Optimizing Treatment in Refractory Copper Deficiency: A Case Report
Bishara Jahshan, Rami B Moussa, Abdo Haddad

TL;DR
A woman with a history of gastric bypass surgery had treatment-resistant copper deficiency, which improved only after adjusting the IV copper administration frequency.
Contribution
Demonstrates that standard IV copper protocols may be insufficient for post-gastric bypass patients, suggesting the need for individualized treatment.
Findings
Standard IV copper regimen (2 mg daily for five days every four to six weeks) failed to correct copper deficiency over two years.
Increasing IV copper frequency to 2 mg twice weekly rapidly normalized copper levels.
Refractory copper deficiency in post-gastric bypass patients may require tailored treatment approaches.
Abstract
Copper deficiency, though rare, is increasingly observed in patients who have undergone Roux-en-Y gastric bypass due to impaired absorption in the stomach, proximal duodenum, and small intestine. Deficiency may manifest as anemia, cytopenias, and myeloneuropathy. Standard treatment includes oral or intravenous (IV) copper supplementation, with IV replacement preferred in cases of malabsorption. We present a case of treatment-resistant copper deficiency in a woman in her late forties with a history of Roux-en-Y gastric bypass and iron-deficiency anemia, who presented with lower extremity paresthesias. Laboratory evaluation revealed severe copper deficiency (serum copper: 10 µg/dL; normal 80-155 µg/dL). Despite oral supplementation and the standard IV copper regimen (2 mg daily for five days every four to six weeks) over a two-year period, her copper levels remained low. A revised…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
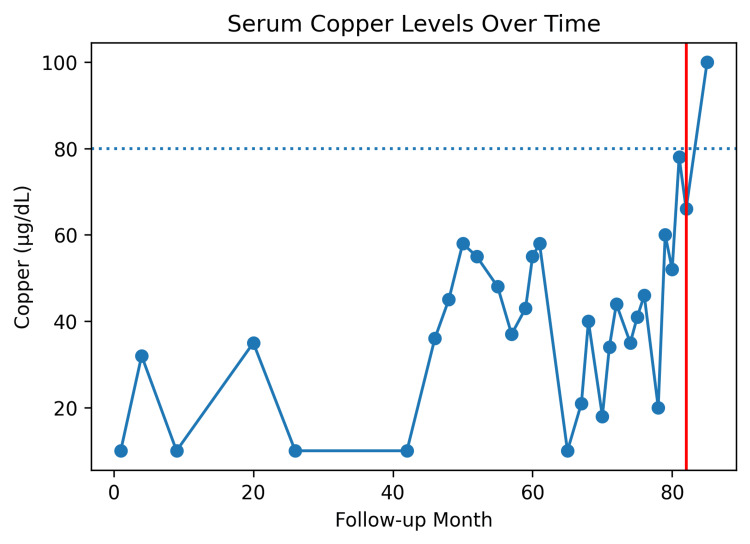 Figure 1
Figure 1| Follow-up Month | Copper (µg/dL) (Reference range: 80-155 µg/dL) |
| 1 | 10 |
| 4 | 32 |
| 9 | 10 |
| 20 | 35 |
| 26 | 10 |
| 42 | 10 |
| 46 | 36 |
| 48 | 45 |
| 50 | 58 |
| 52 | 55 |
| 55 | 48 |
| 57 | 37 |
| 59 | 43 |
| 60 | 55 |
| 61 | 58 |
| 65 | 10 |
| 67 | 21 |
| 68 | 40 |
| 70 | 18 |
| 71 | 34 |
| 72 | 44 |
| 74 | 35 |
| 75 | 41 |
| 76 | 46 |
| 78 | 20 |
| 79 | 60 |
| 80 | 52 |
| 81 | 78 |
| 82 | 66 |
| 85 | 100 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTrace Elements in Health · Gastrointestinal motility and disorders · Parathyroid Disorders and Treatments
Introduction
Although rare, copper deficiency has increased in prevalence. This is due to an increase in gastric bypass surgeries, which impacts the absorption of many vitamins and minerals [1]. The absorption of copper occurs in the stomach, proximal duodenum, and small intestine [2]. As a result, gastric bypass surgery is one of the leading causes of copper deficiency. Having copper deficiency negatively impacts the human body and can lead to myeloneuropathy, gait disorders, anemia, and other cytopenias [3]. Intravenous (IV) supplementation is the recommended treatment when malabsorption is the suspected cause of deficiency. The dosage is typically 1-2 mg of IV copper daily for the duration of five to six days [4].
Here, we describe a case of severe copper deficiency that posed therapeutic challenges, highlighting considerations for alternative IV copper supplementation strategies.
Case presentation
A woman in her late forties with a past medical history of hypertension, morbid obesity, obstructive sleep apnea, and systemic lupus erythematosus presented to the hematology clinic for iron-deficiency anemia.
She reported several months of paresthesias in her lower extremities without muscle weakness or ataxia. She had undergone Roux-en-Y gastric bypass five years prior and was managing iron-deficiency anemia with oral iron supplementation. She neither smoked nor used alcohol or illicit drugs.
