Endotoxemia and its association with immune and coagulopathy responses in severe community-acquired pneumonia and COVID-19
Mathieu Blot, Amadou-Khalilou Sow, David Masson, Maxime Nguyen, Marine Jacquier, Jean-Paul Pais de Barros, Thibault Sixt, Maxime Luu, Pierre-Emmanuel Charles, Lionel Piroth, Jean Pierre Quenot, Christine Binquet, Jean-Pierre Quenot, Jean-Pierre Quenot, Pierre-Emmanuel Charles

TL;DR
This study found no evidence of increased gut-derived endotoxemia in severe pneumonia or COVID-19 patients, challenging its role in systemic inflammation.
Contribution
A highly specific mass spectrometry method revealed no elevated lipopolysaccharide in severe pneumonia or COVID-19 patients.
Findings
Median plasma LPS concentrations were significantly lower in severe pneumonia and COVID-19 patients compared to healthy volunteers.
LPS levels did not correlate with disease severity or mortality and showed no increased risk of thrombotic events.
Findings challenge the hypothesis that gut-derived endotoxemia drives systemic inflammation in severe pneumonia.
Abstract
Acute community-acquired pneumonia (CAP) is a leading cause of infection-related mortality worldwide. Endotoxemia, characterized by elevated plasma lipopolysaccharide (LPS), is a key driver of inflammation and thrombosis in Gram-negative sepsis and has been suggested to occur in severe pneumonia, irrespective of etiology. However, current immunoassays for LPS quantification lack sensitivity and specificity. We aimed to quantify plasma LPS in severe CAP patients, including COVID-19, using a validated mass spectrometry method, and to explore associations with immune activation, coagulation, gut translocation, and clinical outcomes. In this prospective ancillary study of the LYMPHONIE cohort, we included 34 non-COVID-19 severe CAP (sCAP), 34 severe COVID-19 (sCOVID-19) and 34 matched healthy volunteers. Plasma LPS was measured by LC–MS/MS detecting 3-hydroxy fatty acids of lipid A.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
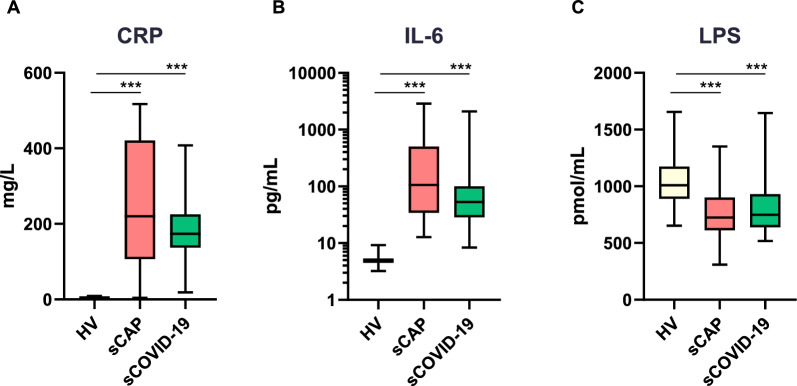 Figure 1
Figure 1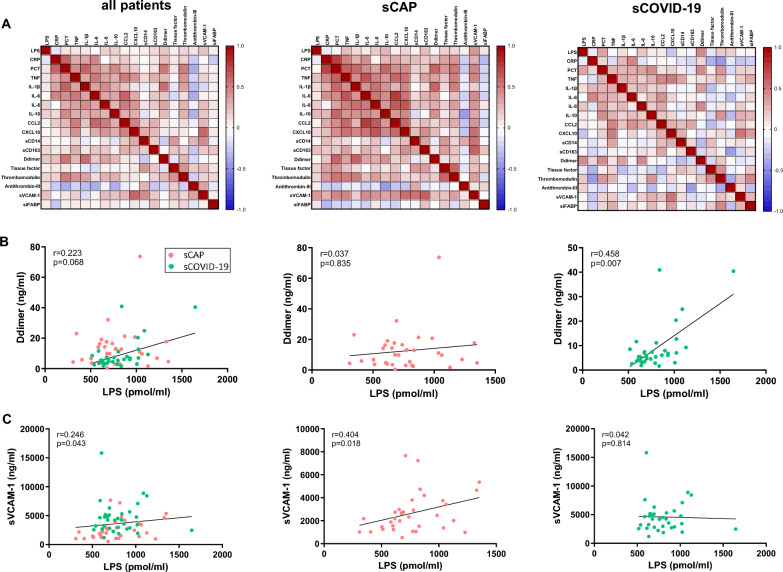 Figure 2
Figure 2- —AOI (Appel d’Offre Interne) from the University hospital of Dijon
- —INSERM (Institut National de la Sante et de la Recherche Medicale - Center de Recherche UMR 1231, Dijon, France)
- —the national research agency (ANR) Investissements d’Avenir Grant (ANR-11 LABX-0021-01, Labex Lipstic, Dijon, France)
- —Université Bourgogne-Europe (Dijon, France)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsImmune Response and Inflammation · Sepsis Diagnosis and Treatment · Clinical Nutrition and Gastroenterology
Background
Acute community-acquired pneumonia (CAP) remains the leading cause of death from infectious diseases worldwide. The most frequent pathogens are viruses, including SARS-CoV-2, influenza viruses, and Gram-positive bacteria, primarily Streptococcus pneumoniae. Severe cases are marked by a dysregulated host immune response, which contributes to circulatory failure, multi-organ dysfunction, and thrombotic complications [1].
