Epidemiology of drug–resistant tuberculosis in Hunan China over a 10–year period
Yi Liu, Jue Wang, Xiaojie Wan, Wang Peng, Jingwei Guo, Xi Yang, Di Zhou, Wenbin Li, Jie Duan, Xuan Zeng, Hua Bai, Zhenhua Chen, Fangzhen Luo, Yunhong Tan

TL;DR
This study analyzed 10 years of drug-resistant tuberculosis cases in Hunan, China, revealing high rates among middle-aged male farmers and regional differences in resistance types.
Contribution
The study provides the first 10-year epidemiological analysis of DR-TB in Hunan Province, identifying key demographic and regional risk factors.
Findings
INH-R TB and MDR-TB were the most common resistance subtypes in Hunan between 2014 and 2023.
Middle-aged and older male farmers were disproportionately affected by DR-TB.
Regional disparities were observed, with the western region having the highest risk for MDR-TB.
Abstract
Drug–resistant tuberculosis (DR–TB) remains a major public health challenge in China, yet long–term epidemiological data from key regions such as Hunan Province in South–Central China are still limited. This study aimed to characterize the epidemiological trends, spatial distribution, and risk factors of Single drug–resistant tuberculosis (SDR–TB), poly–drug–resistant tuberculosis (PDR–TB), multidrug–resistant tuberculosis (MDR–TB), rifampicin–resistant tuberculosis (RR–TB), and isoniazid–resistant tuberculosis (INH–R TB) in Hunan Province between 2014 and 2023, to inform region–specific control strategies. It was a retrospective analysis that was conducted on 6,597 laboratory–confirmed DR–TB cases. Data were obtained from the Provincial Tuberculosis Control Institute. All patients underwent phenotypic drug susceptibility testing. Independent risk factors for DR–TB subtypes were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
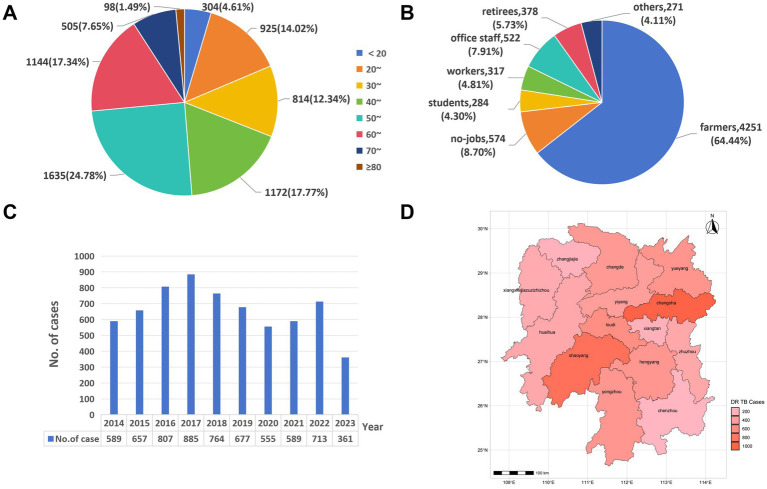 Figure 1
Figure 1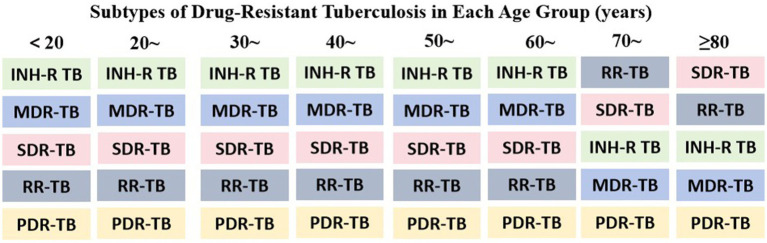 Figure 2
Figure 2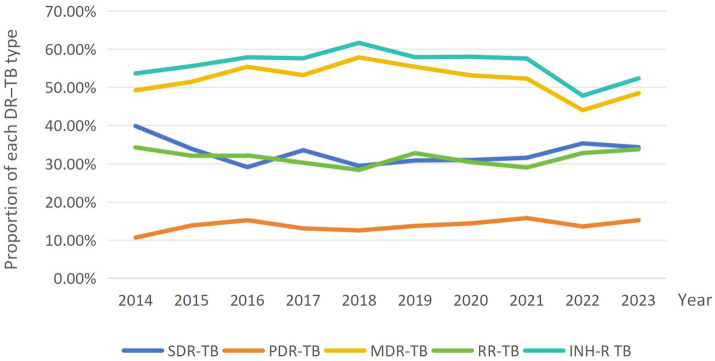 Figure 3
Figure 3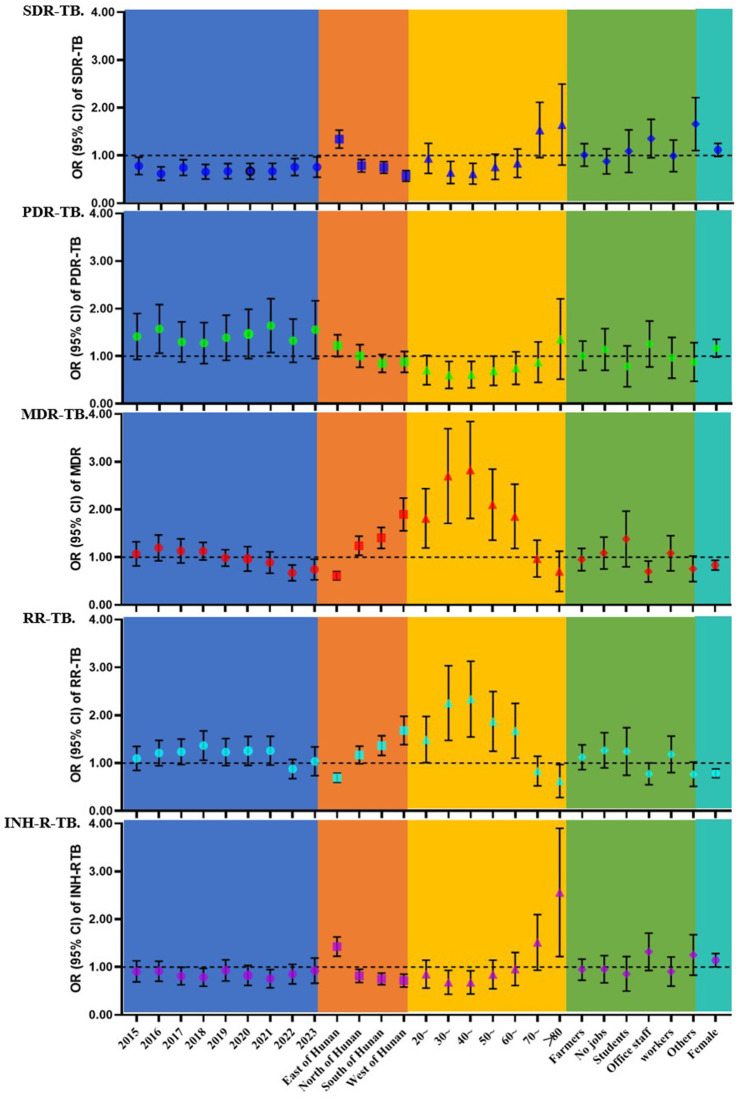 Figure 4
