Exploring the mediating role of psychological resilience between social support and anxiety in nurses: a cross-sectional study in Chengdu, Sichuan, China
Junyi Hou, Mingzhu Song, Hui Li, Xinlin Miao, Xia Wang, Yesha Liu, Jianfeng Sun, Chan Huang

TL;DR
This study explores how psychological resilience connects social support and anxiety in Chinese nurses, finding that resilience partially mediates this relationship.
Contribution
The novel contribution is identifying psychological resilience as a partial mediator between social support and anxiety in nurses.
Findings
35.7% of nurses reported anxiety, with social support and resilience negatively correlated with anxiety.
Psychological resilience partially mediates the relationship between social support and anxiety, accounting for 21% of the total effect.
Subjective support's impact on anxiety is 41% mediated by psychological resilience.
Abstract
Nurse anxiety is a significant public health issue that impacts individual well-being, healthcare system stability, service quality, and patient safety. This study aimed to assess anxiety levels among Chinese nurses and to investigate the association between social support and anxiety, specifically examining the potential mediating role of psychological resilience. The findings are intended to enhance the understanding of mental health mechanisms and inform targeted interventions for nurses. A cross-sectional online survey was conducted from February to April 2025 with 1,133 nursing staff in Sichuan Province, China, using stratified and snowball sampling. Participants completed the Self-Rating Anxiety Scale (SAS), Social Support Rating Scale (SSRS), and Connor-Davidson Resilience Scale (CD-RISC). Data were analyzed using t-tests, ANOVA, Bayesian Estimates, Pearson correlation, and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
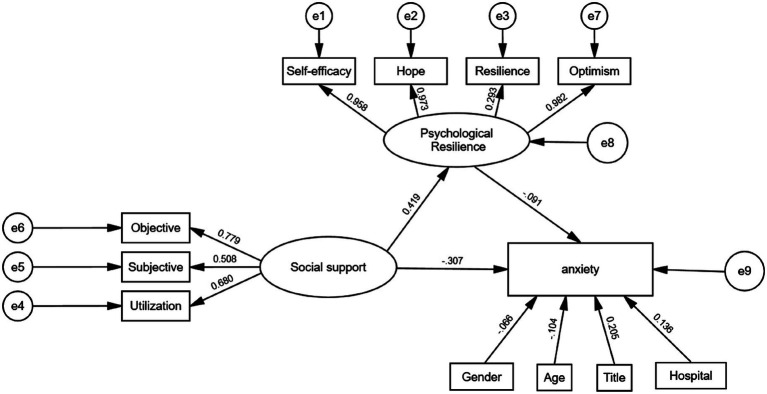 Figure 1
Figure 1 Figure 2
Figure 2| Individual characteristics | Sample size, | Participants with anxiety, | Anxiety score, x̅ ± s | Lower bound† | Upper bound |
| ||
|---|---|---|---|---|---|---|---|---|
| Gender | Male | 230 | 124 (53.9) | 41.04 ± 8.24 | 39.99 | 42.08 | 4.963 | <0.001* |
| Female | 903 | 280 (31) | 38.07 ± 8.04 | 37.55 | 38.60 | |||
| Age (years) | <22 | 71 | 36 (50.7) | 42.62 ± 10.06 | 40.73 | 44.51 | 6.042 | <0.001* |
| [22, 25) | 421 | 149 (35.4) | 38.29 ± 9.19 | 37.52 | 39.07 | |||
| [25, 30) | 458 | 168 (36.7) | 38.53 ± 7.54 | 37.79 | 39.28 | |||
| ≥30 | 183 | 51 (27.9) | 38.37 ± 5.61 | 37.20 | 39.55 | |||
| Nursing experience (years) | <3 | 459 | 179 (39) | 40.05 ± 8.89 | 39.31 | 40.79 | 8.041 | <0.001* |
| [3, 5) | 301 | 94 (31.2) | 37.28 ± 8.67 | 36.36 | 38.19 | |||
| [5, 10) | 232 | 91 (39.2) | 37.99 ± 6.43 | 36.95 | 39.03 | |||
| ≥10 | 141 | 40 (28.4) | 38.32 ± 6.27 | 36.98 | 39.66 | |||
| Professional title | Primary | 883 | 286 (32.4) | 38.07 ± 8.20 | 37.54 | 38.60 | 11.419 | <0.001* |
| Intermediate | 225 | 108 (48) | 40.92 ± 7.72 | 39.87 | 41.98 | |||
| Senior | 25 | 10 (40) | 39.80 ± 7.14 | 36.63 | 42.97 | |||
| Education | Secondary nursing education or below | 31 | 5 (16.1) | 37.65 ± 5.12 | 34.77 | 40.52 | 0.292 | 0.747 |
| Associate degree | 668 | 235 (35.2) | 38.76 ± 8.07 | 38.14 | 39.38 | |||
| Bachelor’s degree or above | 434 | 164 (37.8) | 38.62 ± 8.48 | 37.85 | 39.39 | |||
| Hospital level | Grade 3 (3A/3B) | 728 | 215 (29.5) | 37.41 ± 7.83 | 36.83 | 37.98 | 30.027 | <0.001* |
| Grade 2 (2A/2B) | 190 | 111 (58.4) | 42.17 ± 8.88 | 41.04 | 43.30 | |||
| Other | 215 | 78 (36.3) | 39.88 ± 7.53 | 38.82 | 40.95 | |||
| Night shift duty | Yes | 896 | 332 (37.1) | 38.73 ± 8.43 | 38.21 | 39.28 | 0.553 | 0.58 |
| No | 237 | 72 (30.4) | 38.41 ± 7.05 | 37.37 | 39.45 | |||
| Marital status | Unmarried/divorced | 732 | 274 (37.4) | 38.76 ± 8.54 | 38.16 | 39.35 | 0.211 | 0.646 |