Endotoxemia**,** defined by elevated plasma concentrations of lipopolysaccharide (LPS), is a central driver of inflammation and thrombosis in Gram-negative bacterial sepsis [1]. However, preclinical and clinical evidence suggests that LPS translocation into the bloodstream may also occur in early-stage sepsis of non-Gram-negative origin and is associated with poor outcomes [2–4]. In patients with CAP, circulating LPS levels can be comparable to levels observed in Gram-negative bacteremia, despite the absence of LPS-expressing pathogens [5]. In addition, low-grade endotoxemia is associated with short- and long-term risk of cardiovascular events in CAP patients [6]. Low-grade endotoxemia has also been detected in COVID-19 [7–10]. Interestingly, the SARS-CoV-2 spike protein may bind bacterial LPS and enhance its pro-inflammatory effects [11], and could favor thrombosis by eliciting a pro-inflammatory and pro-coagulant state.
This suggests that endotoxemia may reflect gut-derived bacterial translocation, driven by intestinal barrier dysfunction during critical illness, regardless of the primary pathogen. Elevated LPS levels have been associated with features of sepsis-induced immunoparalysis and may also be exacerbated by mechanical ventilation, which in preclinical models promotes enterocyte apoptosis and intestinal barrier breakdown [12].
Digestive decontamination with non-absorbable antibiotics has been shown in meta-analyses to reduce multi-organ dysfunction in ICU patients [13]. Additional non-antibiotic strategies are under investigation. Our group showed that recombinant phospholipid transfer protein (PLTP), a plasma protein that binds and neutralizes LPS, improves outcomes in murine models of peritonitis [14].
Overall, endotoxemia may serve as a biomarker of intestinal injury and systemic severity in severe pneumonia, independently of microbial etiology. A better understanding of its role could open new therapeutic avenues, including LPS neutralization or removal strategies.
However, the immunoassays currently used for LPS quantification suffer from technical limitations, including poor sensitivity and cross-reactivity, particularly with immunoassay-based tests, which call into question the reliability of the results obtained using these methods.
Our study aims to compare plasma concentrations of LPS between patients with severe community-acquired pneumonia (CAP) caused by SARS-CoV-2 (sCOVID-19) or other pathogens (sCAP) and healthy volunteers (HV), using a patented high-performance liquid chromatography–tandem mass spectrometry (LC–MS/MS) method that detects 3-hydroxy fatty acids (C10, C12, C14, C16, and C18), components of the lipid A moiety of LPS. Secondary analyses explored associations between LPS levels, immune and coagulation markers, gut translocation, and clinical outcomes.
Methods
This study is a prospective, exploratory ancillary analysis of the ongoing LYMPHONIE project (ClinicalTrials.gov identifier: NCT03505281), initiated in November 2018 at the Dijon-Bourgogne University Hospital (France).
Patients with severe community-acquired pneumonia
Eligible patients were those with severe community-acquired pneumonia, defined by the presence of: (1) clinical and radiological signs of pneumonia (at least two acute symptoms such as cough, purulent sputum, dyspnea, chest pain, body temperature < 35 °C or ≥ 38.5 °C, along with a new pulmonary infiltrate on imaging); (2) severity criteria, including at least two quick-SOFA components (systolic blood pressure ≤ 100 mmHg, respiratory rate ≥ 22 breaths/min, or Glasgow Coma Scale < 15), and/or the need for mechanical ventilation and/or vasopressors; and (3) diagnosis made within 48 h of hospital admission.
Non-inclusion criteria included age under 18 years, pregnancy, legal protection status, decisions to limit care, known immunodeficiency, chronic conditions associated with profound lymphopenia (e.g., cirrhosis, lymphoproliferative or myeloproliferative disorders, solid malignancy, or active systemic lupus erythematosus), or hospitalization for sepsis within the previous 3 months.
Patients with sCOVID-19 were included if they tested positive for SARS-CoV-2 by reverse transcriptase-polymerase chain reaction (RT-PCR) on a respiratory sample, whereas severe community-acquired pneumonia (sCAP) patients were those with no positive test for COVID-19.
Oral informed consent was obtained from patients or their legal representatives. The study was approved by the regional ethics committee (Comité de Protection des Personnes SUD MEDITERRANEE V; reference 2017-A03404-49). Blood samples collected in ethylenediaminetetraacetic acid (EDTA) tubes were drawn within 48 h of admission. After centrifugation at 2000 × g for 10 min at 4 °C, plasma was aliquoted and stored at − 80 °C in the certified biological resource center (CRB Ferdinand Cabanne; NF S96-900 certified).