Figure 4| Subtypes | Yes ( | No ( | Proportion (95% CI) |
|---|---|---|---|
| SDR–TB | 2,158 (32.71) | 4,439 (67.29) | 32.71 (31.58–33.84) |
| PDR–TB | 907 (13.75) | 5,690 (86.25) | 13.75 (12.92–14.58) |
| MDR–TB | 3,455 (52.37) | 3,142 (47.63) | 52.37 (51.17–53.58) |
| RR–TB | 2076 (31.47) | 4,521 (68.53) | 31.47 (30.35–32.59) |
| INH–R TB | 3,712 (56.27) | 2,885 (43.73) | 56.27 (55.07–57.67) |
| Subtypes | No. of cases in each age group (years) | Total |
|
| |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| <20 | 20~ | 30~ | 40~ | 50~ | 60~ | 70~ | ≥80 | ||||
| SDR–TB | 111 | 335 | 228 | 310 | 504 | 376 | 244 | 50 | 2,158 | 109.656 | 0.000 |
| PDR–TB | 50 | 127 | 100 | 139 | 220 | 164 | 84 | 23 | 907 | 18.667 | 0.009 |
| MDR–TB | 136 | 456 | 476 | 711 | 894 | 590 | 168 | 24 | 3,455 | 163.308 | 0.000 |
| RR–TB | 97 | 291 | 219 | 304 | 498 | 381 | 277 | 40 | 2076 | 105.798 | 0.000 |
| INH–R TB | 144 | 488 | 505 | 758 | 961 | 641 | 188 | 27 | 3,712 | 170.558 | 0.000 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTuberculosis Research and Epidemiology · Diagnosis and treatment of tuberculosis · Malaria Research and Control
Introduction
Tuberculosis (TB) remains a leading cause of mortality from infectious diseases worldwide (1). The emergence and spread of Drug–resistant tuberculosis (DR–TB) have posed serious challenges to global TB control (2, 3). As one of the countries with the highest TB burden, China faces a particularly high prevalence of DR–TB, posing significant challenges to national TB control efforts (4). South–Central China, including Hunan Province, is characterized by a large population, substantial internal migration, and diverse socioeconomic conditions (5, 6). Although this region plays a critical role in national TB control, there is a lack of long–term systematic research on DR–TB in this area. A clear and comprehensive understanding of DR–TB trends and characteristics in this region is crucial for designing effective prevention and control strategies at regional and national levels.
