Esophageal Perforation Caused by an Ingested Fish Bone Leading to Aortic Pseudoaneurysm: A Rare Vascular Complication in a 54-Year-Old Patient
Martin Nguyen, Tai Nguyen, Long Nguyen, Thai Nguyen, Thao Pham

TL;DR
A 54-year-old woman developed a rare aortic pseudoaneurysm after swallowing a fish bone that pierced her esophagus, requiring urgent treatment to prevent life-threatening complications.
Contribution
This case report highlights a rare vascular complication of esophageal foreign body ingestion and emphasizes the need for close monitoring and multidisciplinary management.
Findings
A fish bone caused esophageal perforation and a thoracic aortic pseudoaneurysm in a 54-year-old patient.
Urgent TEVAR and hybrid surgical measures successfully managed the pseudoaneurysm without rupture or infection.
The case underscores the importance of surveillance and coordinated care to prevent catastrophic aortoesophageal fistula.
Abstract
Ingestion of sharp esophageal foreign bodies (EFBs) such as fish bones is common and usually benign, but transmural perforation can lead to rare, life-threatening vascular complications. A 54-year-old woman presented with acute chest pain after fish bone ingestion. Computed tomography angiography (CTA) demonstrated a linear radiopaque FB penetrating the esophageal wall at the T3 level and located near the proximal descending thoracic aorta. Endoscopic removal confirmed esophageal perforation, and broad-spectrum intravenous antibiotics were initiated. Despite initial management, follow-up imaging revealed the development of a thoracic aortic pseudoaneurysm (AP) at the site of penetration, prompting urgent thoracic endovascular aortic repair (TEVAR) with adjunctive hybrid surgical measures to preserve cerebral perfusion. The postoperative course was uneventful, and subsequent imaging…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
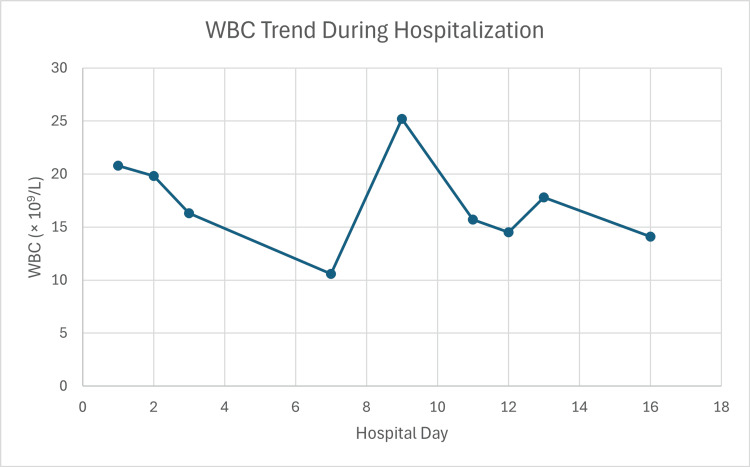 Figure 1
Figure 1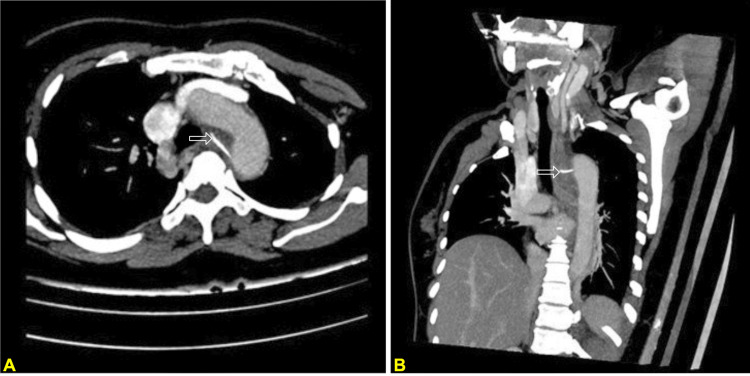 Figure 2
Figure 2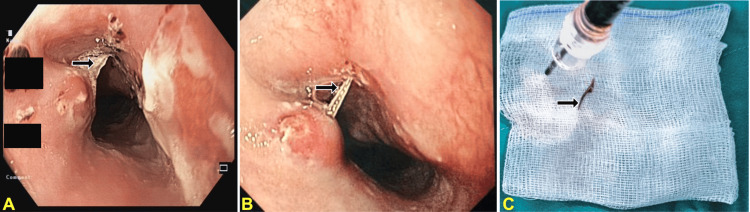 Figure 3
Figure 3 Figure 4
Figure 4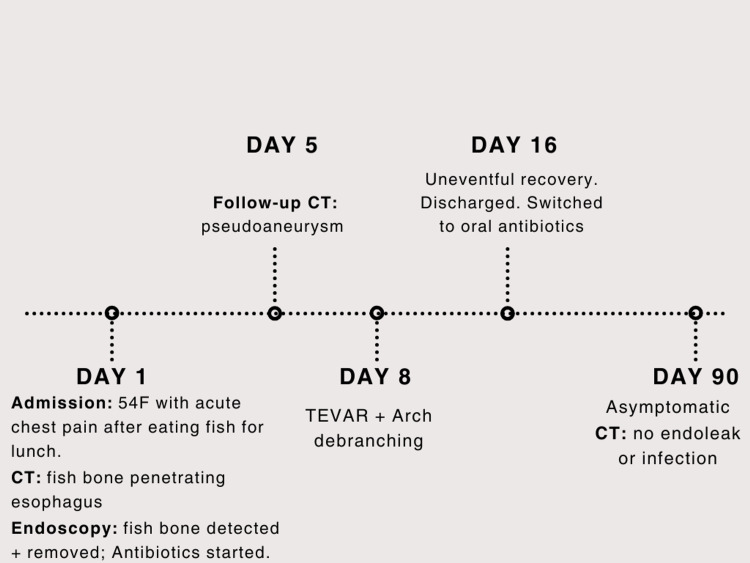 Figure 5
Figure 5| Lab | Result | Normal range |
| WBC | 20.8 × 109/L | 4-11 × 109/L |
| Neutrophils (%) | 89.9% | 40-70% |
| Hb | 144 g/L | 129-160 g/L |
| Hct | 42.7% | 36-47% |
| MCV | 87.7 fL | 80-95 fL |
| MCH | 29.6 pg | 26-34 pg |
| PLT | 401 × 109/L | 150-400 × 109/L |
| CRP | 43.1 mg/L | <1.5 mg/L |
| Clinical parameter | ASGE1 guidelines (2011) [ | ESGE2 guidelines (2016) [ | AJR3 guidelines (2014) [ |