| Married | 401 | 130 (32.4) | 38.52 ± 7.43 | 37.72 | 39.32 | |||
| Parental status | One child | 203 | 66 (32.5) | 37.67 ± 7.25 | 36.54 | 38.79 | 2.439 | 0.063 |
| Two children | 73 | 25 (34.2) | 38.96 ± 5.44 | 37.09 | 40.83 | |||
| Married, no children | 125 | 40 (32) | 40.15 ± 8.79 | 38.72 | 41.58 | |||
| Unmarried, no children | 732 | 273 (37.3) | 38.67 ± 8.48 | 38.08 | 39.26 | |||
| Variables | Anxiety | Objective support | Subjective support | Support utilization | Total social support score |
|---|---|---|---|---|---|
| Anxiety | 1 | −0.277** | −0.126** | −0.306** | −0.283** |
| Objective support | −0.277** | 1 | 0.427** | 0.526** | 0.831** |
| Subjective support | −0.126** | 0.427** | 1 | 0.307** | 0.799** |
| Support utilization | −0.306** | 0.526** | 0.307** | 1 | 0.703** |
| Total social support score | −0.283** | 0.831** | 0.799** | 0.703** | 1 |
| Variables | Anxiety | Self-efficacy | Hope | Resiliency | Optimism | Total psychological resilience score |
|---|---|---|---|---|---|---|
| Anxiety | 1 | −0.186** | −0.224** | −0.285** | −0.239** | −0.260** |
| Self-efficacy | −0.186** | 1 | 0.933** | 0.302** | 0.940** | 0.963** |
| Hope | −0.224** | 0.933** | 1 | 0.278** | 0.955** | 0.963** |
| Resiliency | −0.285** | 0.302** | 0.278** | 1 | 0.281** | 0.464** |
| Optimism | −0.239** | 0.940** | 0.955** | 0.281** | 1 | 0.966** |
| Psychological resilience | −0.260** | 0.963** | 0.963** | 0.464** | 0.966** | 1 |
| Variables | Total social support score | Objective support | Subjective support | Support utilization | Total psychological resilience score | Self-efficacy | Hope | Resiliency | Optimism |
|---|---|---|---|---|---|---|---|---|---|
| Total social support score | 1 | 0.831** | 0.799** | 0.703** | 0.361** | 0.327** | 0.329** | 0.231** | 0.350** |
| Objective support | 0.831** | 1 | 0.427** | 0.526** | 0.318** | 0.285** | 0.282** | 0.235** | 0.299** |
| Subjective support | 0.799** | 0.427** | 1 | 0.307** | 0.228** | 0.221** | 0.203** | 0.124** | 0.225** |
| Support utilization | 0.703** | 0.526** | 0.307** | 1 | 0.328** | 0.277** | 0.318** | 0.200** | 0.324** |
| Total psychological resilience score | 0.361** | 0.318** | 0.228** | 0.328** | 1 | 0.963** | 0.963** | 0.464** | 0.966** |
| Self-efficacy | 0.327** | 0.285** | 0.221** | 0.277** | 0.963** | 1 | 0.933** | 0.302** | 0.940** |
| Hope | 0.329** | 0.282** | 0.203** | 0.318** | 0.963** | 0.933** | 1 | 0.278** | 0.955** |
| Resiliency | 0.231** | 0.235** | 0.124** | 0.200** | 0.464** | 0.302** | 0.278** | 1 | 0.281** |
| Optimism | 0.350** | 0.299** | 0.225** | 0.324** | 0.966** | 0.940** | 0.955** | 0.281** | 1 |
| Variables | Anxiety (model 1) | Psychological resilience (model 2) | Anxiety (model 3) |
|---|---|---|---|
| Constant | 55.102** (19.126) | 114.574** (11.957) | 60.973** (20.222) |
| Age (year) | −0.171 (−2.079) | −0.439 (−1.602) | −0.194 (−2.383) |
| Professional title | 0.287** (1.734) | 0.728* (1.321) | 0.324** (1.986) |
| Hospital level | 1.437** (4.757) | −7.931** (−7.894) | 1.031** (3.369) |
| Nurses’ social support | −0.313** (−9.429) | 1.295** (11.722) | −0.247** (−7.116) |
| Nurses’ psychological resilience | −0.051** (−5.798) | ||
| 0.124 | 0.196 | 0.150 | |
|
|
| Analysis path | Meaning | Effect size | 95% confidence interval | z/ |
| |
|---|---|---|---|---|---|---|
| Lower limit | Upper limit | |||||
| Social support → psychological resilience → anxiety | Indirect effect | −0.066 | −0.080 | −0.038 | −6.297 | <0.001 |
| Social support → psychological resilience | X → M | 1.295 | 1.078 | 1.511 | 11.722 | <0.001 |
| Psychological resilience → anxiety | M → Y | −0.051 | −0.069 | −0.034 | −5.798 | <0.001 |
| Social support → anxiety | Direct effect | −0.247 | −0.315 | −0.179 | −7.116 | <0.001 |