The global incidence of DR–TB has increased, driven primarily by the widespread use of anti–TB drugs and inadequate adherence to treatment (7, 8). DR–TB can be classified into several resistance patterns (9). In this study, we focused on five major types: monoresistant tuberculosis (SDR–TB), poly–drug–resistant tuberculosis (PDR–TB), multidrug–resistant tuberculosis (MDR–TB), rifampicin–resistant tuberculosis (RR–TB), and isoniazid–resistant tuberculosis (INH–R TB). The management of DR–TB is prolonged and costly, with poorer treatment outcomes, placing substantial physical, psychological, and economic burdens on patients and creating major challenges for public health systems (10–12).
A clear understanding of the epidemiological characteristics, temporal trends in drug resistance, and related risk factors of DR–TB in South–Central China is vital for designing targeted interventions. To address this need, we conducted a 10–year retrospective analysis of DR–TB in the region to describe its epidemiology, assess temporal trends in drug resistance, and identify demographic and geographic risk factors.
Materials and methods
Data source
This study retrospectively analyzed data from patients diagnosed with TB at the Hunan Chest Hospital between January 1, 2014, and August 1, 2023. Located in South–Central China, the hospital is a provincial–level designated TB institute and clinical center. Demographic and clinical date–such as sex, age, occupation, place of residence, diagnostic results, and drug–susceptibility profiles–were extracted from the hospital’s information system. All personally identifiable data were anonymized prior to analysis to protect patient confidentiality.
Inclusion and exclusion criteria
Eligible patients were residents of Hunan Province and had a laboratory–confirmed diagnosis of DR–TB, established through drug susceptibility testing (DST). Patients with a history of repeated hospital admissions, incomplete medical records, or residence outside Hunan Province were excluded. In total, 6,597 patients were included in the final analysis.