Healthy volunteers
We prospectively enrolled 34 healthy volunteers (HV). Inclusion criteria were: (i) age ≥ 18 years with oral consent provided; (ii) no fever, antibiotic use, or surgery within the previous 30 days; (iii) body temperature < 37.8 °C on the day of inclusion and no signs of suspected infection; and (iv) absence of any known immune deficiency. EDTA-treated whole blood was collected, and plasma was subsequently stored under the same conditions as for patient samples.
To ensure data comparability, we performed two separate matching procedures: one between HV and with sCOVID-19 patients, and the other between HV and sCAP patients. In both cases, matching was performed on sex and age. No matching was applied for comorbidities or body mass index.
Variables of interest, clinical outcomes, and data collection
Clinical and biological parameters, along with the Charlson Comorbidity Index and severity scores—including the Sequential Organ Failure Assessment (SOFA), Simplified Acute Physiology Score II (SAPS II), and Pneumonia Severity Index (PSI)—were recorded at the time of inclusion. Acute respiratory distress syndrome (ARDS) was defined according to the Berlin criteria [15], while septic shock was defined as persistent hypotension requiring vasopressor support with a serum lactate concentration > 2 mmol/l despite adequate fluid resuscitation.
Clinical outcomes were assessed up to 30 days following hospital admission. These included 30-day mortality, the number of hospital-, ICU-, and ventilator-free days, as well as the occurrence of venous thromboembolic events and cardiovascular events (CVE).
Ventilator-free days were defined as the number of days alive between day 1 and day 30 after the onset of severe pneumonia during which the patient was breathing without mechanical ventilation.
Venous thromboembolic events were diagnosed during routine care, using computed tomography pulmonary angiography for pulmonary embolism and vascular ultrasonography for deep vein thrombosis. Cardiovascular events included myocardial infarction, ischemic stroke, or cardiovascular death.
All data were collected by trained clinical research assistants using a standardized electronic case report form (Cleanweb™), which included automated validation rules to flag missing or inconsistent entries. In addition, all data underwent double-checking to ensure accuracy and completeness.
Plasma biomarkers of immune and coagulopathy response, and gut dysfunction
Fourteen plasma analytes were quantified using a Luminex multiplex assay (R&D Systems, USA), following the manufacturer’s instructions. These included cytokines and chemokines [TNF, IL-1β, IL-6, IL-8, IL-10, chemokine (C–C motif) ligand 2 (CCL2), and chemokine (C-X-C motif) ligand 10 (CXCL10)]; markers of monocyte/macrophage activation [soluble CD14 (sCD14) and soluble CD163 (sCD163)]; and biomarkers of coagulopathy [D-dimer, tissue factor, thrombomodulin, antithrombin III, and soluble vascular cell adhesion molecule-1 (sVCAM-1)]. All measurements were performed on the same day by the same operator to minimize inter-assay variability.
In addition, human plasma concentrations of intestinal fatty acid-binding protein (I-FABP), a surrogate marker of gut barrier integrity, were measured using a commercially available enzyme-linked immunosorbent assay (ELISA), also following the manufacturer’s protocol (R&D Systems, Minneapolis, MN, USA).
Lipopolysaccharide measurement
Plasma LPS concentrations were measured using a patented LC–MS/MS method (EndoQuant), specifically designed for the targeted quantification of 3-hydroxy (3-OH) fatty acids (C10, C12, C14, C16, and C18), which are covalently linked to the lipid A moiety of LPS [16]. For this purpose, two plasma aliquots (100 µL each) were spiked with 4 pmol of internal standards (3-hydroxyundecanoic, 3-hydroxytridecanoic, 3-hydroxyheptadecanoic).
Plasma was hydrolyzed (for total 3-OH fatty acids) or left unhydrolyzed (for unesterified 3-OH fatty acids) using 8 M HCl for 3 h at 90 °C. Fatty acids were then extracted using a hexane/ethyl acetate (3:2) solvent mixture and reconstituted in ethanol after vacuum evaporation. Chromatographic separation was done using an Infinity 1260 HPLC binary system (Agilent) equipped with a ZORBAX SB-C18 column (50 × 2.1 mm, 1.8 µm; Agilent) maintained at 30 °C. MS/MS detection was carried out on an Agilent QQQ 6490 triple quadrupole mass spectrometer fitted with a Jet-Stream electrospray ionization (ESI) source. Quantification of 3-OH fatty acids was achieved in negative selected reaction monitoring (SRM) mode, as previously described [16, 17].
The esterified fraction of 3-OH fatty acids (i.e., those bound to LPS) was calculated by subtracting the concentration of unesterified 3-OH fatty acids from the total concentrations. Final plasma LPS concentrations were expressed as the sum of esterified 3-OH fatty acids.