| Primary screening modality | Biplane radiography: recommended to confirm the location, size, and shape of radiopaque objects and exclude free mediastinal air | Plain radiography: recommended to assess radiopaque objects5. Not recommended for uncomplicated nonbony food bolus impaction | Plain radiography: an initial screening tool, but acknowledged to have significant limitations for radiolucent objects |
| Sensitivity for fish bones | Low/variable: notes that fish or chicken bones are "not readily seen" on plain films8 | Quantified low (32%): explicitly cites prospective data indicating plain radiography has a sensitivity of only 32% for fish bones9 | Poor: states radiography "poorly visualizes fish bones" due to variable calcification and obscuration by soft tissue masses10 |
| Indications for CT | Adjunctive/limited: "may be useful" if radiographs are negative, though notes CT may still fail to detect radiolucent objects11 | Complication-focused: strongly recommended for patients with suspected perforation or complications requiring surgery | Diagnostic standard: considered the "test of choice" for fish bone impaction. Sensitivity reported at 90-100% with superior detection of "invisible" objects compared to plain film |
| Use of contrast studies | Contraindicated: generally should not be performed due to aspiration risk and interference with subsequent endoscopic visualization | Contraindicated (barium): barium swallow is not recommended. Water-soluble contrast is considered only if the X-ray is negative and obstruction is not suspected | Restricted: use of oral contrast is controversial and often discouraged due to aspiration risk. Water-soluble agents are reserved for confirming suspected perforation |
| Management of negative imaging | Endoscopy mandatory: persistent esophageal symptoms require endoscopic evaluation even in the setting of negative radiographic evaluation | Endoscopy mandatory: if X-ray is negative but suspicion remains, diagnostic work-up should proceed; medical treatment (e.g., glucagon) should not delay endoscopy | Advanced imaging (CT): a negative radiograph is insufficient to rule out sharp radiolucent objects; CT is indicated to unmask complications occult on plain film |
| Key distinction | Views CT primarily as a problem-solving tool when plain films are equivocal | Establishes the specific 32% sensitivity statistic for plain films, justifying a lower threshold for advanced imaging | Advocates for CT with 3D reconstruction as the definitive modality for radiolucent foreign bodies (fish bones, wood, plastic) |