Research methods
Phenotypic drug susceptibility testing for first–line anti–TB drugs–isoniazid (INH), rifampicin (RIF), ethambutol (EMB), and pyrazinamide (PZA)–was conducted using the absolute concentration method on solid media. Fresh colonies grown on Löwenstein–Jensen (L–J) medium were harvested, homogenized, and adjusted to a concentration of 1 mg/mL. The suspension was subsequently diluted 100–fold with sterile saline, and 0.1 mL of the diluted inoculum was inoculated onto solid medium slopes. After thorough mixing, the medium were incubated at 37 °C, and results were evaluated after 4 weeks. All procedures were performed in a Class II biosafety cabinet in accordance established with laboratory safety guidelines.
Quality control
All laboratory staff underwent proficiency training provided by National Tuberculosis Reference Laboratory (NTRL). Each batch of culture medium underwent sterility testing and was verified with the H37Rv reference strain to ensure accuracy and reproducibility. All testing procedures were conducted in compliance with established quality–control standards.
Statistical analysis
Data cleaning and statistical analysis were conducted in R (version 4.2.2) using RStudio. Figures were produced in R and Excel. Descriptive statistics summarized the distribution of DR–TB. Associations with age, sex, occupation, and region were examined using chi–square tests for categorical variables and Mann–Whitney U tests for continuous variables. Multivariable logistic regression was fitted including the following factors: year, region, age group, occupation and sex. Odds ratios (ORs) with 95% confidence intervals (CIs) and two–sided P–values were calculated; p < 0.05 was considered statistically significant.
Results
Epidemiology of DR–TB
This study included 6,597 patients with DR–TB diagnosed at Hunan Chest Hospital between 2014 and 2023. Among them, 4,946 were male and 1,651 were female, with a male–to–female ratio of 3.00:1. Ages ranged from 5 to 88 years, with a median of 50 years (interquartile range (IQR): 34–60). The 50–59 age group accounted for the highest proportion of cases (24.78%, 1,635/6,597), followed by the 60–69 age group (17.34%, 1,144/6,597; Figure 1A). Given the small number of cases aged < 10 years (n = 3), this group was merged with the ≤ 20 years category for subsequent analyses. By occupation, farmers accounted for the largest proportion of cases (64.44%, 4,251/6,597), followed by unemployed individuals (8.70%, 574/6,597) and public–sector employees (7.91%, 522/6,597) (Figure 1B). Temporal trend analysis (Figure 1C) showed that the number of DR–TB cases was relatively high between 2016–2018, peaking in 2017, and declined from 2019 to 2021. Regional analysis (Figure 1D) indicated that cases were concentrated in Changsha (16.39%, 1,081/6,597), Shaoyang (13.78%, 909/6,597), and Loudi (9.05%, 597/6,597), together accounting for 39.22% of all cases; fewer cases occurred in Xiangxi (0.26%, 17/6,597) and Zhangjiajie (1.00%, 66/6,597). Spatial distributions of DR–TB subtypes are shown in Appendix Table S1.
The distributions of DR–TB in Hunan, China, from 2014 to 2023. (A) Age distribution; (B) occupational distribution; (C) temporal distribution; and (D) spatial distribution.
Patterns of drug resistance subtypes
In this study, INH–R TB had the highest positivity rate (56.27%; 95% CI: 55.07–57.67), followed by MDR–TB (52.37%; 95% CI: 51.17–53.58). The rates for SDR–TB and RR–TB were similar, at 32.71% (95% CI: 31.58–33.84) and 31.47% (95% CI: 30.35–32.59), respectively. In contrast, PDR–TB had the lowest rate (13.75%; 95% CI: 12.92–14.58). Detailed results are shown in Table 1. The distribution of different DR–TB types across age groups was examined using the chi–square test, with results presented in Table 2. Among the 6,597 patients included, MDR–TB (3,455 cases) and INH–R TB (3,712 cases) were the most common types. Age distributions differed significantly across all resistance categories (p < 0.05). Overall, the number of DR–TB cases increased with age before declining, with a peak in the 50–59 age group. Specifically, INH–R TB and MDR–TB showed similar age–specific patterns, with the highest proportions in the 50–59 age group (INH–R TB: 961 cases, 25.9%; MDR–TB: 894 cases, 25.9%), followed by the 40–49 age group. In contrast, RR–TB, SDR–TB, and PDR–TB were also concentrated mainly in middle–aged and older adults, but their proportions within the ≥ 70 age group differed. Figure 2 illustrates the predominant subtypes of DR–TB across age groups.
