Compensatory versus non-compensatory types in myopic acute acquired comitant esotropia: a new classification based on fusion ability at the far point
Yipao Li, Binjun Zhang, Luyao Tong, Na Liao, Huanyun Yu, Fang Zhang, Minghui Wan

TL;DR
This paper introduces a new classification of myopic acute acquired comitant esotropia based on fusion ability at the far point, revealing two distinct subtypes with different clinical features and potential causes.
Contribution
A novel classification system for myopic AACE based on fusion compensation at the far point, linking clinical subtypes to eye-use habits and pathogenesis.
Findings
Prolonged near gaze without myopia correction is a significant risk factor for myopic AACE.
Two subtypes of AACE—compensatory and non-compensatory—exhibit distinct clinical features and pathogenic mechanisms.
Abstract
To propose a novel classification of acute acquired comitant esotropia (AACE) with myopia based on fusion compensation ability at the far point (FP) without myopia correction (MC) and to investigate its pathogenesis in relation to eye-use habits. A retrospective case-control study. This study enrolled 105 myopic AACE patients and 107 control subjects with simple myopia. Data collected included refractive error, angle of deviation (measured by prism and alternate cover test (PACT) and Maddox prism test (MPT) at distance and near), and detailed eye-use habits. AACE patients were categorized into compensatory (n = 92) or non-compensatory (n = 13) groups based on their ability to maintain binocular fusion at the FP without MC. A total of 98.10% of AACE patients neglected MC during prolonged near gaze before onset, a rate significantly higher than controls (13.08%). The cohort was divided…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
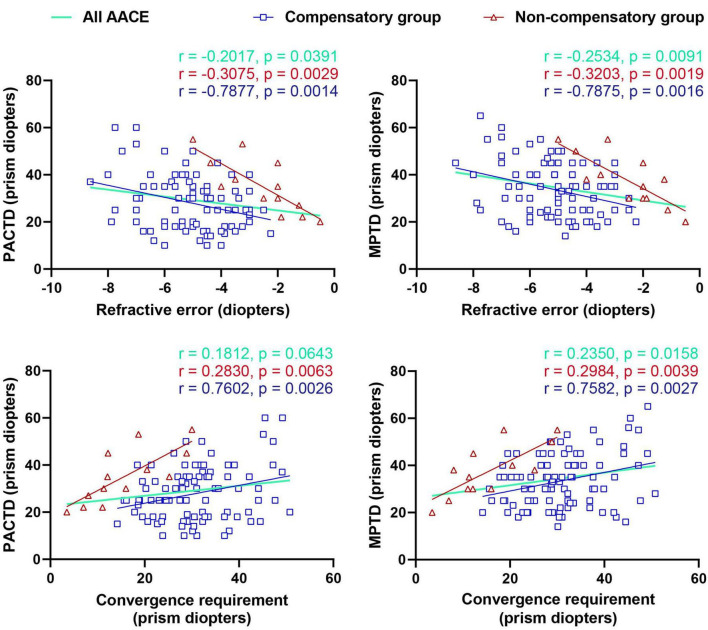 FIGURE 1
FIGURE 1| Characteristics | AACE group ( | Control group ( | 95% confidence interval | |
|---|---|---|---|---|
| Age at visit (years) | 26 (18.5, 33) | 25 (21, 29) | 1.00 (–1.00 to 3.00)†† | 0.546 |
| Age at AACE onset (years) | 23 (17, 31.7) | — | — | — |
| Sex (M: F) | 63: 42 | 55: 52 | — | 0.207 |
| Refractive error (diopters) | –4.74 ± 1.60 | –4.70 ± 1.58 | –0.04 (–0.47 to 0.39) | 0.861 |
| Rate of daily MC | 89/105 | 95/107 | — | 0.387 |
| Rate of prolonged near gaze without MC* | 103/105 | 14/107 | — | <0.001 |
| Duration of daily near gaze time (hours) | 6 (6, 8) | 6 (4, 7) | 1.00 (0.00 to 1.00)†† | 0.012 |
| Characteristics | All patients ( | Compensatory group ( | Non-compensatory group ( | 95% confidence interval | |
|---|---|---|---|---|---|
| Age at AACE onset (years) | 23 (17, 31.7) | 25 (17, 34.45) | 17 (14.5, 21) | 6.10 (1.50 to 12.00)†† | 0.015 |
| Sex (M: F) | 63: 42 | 55: 37 | 8: 5 | — | 0.904 |
| Rate of daily MC | 89/105 | 84/92 | 5/13 | — | <0.001 |
| Rate of prolonged near gaze without MC | 103/105 | 90/92 | 13/13 | — | >0.999 |
| Duration of daily near gaze time (hours) | 6 (6, 8) | 6 (6, 8) | 6 (5.5, 8) | 0.00 (–1.00 to 1.00)†† | 0.990 |
| Pupil distance (cm) | 6.16 ± 0.31 | 6.16 ± 0.31 | 6.17 ± 0.37 | –0.01 (–0.20 to 0.17) | 0.891 |
| Refractive error (diopters) | –4.74 ± 1.59 | –5.04 ± 1.39 | –2.57 ± 1.36 | –2.48 (–3.29 to –1.66) | <0.001 |