Statistical analyses
Categorical variables were summarized as counts and percentages, and continuous variables were described using medians and interquartile ranges (IQR), as most variables did not follow a normal distribution. Baseline patient (sCOVID-19 and sCAP) and HV characteristics were described and compared between groups. The percentage of patients with low and high plasma LPS levels, defined according to the median value of LPS in patients (sCAP and sCOVID-19), was described and compared. Using the median plasma LPS concentration as the cutoff is an unbiased data-driven approach chosen in the absence of an established clinical or biological threshold and to ensure balanced group sizes. Categorical variables were compared using Fisher’s exact test or McNemar’s test, as appropriate. For continuous variables, the Wilcoxon signed-rank test was used. Spearman’s correlation coefficients were calculated to assess correlations, as appropriate. P-values < 0.05 were considered statistically significant and are highlighted in bold in the tables. Statistical analyses were conducted using R software (version 4.3.0), and figures were generated with GraphPad Prism (version 10.0.3).
Results
Population included
We included 34 patients with sCAP, 34 with sCOVID-19, and 34 matched HV. Among patients with sCAP, the etiologies were bacterial in 11 patients (32%), viral in 8 (24%), mixed in 5 (15%), and unknown in 10 (29%). In the sCOVID-19 group, 4 patients (12%) had a documented bacterial coinfection (Suppl. Table 1).
Intensive care unit admission was required for 31 (91%) of sCAP patients and 34 (100%) of sCOVID-19 patients. Median SOFA score was 9.5 (6-11) for sCAP patients, and 7 (4-8) for sCOVID-19 patients. Septic shock and ARDS were reported in 10 (29%) and 21 (62%) of sCAP patients, and in 4 (12%) and 31 (91%) of sCOVID-19 patients, respectively. Two-thirds of patients required vasopressors. Venous thrombosis was reported in 4 (12%) of sCAP patients, and 6 (18%) of sCOVID-19 patients. Cardiovascular events were reported in 6 (18%) of patients from both the sCAP and sCOVID-19 groups. Thirty-day mortality was 6% and 12% for sCAP patients and sCOVID-19 patients, respectively (Table 1). Table 1. Baseline characteristics and outcomes of the study population (LYMPHONIE study, 2018–2022)Normal rangeMissing dataStudy groupP* valueHealthysCAPsCOVID-19H versus NCH versus CN = 34N = 34N = 34DemographicsAge (yr), median (IQR)63 (52–71)66 (57–71)65 (52–71)0.1070.130Male sex, n (%)20 (59)26 (76)19 (56)0.0770.999Body-mass index (kg/m^2^), median (IQR)25 (24–29)29 (27–37)31 (26–35)0.0030.004Chronic comorbiditiesCardiovascular disease, n (%)2 (6)8 (24)6 (18)0.0410.289Pulmonary disease, n (%)012 (35)4 (12)0.0010.134Diabetes mellitus, n (%)1 (3)10 (29)12 (35)0.016****0.003Charlson score0 (0–1)1 (0–2)1 (0–1)0.0010.074Severity at hospital admissionSeptic shock, n (%)010 (29)4 (12)ARDS, n (%)021 (62)31 (91)Pneumonia severity index, median (IQR)–117 (86–135)83 (71–111)SAPS II, median (IQR)–27 (17–35)17 (9–26)SOFA score, median (IQR)–9.5 (6–11)7 (4–8)Biological findings on admissionASAT (IU/l), median (IQR)15–370/0/2–47 (27–97)76 (45–111)Serum creatinine (μmol/l), median (IQR)59–104–109 (73–172)80 (61–100)NT-ProBNP (pg/ml), median (IQR) < 1250/0/1–1748 (640–7488)283 (81–1322)PaO_2_:FiO_2_ (mm Hg), median (IQR) ≥ 400–118 (72–166)115 (86–172)Arterial pH (mm Hg), median (IQR)7.35–7.45–7.37 (7.24–7.43)7.44 (7.35–7.46)Serum bicarbonate (mmol/l), median (IQR)20–290/0/1–23.5 (21–27)25 (23–27)Lactate level (mmol/l), median (IQR)0.5–2.0–2.15 (1.40–3.60)1.50 (1.30–2.50)C-reactive protein (mg/l), median (IQR) < 3.20/0/22 (2–2)220 (107–417)174 (137–224) < 0.001** < 0.001Platelets (× 10^9^/l), median (IQR)150–400232 (198–268)171.5 (144–244)240 (176–318) < 0.0130.432Leukocytes (× 10^6^/l), median (IQR)3.8–9.56.3 (5.2–7.3)10.4 (7.5–14.2)7.9 (4.7–12.8) < 0.0010.002Neutrophils (× 10^6^/l), median (IQR)1.7–5.83.5 (2.7–4.3)9.1 (6.6–14.7)6.5 (3.7–11.2) < 0.001 < 0.001Lymphocytes (× 10^3^/l), median (IQR)1.07–4.031625 (1325–2175)545 (290–900)755 (530–820) < 0.001**** < 0.001**Monocytes (× 10^3^/l), median (IQR)0.2–0.7420 (345–595)415 (220–860)315 (220–540)0.6810.094TreatmentsICU admission, n (%)–31 (91)34 (100)Antibiotic multitherapy, n (%)–26 (76)19 (56)Corticosteroids, n (%)–20 (59)24 (71)Invasive mechanical ventilation, n (%)–25 (74)27 (79)Renal replacement therapy, n (%)–7 (21)2 (6)Vasopressors, n (%)–20 (59)19 (56)OutcomesVenous thrombosis event, n (%)–4 (12)6 (18)Cardiovascular event, n (%)6 (18)6 (18)ICU-free days at 30 days (days), median (IQR)–18 (12–27)16 (10–30)Ventilator-free days at 30 days (days), median (IQR)–24 (14–30)16 (10–30)Hospital-free days at 30 days (days), median (IQR)–4.5 (0–16)0.50 (0–12)30-day mortality, n (%)–2 (6)4 (12)90-day mortality, n (%)–2 (6)5 (15)ARDS, acute respiratory distress syndrome; ICU, intensive care unit; IQR, interquartile range; sCAP, severe community-acquired pneumonia*Missing data: the notation X/Y/Z now indicates the number of missing values in the three respective groups (healthy volunteers/sCAP/sCOVID-19)
Comparison of characteristics and LPS levels in sCAP and sCOVID-19 patients with matched healthy volunteers
As expected, median age and sex ratio did not differ significantly between the patient groups and HV. However, sCAP patients had significantly higher body mass index (BMI), more frequent cardiovascular and pulmonary comorbidities, diabetes, and a higher Charlson comorbidity index. Compared to HV, sCOVID-19 patients also had higher BMI and a greater prevalence of diabetes (Table 1).
Compared to HV, patients with sCAP and sCOVID-19 exhibited significantly elevated levels of inflammatory biomarkers (CRP, TNF, IL-1β, IL-6, IL-8, CCL2, CXCL10, sCD14) as well as markers of coagulopathy (D-dimer, sVCAM-1), but showed lower levels of soluble I-FABP (Table 2, Fig. 1). Table 2. Plasma concentration of biomarkers of immune and coagulopathy responses, gut dysfunction, and LPS (LYMPHONIE study, 2018–2022)Study groupP valueHealthysCAPsCOVID-19H versus NCH versus CN = 34N = 34N = 34Cytokines, chemokinesTNF (pg/ml)7 (6–8)16 (10–20)12 (11–15)** < 0.001**** < 0.001IL-1β (pg/ml)12 (10–13)17 (13–21)13 (12–15) < 0.0010.006IL-6 (pg/ml)5 (4–5)106 (36–480)53 (29–100) < 0.001 < 0.001IL-8 (pg/ml)2 (2–2)6 (3–19)6 (4–10) < 0.001**** < 0.001IL-10 (pg/ml)8 (4–11)8 (6–13)8 (6–10)0.0640.385CCL2 (pg/ml)181 (160–212)315 (189–680)342 (248–528) < 0.001**** < 0.001CXCL10 (pg/ml)35 (27–44)231 (77–662)492 (323–692) < 0.001**** < 0.001Biomarkers of monocyte/macrophage activationsCD14 (ng/ml)2243 (1863–2601)3068 (2623–3542)3714 (2928–4080) < 0.001**** < 0.001sCD163 (ng/ml)594 (450–814)751 (515–1031)636 (547–864)0.0570.033Biomarkers of coagulopathyD-dimer (ng/ml)1114 (641–2037)9860 (4337–16,501)5901 (3665–8581) < 0.001**** < 0.001Tissue-factor (pg/ml)39 (35–49)39 (32–54)55 (47–66)0.343 < 0.001Thrombomodulin (ng/ml)5.43 (4.48–6.12)6.58 (4.39–8.67)5.55 (4.59–7.53)0.0180.163Antithrombin-III (ng/ml)3775 (2900–4384)2470 (2156–3284)4107 (3219–4639) < 0.0010.134sVCAM-1 (ng/ml)742 (663–1008)2258 (1376–3419)4241 (2814–5188) < 0.001**** < 0.001Biomarker of gut dysfunctionsI-FABP (pg/ml)362 (242–560)240 (111–394)173 (96–263)0.0780.008Endotoxemia measurementLPS (pmol/ml)1009 (921–1163)724 (615–872)750 (640–930) < 0.001**** < 0.001**Median and interquartile range are representedCCL, chemokine (C–C motif) ligand; CXCL, chemokine (C-X-C motif) ligand; IL, interleukin; LPS, lipopolysaccharide; PCT, procalcitonin; sVCAM, soluble vascular cell adhesion molecule-1; sI-FABP, soluble intestinal fatty acid-binding protein; TNF, tumor necrosis factorFig. 1Plasma LPS concentrations and inflammatory response in healthy volunteers and patients with severe community-acquired or COVID-19 pneumonia (LYMPHONIE study, 2018–2022). Data are presented as box-and-whisker plots and differences were analyzed using the Wilcoxon matched-pairs signed rank test and significance indicated as *p < 0.05; **p < 0.01; ***p < 0.001; ****p < 0.0001
Unexpectedly, median plasma concentrations of LPS were significantly lower in both sCAP patients (724 [615–872] pmol/ml) and sCOVID-19 patients (750 [640–930] pmol/ml), compared to matched HV (1009 [921–1163] pmol/ml; p < 0.001 for both comparisons) (Table 2, Fig. 1).