| Author (year) | Age/sex | Foreign body | Diagnosis | Treatment strategy | Infection/complications | Outcome |
| Ma et al. (2026) [ | 74 F | Fish bone | Ruptured Pseudoaneurysm | TEVAR + endoscopic clips | Persistent mediastinitis | Recurrent bleeding (treatment failure) |
| Gong et al. (2022) [ | 71 F | Fish bone | Aortic perforation/AEF | TEVAR (no open surgery) | None | Survived (alive at 19 mo) |
| Gong et al. (2022) [ | 48 M | Fish bone | Aortic impalement | Simultaneous endoscopy + TEVAR | Transient fever | Survived (alive at 5 mo) |
| Zeng et al. (2020) [ | 58 M | Duck bone | Intramural hematoma | TEVAR + endoscopic removal | Not reported | Survived |
| Rawala et al. (2018) [ | 80 F | Unknown | AEF + aneurysm | TEVAR only | MRSA sepsis (stent infection) | Died (3 mo postop) |
| Shen et al. (2018) [ | 40 M | Chicken bone | AEF + pseudoaneurysm | TEVAR + thoracotomy (omentum flap) | Mild leukocytosis | Survived |
| Mezzetto et al. (2016) [ | 79 M | Goat bone | Pseudoaneurysm | TEVAR + endoscopic clips | Fever + leukocytosis | Survived |
| Xi et al. (2013) [ | 25 M | Fish bone | Pseudoaneurysm | TEVAR only | None | Survived |
| Chen et al. (2012) [ | 22 M | Chicken bone | AEF + pseudoaneurysm | TEVAR + thoracoscopy (debridement) | Leukocytosis (WBC 19.9) | Survived |
| Kelly et al. (2009) [ | 59 M | Fish bone | AEF | TEVAR → explantation | Sepsis (stent infection) | Survived (required open repair) |
| Assink et al. (2005) [ | 32 M | Fish bone | AEF | TEVAR + thoracotomy | None | Survived |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfectious Aortic and Vascular Conditions · Foreign Body Medical Cases · Esophageal and GI Pathology
Introduction
In the USA, esophageal foreign bodies (EFBs) occur in about 100,000 cases annually [1]. Accidental FB ingestion in adults often occurs in the elderly with cognitive impairment, while intentional ingestion may happen in individuals with psychiatric disorders [2]. The typical presentation includes acute dysphagia and the inability to swallow saliva. Other symptoms may include odynophagia, retrosternal pain, FB sensation, vomiting, and drooling [1]. Approximately 1%-3% of patients require surgery due to complications, including perforation, irretrievable FB, mediastinitis, empyema, fistula, and severe hemorrhage [3-5]. Osseous FB, such as fish or chicken bones, is a leading cause of esophageal injury [6].
