE results in various intervention program designs, making subgroup analyses and meta-regressions difficult, which do not allow for synthesizing specific exercise recommendations. Finally, due to the wide variety of assessment tools used across the included studies, it was not feasible to convert the standardized mean differences back to original units. Future research should prioritize standardized outcome measures to facilitate clearer clinical guidelines.
Conclusion
5
This systematic review and meta-analysis provide a comprehensive overview of the effectiveness of OFE intervention on health outcomes. The evidence indicates that OFE intervention effectively improves physical activity, physical fitness, psychological well-being, and other health-related results. However, due to the considerable variation in intervention characteristics and outcome measurements, it is not possible to determine which interventions are most beneficial. High-quality RCTs with well-reported OFE intervention characteristics are required to determine effective OFE exercise protocols and facilitate translation into practice.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ding D Lawson KD Kolbe-Alexander TL Finkelstein EA Katzmarzyk PT van Mechelen W . The economic burden of physical inactivity: a global analysis of major non-communicable diseases. Lancet. (2016) 388:1311–24. doi: 10.1016/S 0140-6736(16)30383-X, 27475266 · doi ↗ · pubmed ↗
- 2Lee I-M Shiroma EJ Lobelo F Puska P Blair SN Katzmarzyk PT. Effect of physical inactivity on major non-communicable diseases worldwide: an analysis of burden of disease and life expectancy. Lancet. (2012) 380:219–29. doi: 10.1016/S 0140-6736(12)61031-9, 22818936 PMC 3645500 · doi ↗ · pubmed ↗
- 3Organization WH. Global Health risks: Mortality and burden of disease attributable to selected major risks. Geneva: World Health Organization (2009).
- 4Organization WH. Global action plan on physical activity 2018–2030: More active people for a healthier world. Geneva: World Health Organization (2019).
- 5Hallal PC Andersen LB Bull FC Guthold R Haskell W Ekelund U. Global physical activity levels: surveillance Progress, pitfalls, and prospects. Lancet. (2012) 380:247–57. doi: 10.1016/S 0140-6736(12)60646-1, 22818937 · doi ↗ · pubmed ↗
- 6Kohl HW Craig CL Lambert EV Inoue S Alkandari JR Leetongin G . The pandemic of physical inactivity: global action for public health. Lancet. (2012) 380:294–305. doi: 10.1016/S 0140-6736(12)60898-8, 22818941 · doi ↗ · pubmed ↗
- 7Durão S Burns J Schmidt B-M Tumusiime D Hohlfeld A Pfadenhauer L . Infrastructure, policy and regulatory interventions to increase physical activity to prevent cardiovascular diseases and diabetes: a systematic review. BMC Public Health. (2023) 23:112. doi: 10.1186/s 12889-022-14841-y, 36647042 PMC 9841711 · doi ↗ · pubmed ↗
- 8Chow H-w. Outdoor fitness equipment in parks: a qualitative study from older adults’ perceptions. BMC Public Health. (2013) 13:1216. doi: 10.1186/1471-2458-13-1216, 24359536 PMC 3878060 · doi ↗ · pubmed ↗