| Far point (cm) | 21.62 (17.58, 27.13) | 20 (16.67, 24.81) | 50 (26.79, 66.67) | –23.95 (–33.33 to –10.77)†† | <0.001 |
|
| |||||
| Distance | 30 (18.5, 36) | 25 (18, 35) | 35 (24.5, 45) | –7.00 (–15.00 to –0.00)†† | 0.040 |
| Near | 20 (14, 30) | 20 (12, 30) | 35 (22.5, 42.5) | –12.00 (–20.00 to –5.00)†† | 0.003 |
|
| |||||
| Distance | 35 (25, 42.5) | 33 (25, 40) | 38 (30, 47.5) | –5.00 (–10.00 to 2.00)†† | 0.195 |
| Near | 25 (18, 36) | 25 (18, 35) | 35 (30, 42.5) | –10.00 (–15.00 to –2.00)†† | 0.011 |
| PACT without MC at the FP | 0 (0, 6) | 0 (0, 4) | 15 (14, 22.5) | –14.00 (–16.00 to –14.00)†† | <0.001 |
|
| |||||
| Distance | 16/105 | 16/92 | 0/13 | — | 0.210 |
| Near | 43/105 | 43/92 | 0/13 | — | 0.001 |
|
| |||||
| Distance | 15:90 | 15:77 | 0:13 | — | 0.206 |
| Near | 51:54 | 51:41 | 0:13 | — | <0.001 |
| CRFP (prism diopters) | 29.01 (22.45, 34.53) | 30.51 (24.44, 36.90) | 12.20 (9.56, 22.84) | 15.78 (10.13 to 20.46) | <0.001 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOphthalmology and Visual Impairment Studies · Ophthalmology and Eye Disorders · Visual perception and processing mechanisms
Introduction
Acute acquired comitant esotropia (AACE) is characterized by sudden-onset, comitant esotropia, often with diplopia and preserved binocular potential (1–4). The classic Burian and Miller classification delineates three types: Type I (Swan) from fusion disruption, Type II (Burian-Franceschetti) associated with psychosomatic stress, and Type III (Bielschowsky) occurring in uncorrected myopic individuals (1). However, the rising incidence of AACE (5–9), particularly among myopic adults engaged in extensive near work (10, 11), challenges this traditional schema. Etiologies remain debated, encompassing neurological disorders (12), medial rectus muscle abnormalities (13), excessive near-work (10, 14), decompensated esophoria (15), and digital device overuse (5, 16).
A critical unresolved debate is whether uncorrected myopia during near work is an independent risk factor (3, 10, 17). While many patients routinely wear corrective lenses, their habits during prolonged near tasks are often overlooked. Furthermore, the established classification may not adequately reflect the spectrum of clinical presentations seen today.
Most myopic AACE patients retain some binocular function (7), suggesting a compensatory process might be involved in the pathogenesis. We hypothesize that the ability to maintain fusion at the far point (FP) without correction—a point requiring minimal accommodative convergence—could be a key differentiator, potentially separating patients into distinct pathogenic categories. As the FP is the natural viewing distance for uncorrected myopes and requires minimal accommodative effort, it provides a unique vantage point to assess vergence adaptation (18, 19). Assessing binocular function at this specific, ecologically relevant distance may be important for providing insights into the adaptive mechanisms underlying myopic AACE.
This study aims to investigate the pathogenesis of myopic AACE by introducing a novel classification based on fusion compensation ability at the FP and to examine its correlation with specific eye-use habits, particularly prolonged near gaze without myopia correction (MC).