| Social support → anxiety | Total effect | −0.313 | −0.378 | −0.248 | −9.429 | <0.001 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHealthcare professionals’ stress and burnout · Resilience and Mental Health · Nursing education and management
Introduction
1
The mental health of healthcare professionals is critical to the resilience of the public health system (1). As a core component of the healthcare workforce, nurses experiencing high anxiety levels not only jeopardize their own well-being but also pose a significant threat to patient safety and care quality, making this a pressing public health issue (2). Globally, stress related to clinical practice affects approximately one-third of nurses (3). Tasked with providing high-quality care, nurses face considerable psychological stressors, including long working hours, shift rotations, exposure to patient suffering, and workplace violence (4, 5). These demands render nurses more susceptible to depression, anxiety, and burnout compared to other professional groups (6), ultimately impairing work efficiency, clinical performance, and the stability of the healthcare system (7).
Anxiety is among the most prevalent psychological issues reported by clinical nurses (8). Recent studies highlight the global scale of this challenge: in the United States, approximately 30% of nurses experience moderate to severe anxiety (9), with burnout studies indicating anxiety as a major component affecting up to 41.5% of hospital nurses (10). Survey from Japan reveals anxiety symptoms in about 24.2% of nurses (11). In China, a recent study of 7,114 nurses found an anxiety prevalence of 29.03% (12), which escalated to 46% among 4,188 nurses surveyed amid the COVID-19 pandemic (13). This persistent anxiety crisis not only threatens nursing workforce stability but also challenges the sustainable development of healthcare systems worldwide, underscoring the urgent need to identify protective factors and intervention pathways.
Drawing on the stress-buffering model (14), we hypothesize that the effect of social support on anxiety is mediated by psychological resilience. The underlying rationale is that social support does not neutralize anxiety directly (15). Rather, we propose that it first fosters the development of psychological resilience. This internalized resource then empowers nurses to better manage stressors, thereby reducing anxiety. Social support refers to the psychological, informational, and material resources that individuals obtain through social connections, which may help them cope with stress (16). Evidence suggests that enhancing social support is an effective strategy for mitigating psychological symptoms, buffering occupational stress, and reducing emotional distress among healthcare workers (17, 18). For instance, one study indicated that nurses with lower levels of social support were nearly twice as likely to experience anxiety symptoms compared to those with adequate support (19). However, the specific mechanisms underlying this protective effect require further elucidation. Psychological resilience—defined as the capacity to adapt and recover from adversity (20)—is a well-established protective factor against anxiety and depression (21). Empirical studies confirm that resilience-focused interventions can significantly reduce anxiety and stress among nurses (22). Critically, social support and psychological resilience are closely associated. Beyond directly alleviating distress, social support may also enhance an individual’s ability to cope with stress by fostering psychological resilience (23). Research suggests a positive correlation between the two, with potential synergistic effects strengthening emotional protection (24). This suggests that psychological resilience may act as a potential mediator, indicating that the protective effect of social support against anxiety is partly achieved by enhancing psychological resilience.