Subtypes of DR–TB in each age group (years). This figure illustrates the distribution of DR–TB subtypes by proportion across age groups (in descending order). The classification of DR–TB encompasses, but is not limited to, the subtypes displayed.
Temporal profiling of DR–TB
From 2014 to 2023, detection rates of the different DR–TB types showed distinct patterns (Figure 3). RR–TB consistently had the highest rate and displayed a temporal trend similar to MDR–TB. The MDR–TB rate peaked in 2018, then declined with fluctuations. SDR–TB and INH–R TB remained relatively stable, generally ranging from 30 to 40%, with parallel trends and only minor variations. PDR–TB had the lowest rate throughout the study period. Chi–square tests indicated that, except for RR–TB, distributions of the other subtypes varied significantly by year (SDR–TB, PDR–TB, MDR–TB, and INH–R TB: p < 0.05; χ^2^ = 27.797, 10.322, 39.609, and 36.990, respectively). Detailed results are provided in Appendix Table S1.
Temporal trends in detection rates of different DR–TB types, 2014–2023. The Y–axis represents the proportion of each DR–TB type, calculated as its case count divided by the total number of DR–TB cases for that year.
Differences by region, sex, and occupation
Based on geographic location, the 14 prefecture–level divisions of Hunan Province were grouped into five regions: eastern (Changsha, Xiangtan, Zhuzhou), southern (Hengyang, Yongzhou, Chenzhou), western (Zhangjiajie, Xiangxi, Huaihua), northern (Yueyang, Changde), and central (Loudi, Yiyang, Shaoyang). Regional analysis showed significant differences in the distribution of SDR–TB, PDR–TB, MDR–TB, RR–TB, and INH–R TB across these regions (χ^2^ = 134.501, 16.524, 197.853, 123.445, and 165.209, respectively; p < 0.05). Gender–based analysis revealed that males constituted a significantly higher proportion of cases than females for SDR–TB, MDR–TB, RR–TB, and INH–R TB (χ^2^ = 4.350, 163.308, 105.798, and 170.558, respectively; p < 0.05). Regarding occupational distribution, farmers represented the largest subgroup within the study population. Chi–square tests indicated significant variation in the distribution of SDR–TB, MDR–TB, RR–TB, and INH–R TB across occupational categories (χ^2^ = 39.165, 58.294, 34.275, and 64.518, respectively; p < 0.05). Detailed results are shown in Appendix Table S1 and Supplementary Figure S1.
Multivariable analysis of risk factors
The results of the multivariate logistic regression analysis are summarized in Figure 4. For SDR–TB, the incidence risk generally decreased from 2015 to 2023 compared with 2014. Geographically, the eastern region had a significantly higher risk (OR = 1.334), whereas the northern, southern, and western regions had lower risks. For PDR–TB, the risk was significantly higher in 2016 (OR = 1.515) and 2021 (OR = 1.574) compared with 2014, and the eastern region also showed increased risk (OR = 1.208). For MDR–TB, the risk was significantly elevated in 2016, 2018, and 2019 compared with 2014. Spatially, the eastern region had lower risk (OR = 0.658), whereas the northern (OR = 1.219), southern (OR = 1.388), and western (OR = 1.734) regions had higher risks. Individuals aged 20–69 years were at significantly higher risk than those under 20 years, and females had a lower risk than males (OR = 0.819). For RR–TB, the risk increased significantly in 2018 (OR = 1.344). The eastern region had lower risk, while the southern and western regions had higher risks. The 20–69 age group had elevated risk, and females had a lower risk than males (OR = 0.784). For INH-R TB, the risk decreased in 2018 and 2021. The eastern region showed higher risk, whereas other regions had lower risks. Females were at significantly higher risk than males (OR = 1.137). Detailed results are provided in Appendix Table S2.