Materials and methods
This retrospective study adhered to the Declaration of Helsinki and was approved by the Ethics Committee of Wenzhou Medical University (2023-190-K-155-01). Informed consent was waived due to the anonymized retrospective data.
We enrolled 105 myopic AACE patients from the Affiliated Eye Hospital of Wenzhou Medical University (Jan 2020–Nov 2023). Inclusion criteria were: (1) myopia in both eyes; (2) AACE diagnosis; (3) complete records. Exclusion criteria included: ocular surgery, trauma, neurological disorders, or best-corrected visual acuity < 18/20 in either eye. A control group of 107 simple myopia patients was recruited.
All patients underwent detailed history-taking, including: routine MC habits, MC status during prolonged near gaze (e.g., smartphone use), daily near gaze duration, and time without MC during near tasks. Near gaze refers to sustained visual tasks at close distances, typically involving focused attention. The average distance was self-reported as <30 cm for myopes.
The refractive error for each participant was defined as the mean spherical equivalent of both eyes. Ocular deviation was measured with MC using prism and alternate cover test (PACT) and Maddox prism test (MPT) at distance (6 m) and near (33 cm). The deviation at the FP without MC was also measured. Binocular vision was assessed using Titmus, OPTEC3500, Worth 4-dot, and Bagolini striated lenses tests. The the convergence requirement at the FP (CRFP) was calculated as pupillary distance (mm) / FP (meters). The Bagolini test was chosen as the primary criterion for defining fusion at the FP because it assesses fusion under natural viewing conditions without artificial dissociation, closely simulating the state during uncorrected near work (20, 21). Conventional dissociative tests (e.g., Worth four-dot), while used complementarily at standard distances, are less suitable for evaluating the specific physiological condition at the FP (22).
AACE patients were divided into two groups based on the Bagolini test at the FP without MC: those maintaining fusion were assigned to the compensatory group; those who could not were assigned to the non-compensatory group. The FP was chosen as the diagnostic criterion due to its unique distance, allowing clear vision with minimal accommodative-convergence demand in uncorrected myopia. Fusion at the FP reflects compensation for esodeviation and thus functions as a classification marker.
Statistical analyses were performed using Graphpad Prism 9.4.1. Group comparisons used t-tests, Mann-Whitney U tests, chi-square tests, or Fisher’s exact tests. Correlations were assessed using Spearman’s rank coefficient. A p-value < 0.05 was significant.
Results
Baseline characteristics and eye-use habits
The study included 105 AACE patients and 107 controls. The baseline characteristics were comparable between the two groups (Table 1). The median age of AACE patients was 26 years (interquartile range [IQR]: 18.5–33), while that of the controls was 25 years (IQR: 21–29), with no significant difference (P = 0.546). Regarding refractive error, the spherical equivalent was −4.74 ± 1.60 D in AACE patients and −4.70 ± 1.58 D in controls (P = 0.861). No significant difference was found in the rate of routine MC between groups (84.76% vs. 88.79% P = 0.387). However, the AACE group had a significantly higher rate (98.10% vs. 13.08%, P < 0.001) of near gaze without MC. Additionally, refractive error showed significant correlations with both PACTD and MPTD in the entire AACE cohort, as well as in both the compensatory and non-compensatory subgroups (all P < 0.05, Figure 1). Additionally, the AACE subgroups were compared with control group (Supplementary Tables 1, 2).
Correlation of refractive error and convergence requirement at far point (CRFP) with distance deviation (PACTD and MPTD) in all AACE patients, the compensatory group, and the non-compensatory group. AACE, acute acquired comitant esotropia; PACTD, prism and alternate cover test at distance; MPTD, Maddox prism test at distance.
Characteristics of the compensatory and non-compensatory groups
Based on the presence of fusion at the FP without MC, patients were categorized into compensatory (n = 92, 87.62%) and non-compensatory (n = 13, 12.38%) groups (Table 2).
The compensatory group exhibited a consistent pattern wherein the MPT was significantly greater than the PACT at both distance and near fixation (P < 0.001), and both the MPT and PACT values were significantly larger at distance than at near (P < 0.001). Notably, the PACT measurement at the FP without MC was 0 PD (IQR: 0–4 PD). In contrast, the non-compensatory group demonstrated a different profile: MPT was not greater than PACT at distance and near fixation (P > 0.05), with no significant difference observed between distance and near deviations in both MPT and PACT (P > 0.05). Furthermore, this non-compensatory group showed a significantly larger PACT at the FP without MC, measuring 15 PD (IQR: 14–22.5 PD, Table 2).