Although the majority of ingested FB passes spontaneously, surgical intervention is required in less than 1% of cases [7]. In a landmark review of over 2,000 cases, aortic injury occurred in <0.1% of patients [8]. Within this rare subset, aortic pseudoaneurysm (AP) serves as a precursor to the more severe stage of aortoesophageal fistula (AEF). Because the mortality of untreated AEF approaches 100% [9], the identification of a pseudoaneurysm in a hemodynamically stable patient is one of the most important factors for survival. Here, we present an unusual case of pseudoaneurysm of the aorta caused by a fish bone in a middle-aged woman, which was successfully surgically managed.
Case presentation
A 54-year-old woman presented to the emergency department with acute chest pain following ingestion of a fish bone. She reported accidentally swallowing a bone during a meal, which became lodged in her throat. Attempts to dislodge it by swallowing rice were unsuccessful, leading to persistent throat discomfort and subsequent midline chest pain exacerbated by forceful coughing, without radiation or associated factors. She denied fever, dyspnea, hoarseness, odynophagia, or gastrointestinal bleeding.
Her past medical history was unremarkable, with no chronic illnesses, prior surgeries, or known allergies to medications or foods. She was not taking any regular medications and reported no tobacco, alcohol, or recreational drug use.
On examination, the patient was alert, tachycardic (115 bpm), and mildly febrile (37.9°C). Vital signs were otherwise stable, with normal blood pressure (120/80 mmHg), respiratory rate (18/min), and oxygen saturation (95%). Physical findings included a supple neck without masses or lymphadenopathy, regular cardiac rhythm without murmurs, clear lung fields, and a soft, nontender abdomen. No focal neurological deficits were noted. Laboratory investigations revealed marked leukocytosis (20.8 × 10^9^/L) with neutrophilia (89.9%) (Figure 1), elevated C-reactive protein (43.1 mg/L), consistent with an inflammatory or infectious process (Table 1).
Trend of white blood cell count (×109/L) during hospitalization
Initial imaging with computed tomography (CT) demonstrated a linear radiopaque FB, consistent with a fish bone approximately 2.3 cm in length, penetrating the esophageal wall at the level of the T3 vertebral body (Figure 2). The posterior tip abutted the wall of the proximal descending thoracic aorta, with associated esophageal wall thickening, periesophageal edema, but no definite abscess or pneumomediastinum.
CT scan demonstrated a linear radiopaque foreign body (#2.3 cm), consistent with a fish bone (white arrows)CT: computed tomographyThe object was located at the level of the T3 vertebra, and the posterior end pointed toward the descending aorta. Associated esophageal wall thickening and periesophageal edema were noted. No definite abscess or pneumomediastinum was demonstrated. (A) Axial plane, (B) coronal plane. White arrows (A and B panels) demonstrated the fish bone
Esophagogastroduodenoscopy confirmed the fish bone perforating the esophagus at approximately 20 cm from the incisors, with surrounding mucosal inflammation and edema (Figure 3). The bone was successfully removed endoscopically without complication. Mild antral gastritis was noted incidentally. Afterward, she was treated with broad-spectrum intravenous antibiotics (ertapenem and vancomycin) for suspected mediastinitis. Routine follow-up imaging (four days later) showed resolution of the FB but development of a small pseudoaneurysm (depth 4 mm, length 10 mm) in the proximal descending thoracic aorta at the site of prior penetration (Figure 4), with persistent mediastinal inflammation, periaortic fluid, and enhancing plaques indicative of inflammation.