During the physical examination, it was observed that the patient was obese. There was a slight reduction in sensation noted in her bilateral lower extremities. Her cranial nerves were intact. Her muscle strength was normal. She exhibited normal reflexes, coordination, and gait. Blood work demonstrated iron deficiency and a low copper level of 10 µg/dL (normal: 80-155 µg/dL).
She was initially treated with IV iron sucrose and oral copper citrate supplementation, providing 2 mg of elemental copper twice daily, was administered for three months. At three-month follow-up, her iron deficiency resolved, but copper levels remained low. A more aggressive copper replacement regimen was initiated, adding IV copper (2 mg daily for 5 days every four to six weeks) in addition to oral supplementation. Despite nearly five years on this regimen, her copper levels remained persistently low (see Table 1). Zinc, B12, and iron levels were monitored and repleted as needed.
Eventually, her regimen was changed to 2 mg IV twice weekly for three months, resulting in normalization of copper levels (see Figure 1). After achieving normal levels, the patient was transitioned to a once-weekly IV maintenance regimen.
Trend of serum copper levels over time.Serum copper concentrations are shown across follow-up months. The dotted horizontal line represents the lower limit of normal copper levels (80 µg/dL). The red vertical line at follow-up month 82 indicates initiation of twice-weekly intravenous copper replacement therapy.
Discussion
The recommended dietary allowance of elemental copper for adults is 900 μg per day [5]. Copper is abundant in nuts, organ meats, seeds, and seafood [6]. It is estimated that the incidence of copper deficiency in patients who undergo Roux-en-Y gastric bypass to reach 9.6% [7].
Standard management begins with oral supplementation. If oral therapy is ineffective, particularly with malabsorption, IV copper (2-4 mg/day for six days) is recommended [4]. Published case reports illustrate that copper deficiency often presents with cytopenias and neurologic deficits. These cases show rapid correction with copper replacement, though neurologic recovery is incomplete in some patients [8,9]. In contrast, our patient demonstrates a rare instance of persistent copper deficiency despite prolonged IV and oral supplementation over several years.
Several factors may contribute to treatment resistance, including altered absorption after bariatric surgery and interactions with other micronutrients. Excess zinc can impair copper absorption, making it a recognized cause of secondary copper deficiency [10]. Copper also plays a central role in iron metabolism, so iron and copper deficiencies often coexist [11]. In addition, copper deficiency may resemble or overlap with vitamin B12 deficiency, particularly neurologically, underscoring the need for coordinated monitoring [12,13]. In our case, zinc, iron, and vitamin B12 levels were regularly assessed and corrected throughout the patient’s course.
After years of standard replacement therapy, adjusting the intravenous copper regimen from 2 mg IV daily for five days to 2 mg IV twice-weekly dosing resulted in a significant improvement in persistent copper deficiency. This raises the possibility of more efficient copper repletion regimens in resistant cases.
Conclusions
This case highlights the importance of screening for copper deficiency in gastric bypass patients. What makes it particularly noteworthy is its resistance to standard copper replacement protocols. These observations suggest that adjusting the frequency of IV copper administration may improve the likelihood of achieving repletion and could represent a more effective approach in refractory cases. Individualized dosing schedules should therefore be considered when conventional treatment proves inadequate. These findings may pave the way for more personalized and effective treatment protocols.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Copper deficiency: a frequently overlooked complication after MBS - a systematic review and meta-analysis Obes Surg Xu B Xiao T Li J Lu Q Zhang Y Wan B Liang D 6026133520253975577210.1007/s 11695-024-07569-8 · doi ↗ · pubmed ↗
- 2Clinical manifestations of copper deficiency: a case report and review of the literature Nutr Clin Pract Moon N Aryan M Westerveld D Nathoo S Glover S Kamel AY 108010853620213303770110.1002/ncp.10582 · doi ↗ · pubmed ↗
- 3Copper deficiency in celiac disease J Clin Gastroenterol Halfdanarson TR Kumar N Hogan WJ Murray JA 1621644320091849623010.1097/MCG.0b 013e 3181354294 · doi ↗ · pubmed ↗
- 4Copper deficiency CMAJ Gallant RC Cameron L Mithoowani S 0197202510.1503/cmaj.250072 PMC 1204033440294944 · doi ↗ · pubmed ↗
- 5Nutrition information brief - copper Adv Nutr Burkhead JL Collins JF 6816831320223494082410.1093/advances/nmab 157PMC 8970836 · doi ↗ · pubmed ↗
- 6Copper: Fact sheet for health professionals. National Institutes of Health (NIH). U.S. Department of Health and Human Services 1 2026 3120252022 http://ods.od.nih.gov/factsheets/Copper-Health Professional/
- 7Incidence and prevalence of copper deficiency following roux-en-y gastric bypass surgery Int J Obes (Lond) Gletsu-Miller N Broderius M Frediani JK 3283353620122187654610.1038/ijo.2011.159PMC 3748601 · doi ↗ · pubmed ↗
- 8Acquired copper deficiency: a potentially serious and preventable complication following gastric bypass surgery Obesity (Silver Spring) Griffith DP Liff DA Ziegler TR Esper GJ Winton EF 8278311720091914811510.1038/oby.2008.614PMC 2712481 · doi ↗ · pubmed ↗