Comparative analysis revealed that relative to the compensatory group, the non-compensatory group was characterized by a significantly younger onset age (median 17 vs. 25 years, P = 0.015), a lower daily rate of MC (P < 0.001), lower refractive error (mean −2.57 vs. −5.04 D, P < 0.001), larger angles of deviation (P < 0.05), worse near fusion (Worth 4-dot, P = 0.001), worse near stereopsis (P < 0.001), and a lower convergence requirement at the FP (CRFP, P < 0.001, Table 2).
The far point distance, measured objectively, was significantly closer in the compensatory group (median [IQR]: 20 [16.67, 24.81] cm) compared to the non-compensatory group (median [IQR]: 50 [26.79, 66.67] cm) (P < 0.001). This finding is consistent with the calculated CRFP values. Given that pupillary distance was similar between groups (P = 0.891), the markedly higher CRFP in the compensatory group directly results from their closer far point, indicating a substantially increased convergence requirement even for distant fusion.
Relationship and comparison of CRFP with deviation measures
In the compensatory group, CRFP was positively correlated with both MPTD and PACTD (P < 0.05). CRFP was significantly greater than PACTD (P = 0.019), but not significantly different from MPTD (P = 0.054). In the non-compensatory group, CRFP was positively correlated with MPTD and PACTD (P < 0.001) but was significantly lower than both (P < 0.001, Figure 1).
Discussion
Our study introduces a novel, clinically relevant classification for myopic AACE based on the presence of fusion compensation at the FP without MC. This approach successfully identified two distinct subgroups with significantly different clinical profiles, suggesting potentially divergent pathogenic mechanisms.
The overwhelmingly high rate of neglected MC during prolonged near work (98.10%) in AACE patients, contrasted with similar routine MC rates to controls, underscores that the critical risk factor is not myopia per se, but long-time near work without MC. This aligns with emerging literature on digital eye strain and AACE and offers a clear target for prevention: emphasizing consistent spectacle wear during all near tasks.
The compensatory group, representing the majority, is characterized by a larger deviation at distance relative to near, higher MPTD values relative to PACTD, and orthophoria at the FP without MC. The strong positive correlation between CRFP and deviation, and the near-equivalence of CRFP and MPTD, provides compelling evidence that the esodeviation in these patients may represent a maladaptive compensation for the excessive convergence demand incurred during uncorrected near gaze. Our direct measurement of the far point distance offers further support for this pathogenesis. The significantly closer far point in the compensatory group explains their elevated CRFP and indicates that their vergence system is maintained at a high tonic level, even under minimal accommodative demand at distance. This objective finding substantiates the concept of a system chronically adapted to excessive convergence. We postulate a mechanism: sustained voluntary convergence may overload the medial rectus muscles, potentially leading to adaptations such as contracture or hypertonia. The greater distance deviation may be attributed to insufficient relaxation of the tonically contracted medial recti muscles as convergence demand decreases. Nevertheless, patients’ retained fusional divergence ability may partially overcome this tone to maintain single binocular vision. Esotropia is thus revealed under dissociative conditions that break fusion. Future studies utilizing high-resolution orbital magnetic resonance imaging to quantify medial rectus muscle morphology, or employing electromyography to assess muscle activity, may be warranted to objectively test this hypothesis regarding muscle contracture and hypertonia.
Conversely, the non-compensatory group, with its younger age, lower myopia, larger angles, and absence of the classic deviation pattern, likely embodies a different pathophysiology. The inability to fuse even at the FP indicates a failure of compensatory mechanisms, possibly representing a decompensated esophoria (15) or a more profound disruption of vergence neural integration. This classification may help inform clinical management. It highlights the potential risk of deviation underestimation by conventional cover testing in compensatory patients, which might be attributed to fusional compensation. This suggests a potential need for supplemental tests (e.g., Maddox rod) to better determine the surgical target. These findings also lend support to the consideration of augmented surgical doses, as suggested in prior studies (23), which could potentially reduce the risk of under-correction and recurrence. Furthermore, the classification might offer guidance for postoperative strategies, such as considering binocular training for compensatory patients and alternative rehabilitation approaches for non-compensatory patients, thereby promoting a more personalized therapeutic framework.