To investigate potential factors that could explain this difference, we observed a significant decrease in hemoglobin levels in both sCAP and sCOVID-19 patients, as well as a significant reduction in hematocrit in sCAP, compared with healthy volunteers, suggesting the presence of hemodilution (Supplemental Fig. S1).
Variables associated with high LPS levels
Patients with severe pneumonia (sCAP and sCOVID-19) were stratified into low and high LPS groups based on the median plasma LPS concentrations. Patients in the high LPS group more frequently had underlying pulmonary disease (p = 0.015) and tended to have a higher frequency of cardiovascular comorbidities (30% vs. 11%; p = 0.054). However, no significant differences were observed between the two groups in terms of septic shock or ARDS occurrence, SOFA scores, or levels of inflammatory and coagulopathy biomarkers. The proportion of pneumonia cases caused by Gram-negative bacteria was similar in both groups. Likewise, clinical outcomes did not differ significantly between the two groups (Tables 3 and 4). Table 3. Baseline characteristics and outcomes according to LPS plasma concentrations (LYMPHONIE study, 2018–2022)Missing dataOverallLow LPSHigh LPSP* valueN = 68N = 35N = 33DemographicsAge (yr), median (IQR)65 (57–71)65 (54–71)65 (57–71)0.893Male sex, n (%)45 (66)22 (63)23 (70)0.551Body-mass index (kg/m^2^), median (IQR)30.6 (26.4–36.8)30.8 (26.3–37.2)30.4 (26.5–36.4)0.961Chronic comorbiditiesCardiovascular disease, n (%)14 (21)4 (11)10 (30)0.054Pulmonary disease, n (%)16 (24)4 (11)12 (36)0.015Diabetes mellitus, n (%)22 (32)12 (34)10 (30)0.726Charlson score1 (0–1)1 (0–1)1 (0–1)0.534Severity at hospital admissionSeptic shock, n (%)14 (21)7 (20)7 (21)0.902ARDS, n (%)52 (76)27 (77)25 (76)0.893Pneumonia severity index, median (IQR)93 (73–128.50)91 (72–131)105 (77–128)0.641SAPS II, median (IQR)22 (14.50–34)22 (17–30)21 (11–36)0.888SOFA score, median (IQR)7.5 (4.5–10)8 (5–10)7 (4–10)0.980Biological findings on admissionASAT (IU/l), median (IQR)0/256.50 (38–110)56 (37–115)67 (40–97)0.782Serum creatinine (μmol/l), median (IQR)87 (63.50–135)78 (59–136)90 (79–117)0.116NT-ProBNP (pg/ml), median (IQR)0/1946 (229–4111)816 (194–1712)1497 (259–9207)0.169PaO_2_:FiO_2_ (mm Hg), median (IQR)115 (80–166)109 (79–163)141 (85–166)0.439Arterial pH (mm Hg), median (IQR)7.40 (7.30–7.45)7.40 (7.30–7.45)7.40 (7.30–7.45)0.610Serum bicarbonate (mmol/l), median (IQR)0/124 (21–27)25 (21–27)23.50 (21.50–26)0.416Lactate level (mmol/l), median (IQR)1.80 (1.30–2.80)1.80 (1.10–2.50)2.10 (1.40–3.39)0.087C-reactive protein (mg/l), median (IQR)1/1186.70 (129.20–301)186.70 (113–301)182.50 (132.60–296.75)0.677Platelets (× 10^9^/l), median (IQR)205.50 (157–294.5)211 (163–344)197 (146–265)0.162Leukocytes (× 10^6^/l), median (IQR)8.9 (6.6–13.8)9.1 (6.7–14.2)8.5 (5.6–13.4)0.544Neutrophils (× 10^6^/l), median (IQR)7.9 (5.3–13.1)8.0 (6.1–13.9)7.6 (4.8–12.4)0.354Lymphocytes (× 10^3^/l), median (IQR)665 (390–860)760 (530–900)560 (290–830)0.082Monocytes (× 10^3^/l), median (IQR)385 (220–685)420 (230–670)310 (190–700)0.361Microbiological featuresBacterial etiology identified, n (%)20 (29)9 (26)11 (33)0.491Gram-negative bacteria identified, n (%)15 (22)8 (23)7 (21)0.870TreatmentsICU admission, n (%)65 (96)34 (97)31 (94)0.608Antibiotic multitherapy, n (%)45 (66)26 (74)19 (58)0.145Corticosteroids, n (%)44 (65)23 (66)21 (64)0.858Invasive mechanical ventilation, n (%)52 (76)28 (80)24 (73)0.480Renal replacement therapy, n (%)9 (13)3 (9)6 (18)0.299Vasopressors, n (%)39 (57)23 (66)16 (48)0.151OutcomesVenous