Forest plot of the multivariable analysis. Forest plot of multivariable analyses showing the associations between various risk factors and different DR–TB subtypes.
Discussion
This 10–year retrospective study examines the DR–TB epidemic in Hunan Province, South–Central China. The analysis identifies distinct temporal, geographic, and demographic patterns, providing evidence to inform targeted public health strategies.
The predominance of RR–TB and INH–R TB among resistance types is noteworthy. Both showed temporal trends similar to MDR–TB, with all three peaking in 2018. This pattern may be attributed to the widespread use of RIF and INH as first–line anti–TB drugs. Inconsistent treatment adherence and non–standardized medication practices can create selective pressure, promoting the emergence and transmission of resistant strains. This phenomenon aligns with findings from other high–TB–burden regions (13, 14). The subsequent rebound in resistance rates observed in 2023 may reflect disruptions in TB control services during the COVID–19 pandemic, such as resource reallocation and interruptions in patient follow–up (15–17), underscoring the necessity for sustained vigilance in the post–pandemic era. It should be noted, however, that data collection for 2023 was incomplete due to a hospital information system upgrade concluding in August, which may have influenced the annual estimates.
Geographically, we observed clear spatial disparities in the distribution of DR–TB. The western and southern regions of Hunan had the highest burden of MDR–TB, showing an inverse association with socioeconomic development, consistent with prior studies (18–20). This pattern may reflect limited healthcare access and suboptimal treatment adherence in the mountainous west. In the south, a major source of out–migrant labor, treatment interruption among mobile populations could facilitate transmission of resistant strains (21, 22). By contrast, the more developed eastern region showed lower odds of MDR–TB (OR = 0.658), likely due to stronger TB control infrastructure, including broader DOTS coverage and wider availability of rapid molecular DST (23).
Across most DR–TB subtypes, male patients constituted a significantly higher proportion of cases (73–77%), exceeding the corresponding figures reported in countries such as Mexico and Japan (24, 25). This gender disparity may be attributable to factors including a higher prevalence of smoking among men–which can impair pulmonary immunity–greater occupational exposure to silica dust and other hazardous agents (e.g., in mining or construction), and a tendency to delay seeking medical care (26–28). Individuals aged 30–59 years exhibited a higher incidence of MDR–TB and RR–TB, indicating increased vulnerability potentially linked to high social mobility, greater work–related stress, and heavier comorbidity burdens. Although healthcare resources for this age group are generally sufficient, competing job demands and delayed healthcare–seeking may limit their timely access to TB services.
Farmers accounted for the majority of DR–TB cases (64.44%), highlighting substantial weaknesses in rural TB control. This vulnerability may be linked to insufficient health insurance, low health literacy, physically demanding work, and poor nutrition among agricultural workers, factors that can elevate the risk of TB infection and drug resistance (29–31). The unemployed comprised 8.70% of cases; we speculate that many lost their work capacity due to TB, with unemployment further aggravating economic and social marginalization, thereby perpetuating a vicious cycle of poverty and disease. This pattern underscores the profound impact of DR–TB on patients’ livelihoods and social functioning.
Multivariable logistic regression confirmed an elevated risk of MDR–TB in the western region (OR = 1.734) and among adults aged 30–49 years (OR > 2.0). Public sector employees had a significantly lower risk compared with farmers (OR = 0.710), suggesting that occupational disparities in healthcare access are a potential target for intervention (32). The modestly increased risk of INH–R TB among females (OR = 1.137) warrants further investigation into potential sex–based differences in drug metabolism (e.g., N–acetyltransferase 2 activity) and caregiving–related exposure (33, 34).