Our proposed classification system can be contextualized within the historical framework of AACE subtypes. The non-compensatory group appears to share several characteristics with the acute-onset, fusion-disruptive types in the classic Burian-Miller classification (Types I and II). Similarly, the compensatory group may partially correspond to the traditional Type III (Bielschowsky), which has been associated with uncorrected myopia (1). However, our framework aims to build upon these classical descriptions by introducing a mechanism-based dichotomy centered on convergence adaptation at the far point. A key distinction lies in our focus on the ability to maintain fusion at this specific distance—a physiological marker not central to the classical system. This perspective may provide a more nuanced explanation for the clinical profile of a substantial proportion of contemporary AACE patients and could offer a basis for future subtyping research across the broader AACE spectrum.
This binary classification addresses limitations of the traditional Burian system. It provides a physiological basis for subtyping modern AACE cases and provides a potential explanation for clinical variations that confuse the existing schema. For example, the non-compensatory group’s features do not neatly fit into any classic type. From a clinical standpoint, this classification is pragmatic. Assessing fusion at the FP is simple and informs prognosis (compensatory likely better) and surgical planning, potentially explaining why surgery based on PACT measurements sometimes requires augmentation (23).
This study has limitations primarily stemming from its retrospective design and data collection methods. The reliance on patient-reported questionnaires for eye-use habits introduces the potential for recall bias. Furthermore, the retrospective nature limits causal inference and control for confounders. Future prospective studies incorporating objective measures of near-work behavior (e.g., using wearable sensors) are essential to validate our proposed classification and confirm these associations.
Conclusion
Prolonged near gaze without myopia correction is a paramount risk factor for AACE. Classifying myopic AACE patients based on their fusion compensation ability at the far point reveals two distinct subtypes with different clinical characteristics. The compensatory type appears to be an abnormal adaptation to excessive convergence demand in myopia without MC during near tasks, while the non-compensatory type suggests a decompensated mechanism. This new classification system not only enhances our understanding of the pathogenesis but also provides a practical framework for clinical assessment and management.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Burian H Miller J. Comitant convergent strabismus with acute onset. Am J Ophthalmol. (1958) 45:55–64. 10.1016/0002-9394(58)90223-x 13520873 · doi ↗ · pubmed ↗
- 2Clark A Nelson L Simon J Wagner R Rubin S. Acute acquired comitant esotropia. Brit J Ophthalmol. (1989) 73:636–8. 10.1136/bjo.73.8.636 2765443 PMC 1041834 · doi ↗ · pubmed ↗
- 3Chen J Deng D Sun Y Shen T Cao G Yan J Acute acquired concomitant esotropia: clinical features, classification, and etiology. Medicine. (2015) 94:e 2273. 10.1097/MD.0000000000002273 26705210 PMC 4697976 · doi ↗ · pubmed ↗
- 4Spierer A. Acute concomitant esotropia of adulthood. Ophthalmology. (2003) 110:1053–6. 10.1016/S 0161-6420(03)00102-7 12750113 · doi ↗ · pubmed ↗
- 5Okita Y Kimura A Masuda A Mochizuki Y Kondo M Yamadera K Yearly changes in cases of acute acquired comitant esotropia during a 12-year period. Graefe’s Arch Clin Exp Ophthalmol. (2023) 261:2661–8. 10.1007/s 00417-023-06047-8 37067584 PMC 10107582 · doi ↗ · pubmed ↗
- 6Zhu M Tang Y Wang Z Shen T Qiu X Yan J Clinical characteristics and risk factors of acute acquired concomitant esotropia in last 5 years: a retrospective case-control study. Eye. (2023) 37:320–4. 10.1038/s 41433-022-01939-1 35075284 PMC 9873604 · doi ↗ · pubmed ↗
- 7Mohan A Sen P Mujumdar D Shah C Jain E. Series of cases of acute acquired comitant esotropia in children associated with excessive online classes on smartphone during COVID-19 pandemic; digital eye strain among kids (DESK) study-3. Strabismus. (2021) 29:163–7. 10.1080/09273972.2021.1948072 34223812 · doi ↗ · pubmed ↗
- 8Neena R Remya S Anantharaman G. Acute acquired comitant esotropia precipitated by excessive near work during the COVID-19-induced home confinement. Indian J Ophthalmol. (2022) 70:1359–64. 10.4103/ijo.IJO_2813_21 35326055 PMC 9240503 · doi ↗ · pubmed ↗