thrombosis event, n (%)10 (15)5 (14)5 (15)0.999Cardiovascular event, n (%)12 (18)8 (23)4 (12)0.246ICU-free days at 30 days (days), median (IQR)16.5 (9–26.5)17 (12–28)16 (6–25)0.999Ventilator-free days at 30 days (days), median (IQR)22 (11.5–30)24 (14–30)21 (11–30)0.168Hospital-free days at 30 days (days), median (IQR)1.5 (0–14.5)6 (0–14)0 (0–16)0.76130-day mortality, n (%)6 (9)2 (6)4 (12)0.42190-day mortality, n (%)7 (10)3 (7)4 (12)0.705ARDS, acute respiratory distress syndrome; ICU, intensive care unit; IQR, interquartile range; sCAP, severe community-acquired pneumoniaMissing data: the notation X/Y/Z now indicates the number of missing values in the two respective groups (low LPS/high LPS)Table 4. Plasma concentration of biomarkers of immune and coagulopathy responses, gut dysfunction according to LPS plasma concentrations (LYMPHONIE study, 2018–2022)OverallLow LPSHigh LPSP* valueN = 68N = 35N = 33Cytokines, chemokinesTNF (pg/ml)13 (10–18)13 (10–17)13 (11–20)0.690IL-1β (pg/ml)15 (12–18)14 (12–18)15 (12–19)0.424IL-6 (pg/ml)64 (30–158)73 (33–159)59 (29–158)0.820IL-8 (pg/ml)6 (4–13)5 (3–13)7 (4–14)0.244IL-10 (pg/ml)8 (6–11)7 (6–11)8 (6–13)0.454CCL2 (pg/ml)324 (208–572)309 (248–582)357.22 (189–563)0.927CXCL10 (pg/ml)412 (170–677)360 (211–733)423 (142–611)0.615Biomarkers of monocyte/macrophage activationsCD14 (ng/ml)3310 (2853–3988)3239 (2910–3661)3542 (2781–4080)0.331sCD163 (ng/ml)720 (537–1009)663 (547–864)775 (535–1023)0.615Biomarkers of coagulopathyD-dimer (ng/ml)6849 (4004–13046)5482 (3684–11,658)7916.81 (5382–13,159)0.163PCT (μg/l)1.24 (0.22–13.70)0.77 (0.22–12)2.81 (0.29–16.45)0.517Tissue-factor (pg/ml)49.2 (36.7–63.5)51.5 (36.7–64.4)48.6 (36.7–62.6)0.830Thrombomodulin (ng/ml)6.1 (4.6–8.2)6.4 (4.5–7.5)5.9 (4.8–8.5)0.480Antithrombin-III (ng/ml)3281 (2470–4147)2871 (2288–4225)3472 (2660–4140)0.239sVCAM-1 (ng/ml)2944 (2005–4747)2718 (1889–4755)3560 (2469–4739)0.227Biomarker of gut dysfunctionsI-FABP (pg/ml)183 (107–380)178 (89–394)184 (120–378)0.641Median and interquartile range are representedCCL, chemokine (C–C motif) ligand; CXCL, chemokine (C-X-C motif) ligand; IL, interleukin; LPS, lipopolysaccharide; PCT, procalcitonin; sVCAM, soluble vascular cell adhesion molecule-1; sI-FABP, soluble intestinal fatty acid-binding protein; TNF, tumor necrosis factor
No significant correlation was observed between LPS levels and severity scores (SOFA, PSI, or SAPS II) at day 0.
Most correlations between plasma LPS levels and biomarkers of immune or coagulopathy were weak and not statistically significant, suggesting little to no association. However, a low correlation was observed between LPS and soluble VCAM-1 (sVCAM-1) in the overall population (r = 0.246, p = 0.043), with a stronger correlation in sCAP patients (r = 0.404, p = 0.018). Similarly, LPS levels and D-dimer levels showed a low correlation with the overall population (r = 0.223, p = 0.043), and a more pronounced correlation in patients with sCOVID-19 (r = 0.458, p = 0.007) (Fig. 2).Fig. 2. Correlations between plasma LPS concentrations and immune or coagulopathy biomarkers (LYMPHONIE study, 2018–2022)
Discussion
In this prospective study using a validated LC–MS/MS-based quantification method, we observed that patients with severe pneumonia, including COVID-19 and CAP resulting from other etiologies, did not have increased plasma concentrations of LPS compared to matched healthy volunteers. These findings challenge previous assumptions and reports suggesting elevated endotoxemia in severe pneumonia and sepsis regardless of microbial etiology.