EGD demonstrated a fish bone (black arrows in (A) and (B)) perforating esophageal wall about 20 cm from the incisors. It was successfully removed endoscopically (C) without any complicationsEGD: esophagogastroduodenoscopy(A) and (B) Fish bone was visualized from different angles, and inflammation of the surrounding mucosa was noted. (C) Fish bone after removal. Black arrows (A, B, and C panels) demonstrated the fish bone
CT scan demonstrated a pseudoaneurysm (white arrows) at the previous location of the fish bone (at the level of T3 vertebra), measuring 4 mm × 10 mmCT: computed tomography; CTA: computed tomography angiographyMild bilateral pleural effusion was noted. (A) and (B), coronal and axial planes; (C), CTA volume-rendered reconstruction. The white arrow (A, B, and C panels) demonstrated the aortic pseudoaneurysm
Given the high risk of rupture, the patient underwent urgent thoracic endovascular aortic repair (TEVAR) with deployment of a covered stent-graft to exclude the pseudoaneurysm. Intraoperative angiography revealed unintentional partial coverage of the left common carotid artery origin by the proximal stent edge. To preserve cerebral perfusion, immediate total aortic arch debranching was performed using an 8 mm silver-coated synthetic graft. This involved end-to-side anastomosis of the graft to the right common carotid artery and to the left common carotid artery, with proximal ligation of the left common carotid near its aortic origin and creation of a left carotid-subclavian bypass. Intraoperative cerebral oximetry remained stable throughout.
The postoperative course was uncomplicated, with resolution of symptoms and no neurological sequelae. Subsequent imaging confirmed stent-graft patency, stable mediastinal changes, and a small type II endoleak without evidence of ongoing infection or rupture. She was discharged after about two weeks. Leukocyte count decreased significantly at this time (from 20.8 × 10^9^/L on admission to 14.1 × 10^9^/L at day 16). She was transitioned to prolonged oral antibiotic therapy for a total duration of four weeks. At follow-up three months later, the patient remained asymptomatic with excellent functional recovery (Figure 5).
Important milestones during patient managementCT: computed tomography; TEVAR: thoracic endovascular aortic repair
Discussion
EFBs, particularly fish bones, are common in Asian countries due to dietary habits involving frequent fish consumption [10,11]. In a retrospective study including 427 cases of EFB in China, Ruan reported that 46.4% of cases were due to fish bones and 26.5% to poultry bones [12]. EFBs represent a relatively common presentation in emergency departments, often manifesting as acute dysphagia, inability to swallow saliva, or retrosternal pain [1,12]. EFBs may occur at all levels of the hypopharynx or in the upper portion of the esophagus, potentially due to the lower pressure in the transition zone between striated and smooth muscle fibers [3]. Sharp and pointed objects, such as fish bones, may penetrate the esophageal wall, leading to serious complications, including cervical abscess, mediastinitis, pneumonia, pneumothorax, tracheoesophageal fistula, and, rarely, major vascular injuries such as AEF or AP [7,13,14]. Therefore, when EFBs, especially sharp objects, are suspected, prompt endoscopic evaluation and removal are recommended to minimize complications, morbidity, and mortality [15].
Evaluation of a patient with suspected EFBs should include careful history taking and physical examination [5,16]. The European Society of Gastrointestinal Endoscopy (ESGE) recommended plain radiography for suspected radiopaque objects or when the type of FBs is unknown [16]. A CT scan is recommended in cases of suspected perforation or other complications, which may require surgery [16]. Many swallowed FBs may appear radiolucent on plain radiographs, including fish and chicken bones, plastic, and wood [17]. In these cases, secondary radiographic signs such as prevertebral cervical swelling on a lateral cervical X-ray can suggest the presence of FB in an appropriate setting if it’s consistent with the history [17]. CT scan has been shown to have high sensitivity and specificity (99.8% and 100%) to detect FBs in the upper GI tract, as well as in the detection of fish bones [18,19]. It was also demonstrated to be superior to plain X-rays (sensitivity and specificity of 51.2% and 99.5%, respectively) [19]. Thus, CT scan is considered the first-line imaging modality for radiolucent FBs and a second-line modality when plain X-rays are negative for radiopaque cases; however, clinical suspicion remains high for impacted FBs [19].