Despite insights from this large, decade–long analysis of the DR–TB epidemic in Hunan Province, several limitations should be considered. First, the single–center, retrospective design may limit generalizability and preclude causal inference. Second, the absence of genotyping data limits analysis of transmission dynamics and molecular clustering. Third, missing data on key confounders–including HIV or diabetes comorbidity, behavioral factors (e.g., smoking and alcohol use), and detailed treatment history–may bias risk–factor analyses. Finally, because some second–line and newer antituberculosis drugs were introduced unevenly during the study period, drug–resistant tuberculosis (XDR–TB) and pre–extensively drug–resistant tuberculosis (pre–XDR–TB) were not included in the epidemiologic analyses.
Future multicenter, prospective studies that incorporate whole–genome sequencing (WGS) and qualitative assessments of treatment adherence are needed to address these limitations and clarify the epidemiology of DR–TB.
Conclusion
The DR-TB epidemic in Hunan Province shows marked spatiotemporal heterogeneity and distinctive demographic clustering. To address these challenges, precision public health interventions are essential. Key priorities include (1) expanding the use of rapid molecular diagnostics and DST in high–burden western and southern regions; (2) implementing flexible, community–based directly observed therapy programs tailored to farmers and migrant populations; and (3) enhancing medical security and health education for high–risk occupational groups through coordinated cross–sectoral action. These findings provide a robust evidence base for developing region-specific DR–TB control guidelines in China and comparable settings.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The Lancet Public Health. Taking tuberculosis out of the shadows. Lancet Public Health. (2023) 8:e 247. doi: 10.1016/S 2468-2667(23)00063-436965975 PMC 10036124 · doi ↗ · pubmed ↗
- 2Tiberi S Utjesanovic N Galvin J Centis R D'Ambrosio L van den Boom M . Drug resistant TB –latest developments in epidemiology, diagnostics and management. Int J Infect Dis. (2022) 124:S 20–5. doi: 10.1016/j.ijid.2022.03.02635342000 · doi ↗ · pubmed ↗
- 3Dookie N Ngema SL Perumal R Naicker N Padayatchi N Naidoo K. The changing paradigm of drug–resistant tuberculosis treatment: successes, pitfalls, and future perspectives. Clin Microbiol Rev. (2022) 35:e 0018019. doi: 10.1128/cmr.00180-19, 36200885 PMC 9769521 · doi ↗ · pubmed ↗
- 4Pei S Song Z Yang W He W Ou X Zhao B . The catalogue of Mycobacterium tuberculosis mutations associated with drug resistance to 12 drugs in China from a nationwide survey: a genomic analysis. Lancet Microbe. (2024) 5:100899. doi: 10.1016/S 2666-5247(24)00131-9, 39353459 PMC 11543636 · doi ↗ · pubmed ↗
- 5Akalu TY Clements ACA Xu Z Bai L Alene KA. Mapping drug–resistant tuberculosis treatment outcomes in Hunan Province, China. Trop Med Infect Dis. (2024) 10:3. doi: 10.3390/tropicalmed 10010003, 39852654 PMC 11769319 · doi ↗ · pubmed ↗
- 6Zhao LL Chen Y Chen ZN Liu HC Hu PL Sun Q . Prevalence and molecular characteristics of drug–resistant Mycobacterium tuberculosis in Hunan, China. Antimicrob Agents Chemother. (2014) 58:3475–80. doi: 10.1128/AAC.02426-1424733464 PMC 4068477 · doi ↗ · pubmed ↗
- 7Farhat M Cox H Ghanem M Denkinger CM Rodrigues C Abd El Aziz MS . Drug–resistant tuberculosis: a persistent global health concern. Nat Rev Microbiol. (2024) 22:617–35. doi: 10.1038/s 41579-024-01025-1, 38519618 · doi ↗ · pubmed ↗
- 8Sahasrabudhe T Nilgiri KM. Quantitative study of physical, social, psychological, and environmental challenges faced by patients with drug–resistant tuberculosis. Cureus. (2024) 16:e 69694. doi: 10.7759/cureus.69694, 39435239 PMC 11492352 · doi ↗ · pubmed ↗