Following earlier studies reporting higher LPS levels in CAP patients, it was suggested that endotoxemia results from gut barrier dysfunction and microbial translocation, even in infections caused by non-Gram-negative pathogens. This “intestinal hypothesis” has gained traction as disruption of the digestive barrier is a well-recognized consequence of critical illness, and low-grade endotoxemia has been associated with adverse outcomes, including cardiovascular events [3, 6]. However, many of these findings were based on LAL (Limulus Amebocyte Lysate) assays that predominantly reflect the biologically active portion of circulating LPS, rather than its total burden. In addition, LAL-based assays are prone to false positives due to cross-reactivity with plasma components such as (1- > 3)-β-d-glucans and proteases [18, 19]. Moreover, plasma is a complex biological matrix containing lipoproteins and other factors capable of binding or inactivating LPS [16]. By contrast, our use of mass spectrometry to measure esterified 3-hydroxy fatty acids, specific components of lipid A, enables direct, sensitive, and specific quantification of total LPS mass [16, 17, 20]. This robust methodology may explain the discrepancy with prior studies and underscores the importance of assay selection when evaluating circulating LPS. Then, alterations in lipid metabolism during acute inflammation may reduce measurable plasma LPS levels through enhanced binding to LDL and VLDL particles and subsequent hepatic clearance, while tissue sequestration of LPS during severe organ dysfunction may further limit its circulation [21–26]. In addition, hemodilution related to fluid resuscitation likely contributes to lower plasma LPS concentrations in pneumonia patients, as supported by reduced hemoglobin and hematocrit levels. Differences in gut microbiota composition, potentially influenced by early antibiotic administration in the emergency department, cannot be excluded, although selective digestive tract decontamination was not used in our cohort.
Interestingly, despite lower LPS levels in patients compared to healthy controls, we observed a low positive correlation between LPS and markers of endothelial activation (sVCAM-1) and coagulation (D-dimer), particularly within each pneumonia subgroup. These findings suggest that even relatively low concentrations of circulating LPS might contribute to endothelial dysfunction and pro-thrombotic states, which are prominent features of severe pneumonia, including COVID-19. However, no significant association was found between LPS levels and the incidence of venous thromboembolism or cardiovascular events in our cohort, unlike previous studies [6].
Contrary to our expectations, plasma concentrations of I-FABP, a marker of enterocyte injury and gut permeability, were significantly lower in patients than in healthy volunteers. Similar results were observed in other studies of pneumonia and COVID-19 [27–29], and may reflect altered enterocyte turnover or plasma protein dilution during critical illness rather than preserved gut integrity. This finding, along with low LPS levels, does not support the hypothesis of increased gut-derived LPS translocation in our patient cohort.
Moreover, high LPS levels were not associated with more severe disease features such as septic shock, ARDS, or higher SOFA scores. The prevalence of Gram-negative pathogens was similar in patients with high vs. low LPS concentrations, further arguing against a direct microbial origin of circulating LPS.
Our findings align with prior experimental and clinical results showing the absence of significant endotoxemia during pneumococcal pneumonia, even in the presence of systemic inflammation and organ failure [29]. Together, these results challenge the concept of LPS translocation as a major driver of systemic inflammation in CAP and COVID-19.
The strengths of our study include its prospective design, use of a validated and highly specific LC–MS/MS assay for LPS quantification, and inclusion of well-characterized patient cohorts with matching to healthy controls. Biomarker measurements were centralized and standardized, reducing variability.
However, several limitations should be acknowledged. First, the sample size was relatively small, limiting statistical power for subgroup analyses. This is particularly relevant for rare outcomes such as thromboembolic or cardiovascular events. Second, despite matching, residual confounding due to comorbidities or medications cannot be entirely excluded. Then, patients and HV differed in comorbid conditions, introducing potential confounders in the interpretation of plasma LPS concentrations. Indeed, we only matched patients and HV on age and sex. However, this should be regarded as a conservative bias since certain comorbidities (i.e., chronic respiratory and cardiovascular or renal disease and high BMI) have been previously associated with increased endotoxemia and/or enhanced intestinal permeability [30–35]. Furthermore, we cannot exclude the possibility of later increases in LPS concentrations, as our samples were collected early (< 48 h). The findings of Kritselis et al. suggest that LPS kinetics may be ascending in some patients, especially those with sepsis secondary to pneumonia who ultimately do not survive compared to survivors [5]. Importantly, given the limited sample size, these results should be interpreted with caution. Lastly, I-FABP may be an imperfect marker of gut permeability in severe pneumonia. Conditions such as systemic inflammation, metabolic disturbances, and multi-organ dysfunction can alter enterocyte function and protein release, thereby reducing I-FABP levels in the circulation independently of overt epithelial injury [28, 36, 37]. However, we cannot rule out a potential effect of hemodilution to explain the lower concentrations of I-FABP in patients compared to HV.
Conclusions
In conclusion, using a highly specific LC–MS/MS assay, we found no evidence of increased plasma LPS concentrations in patients with sCOVID-19 or sCAP compared to HV. These findings suggest that gut-derived endotoxemia does not play a major role in the pathophysiology of severe pneumonia. Although moderate correlations between LPS and markers of endothelial activation were observed, LPS levels were not associated with clinical severity or outcomes in our series. Future studies with larger, well-stratified cohorts are needed to evaluate the activity and functional consequences of circulating LPS, and to better define the role of gut–lung crosstalk in pneumonia-related inflammation and thrombosis.
Supplementary Information
Additional file 1.