The diagnostic algorithm for suspected EFBs has evolved regarding the threshold for cross-sectional imaging, though plain radiography remains the universal initial screen [5,16,20]. While all major guidelines agree that biplane radiography is effective for radiopaque objects, there are some differences in how they manage radiolucent ingestions (Table 2). The 2011 guidelines of the American Society for Gastrointestinal Endoscopy (ASGE) suggested that while CT may be useful, it is not definitive, and persistent symptoms mandate endoscopic evaluation even in the setting of negative imaging [5]. In contrast, the 2016 guidelines of the ESGE provide a more quantitative warning regarding the limitations of plain films, explicitly noting a sensitivity of only 32% for detecting fish bones, and report a CT sensitivity of 90%-100% for these cases [16]. From a radiology standpoint, Guelfguat et al. advocate for the aggressive utilization of CT, citing a sensitivity of up to 100% for sharp FBs such as fish bones. Consequently, the take-home point for clinical practice is that a negative plain X-ray is insufficient to exclude FB impaction due to soft tissue obscuration, especially in cases of high clinical suspicion [20]. Current practice increasingly aligns with this radiological perspective, favoring early CT utilization to prevent missed diagnoses of these types of FBs [20].
Historically, AP and AEF secondary to FB ingestion carried a high mortality rate under conservative management, largely due to rapid progression to exsanguination and mediastinal sepsis [9,21]. AEF is an extremely rare entity in a scenario of ingested FBs, with the incidence of less than 0.1% [8]. In a study of 2394 cases of ingested FBs by Nandi et al. [8], only two cases of AEF were reported. In another study of 1338 cases of FBs conducted by Lai et al. [22], none was reported to have AEF.
Regarding treatment, two main approaches include endoscopy and surgery. However, 90% of all cases of ingested FBs will pass spontaneously. About 10%-20% of those FBs can be removed endoscopically, and 1% of all cases require surgery [23]. Endoscopy is the main intervention to remove EFBs, including both flexible endoscopy (FE) and rigid endoscopy (RE). FE is currently considered first-line therapy in the majority of EFB cases, while RE may be more suitable in a few selected cases [24]. Surgery is considered one of the last resorts when severe complications are suspected [12].
For AEF, open surgical repair (OSR) has a high mortality rate (55.5%) even in tertiary care centers [25]. Recently, TEVAR gained popularity as an emergent treatment for AEF [21]. A recent systematic review suggested TEVAR achieved a high technical success rate (87.3%) with a 30-day mortality rate of 19.4% [21]. In acute settings, TEVAR helped control bleeding and stabilize hemodynamics, thus also improved morbidity and mortality associated with OSR [21]. However, TEVAR alone will not treat an esophageal defect, and the stent graft would be exposed to a contaminated environment [21]. AEF recurrence and stent graft infection were 13.8% and 15.2%, respectively [21]. In a systematic review of 55 articles including 72 patients with AEF treated with TEVAR, Canaud et al. [21] reported that all-cause mortality was 40.2% at 7.4 months of follow-up. Prolonged antibiotic use (>4 weeks) was utilized in 80% of patients, and it was the only factor that was associated with a significantly lower incidence of aortic mortality in the multivariate analysis [21]. Due to the high risk of endograft infection and mediastinitis after TEVAR [21,26], some authors considered it as a bridging therapy for patient stabilization before definitive aortic surgery combined with esophageal or bronchial repair [27,28]. In summary, TEVAR is rarely used as a stand-alone procedure, stent-graft removal can be considered, and the esophageal lesion can be surgically addressed once the patient's condition has stabilized [26,29]. In a case of AEF caused by a chicken bone, Chen et al. [30] proposed an alternative approach including an aortic stent graft placement combined with thoracoscopic mediastinal debridement and drainage, as well as an esophageal stent placement to isolate the fistula. After 80 days, the esophageal stent was removed [30]. In this paper, we also reviewed previously reported cases of EFBs complicated by AP or AEF that were managed with endovascular stent treatment over the past two decades (2005-2026) (Table 3).
Mediastinal infection seemed to be the primary predictor of increased mortality and failure rate of TEVAR (Table 3). This is consistent with the study of Canaud et al. [21] in which the authors reported that prolonged antibiotic use was the only factor associated with a lower incidence of aortic mortality (p = 0.003). The analysis of TEVAR outcomes in this setting reveals significantly different outcomes based on the presence of infection (Table 3). In cases where deep mediastinal infection was present and not aggressively managed, TEVAR frequently served only as a temporary seal before eventual catastrophic failure. For instance, Rawala et al. [34] reported a patient who died three months post-procedure due to sepsis from an infected endovascular stent, and Kelly et al. [9] described a case where the stent became infected 51 days after insertion, necessitating high-risk explantation and definitive open surgical reconstruction. An endograft placed in an infected field acts as an FB itself; without adequate debridement, it can become a nidus for persistent infection, leading to pseudoaneurysm recurrence or fistula reformation. This failure mode was recently reinforced by Ma et al. [31], who reported treatment failure due to persistent mediastinitis despite initial sealing of TEVAR.
Conclusions
EFB is a common emergency presentation but can rarely lead to catastrophic aortic complications such as pseudoaneurysm and AEF. Early endoscopic evaluation combined with prompt cross-sectional imaging is critical for detecting esophageal perforation and identifying evolving vascular injury. This case highlights the importance of serial imaging, meticulous surgical planning, and comprehensive postoperative management in the treatment of AP secondary to FB ingestion. Current evidence supports a hybrid approach using TEVAR as initial stabilization, followed by staged definitive management when feasible, with aggressive and prolonged antibiotic therapy to control mediastinal infection. Close clinical and imaging surveillance remains essential for early detection of endograft-related complications and prompt interventions.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Esophageal emergencies: WSES guidelines World J Emerg Surg Chirica M Kelly MD Siboni S 261420193116491510.1186/s 13017-019-0245-2PMC 6544956 · doi ↗ · pubmed ↗
- 2Foreign bodies in the gastrointestinal tract Curr Opin Pediatr Wyllie R 5635641820061696917310.1097/01.mop.0000245359.13949.1c · doi ↗ · pubmed ↗
- 3Esophageal foreign bodies in adults: systematic review of the literature Scand J Gastroenterol Aiolfi A Ferrari D Riva CG Toti F Bonitta G Bonavina L 117111785320183039414010.1080/00365521.2018.1526317 · doi ↗ · pubmed ↗
- 4Management of esophageal foreign bodies: a retrospective review of 400 cases Eur J Cardio-Thorac Surg Off J Eur Assoc Cardio-Thorac Surg Athanassiadi K Gerazounis M Metaxas E Kalantzi N 65365621200210.1016/s 1010-7940(02)00032-511932163 · doi ↗ · pubmed ↗
- 5Management of ingested foreign bodies and food impactions Gastrointest Endosc Ikenberry SO Jue TL Anderson MA 108510917320112162800910.1016/j.gie.2010.11.010 · doi ↗ · pubmed ↗
- 6Case report: area of focus in a case of giant aortic arch pseudoaneurysm following fish bone penetration Front Cardiovasc Med Xiong J Cao J Yu J Li P Zeng Z Pan X 16338081220254121034410.3389/fcvm.2025.1633808 PMC 12588893 · doi ↗ · pubmed ↗
- 7Swallowed foreign bodies in adults Dtsch Arztebl Int Ambe P Weber SA Schauer M Knoefel WT 86987510920122329367510.3238/arztebl.2012.0869 PMC 3536040 · doi ↗ · pubmed ↗
- 8Foreign body in the oesophagus: review of 2394 cases Br J Surg Nandi P Ong GB 5965197862396810.1002/bjs.1800650103 · doi ↗ · pubmed ↗