Nevertheless, the interrelationships between these constructs merit deeper investigation. Social support is best understood as an external resource, in contrast to psychological resilience, which is an intrinsic characteristic (25). The theoretical pathway explored in this study therefore investigates how external social resources (i.e., social support) contribute to the accumulation of internal psychological resources (i.e., psychological resilience), thereby helping to preserve core mental health resources and reduce manifestations of anxiety.
This study proposes that psychological resilience mediates the relationship between social support and anxiety among nurses. We aim to verify this mediating effect, determine its type and magnitude, and provide evidence for targeted mental health interventions. The findings are expected to help nurses better manage workplace stress, enhance their psychological well-being, and improve their overall quality of life.
Methods
2
Study design and participants
2.1
This cross-sectional survey was carried out from February to April 2025. The study population comprised registered clinical nurses with a minimum of 1 year of experience, directly engaged in patient care at hospitals in Chengdu, Sichuan Province, China. Individuals in purely administrative, teaching, or research roles were excluded from participation.
Participants were recruited through a process of stratified random sampling followed by snowball sampling: hospitals in Chengdu’s five main urban districts were first stratified by region and then by type (comprehensive, specialized, community) to select six representative hospitals, from which eligible nurses were subsequently recruited via snowball sampling.
The minimum required sample size was calculated a priori using the formula for cross-sectional studies: (26). Based on a preliminary survey (n = 100) indicating an anxiety prevalence (P) of 35%, and with Z (the Z-statistic for a 95% confidence interval) set at 1.96, the margin of error (d) was set to 15% of P (d = 0.0525). This calculation yielded a minimum required sample size of 833 participants.
An online survey was administered through hospital-affiliated QQ and WeChat groups. Participants received a detailed description of the study’s purpose, along with assurances of anonymity and confidentiality, before providing informed consent. Of the 1,166 questionnaires collected, 33 were excluded due to incomplete data on the primary scales (anxiety, social support, psychological resilience) or key demographic variables, resulting in 1,133 valid responses for the final analysis.
Measurement scales
2.2
Measurement of anxiety
2.2.1
The anxiety levels of nursing staff were assessed using the Self-Rating Anxiety Scale (SAS), a widely recognized instrument developed by Zung (27). It includes 20 items: nervousness, fear, panic, a sense of losing control, a premonition of misfortune, hand and foot trembling, headache, fatigue, restlessness, palpitations, dizziness, a feeling of fainting, dyspnea, paresthesia of the hands and feet, stomachache and indigestion, frequent urination, hyperhidrosis, facial flushing, sleep disturbance, and nightmares. Each item is rated on a 4-point Likert scale ranging from 1 (“Rarely”) to 4 (“Most of the time”). Five items (5, 9, 13, 17, and 19) are reverse-scored. Before calculating the total score, responses to these items are recoded (1 → 4, 2 → 3, 3 → 2, 4 → 1). The sum of all 20 items yields the total anxiety score, with a score above 40 indicating an anxious state. Higher scores reflect more severe anxiety symptoms. We report the Cronbach’s α for all scales in the Supplementary Figures S4–S6.
Measurement of social support
2.2.2
Social support was assessed using the Social Support Rating Scale (SSRS) (28), which is based on the 27-item Social Support Questionnaire (SSQ) developed by Sarason et al. (29) and has been adapted to be more suitable for the Chinese context. The scale consists of 10 items, which are categorized into three dimensions: objective support (3 items), subjective support (4 items), and utilization of social support (3 items). The total score ranges from 12 to 66 points: scores ≤22 indicate low social support, scores between 23 and 44 indicate moderate social support, and scores >44 indicate high social support. The higher the score, the higher the level of social support.
Measurement of psychological resilience
2.2.3
Nurses’ psychological resilience was assessed using the Connor-Davidson Resilience Scale (CD-RISC). Although the original scale contains 25 items and has demonstrated high reliability (Cronbach’s α = 0.89) (30), exploratory factor analysis conducted during our preliminary survey supported a four-factor structure more consistent with the characteristics of the Chinese sample (Supplementary Figures S1–S3). Accordingly, the scale was interpreted using four dimensions: self-efficacy, resiliency, optimism, and hope. Items were rated on a 5-point Likert scale ranging from 0 (“never”) to 4 (“almost always”). Total scores range from 0 to 100, with higher scores indicating greater psychological resilience.
Statistical methods
2.3
After preliminary assessment via histograms confirmed that anxiety, social support, and psychological resilience scores were approximately normally distributed, these variables were described using means and standard deviations (Mean ± SD). Differences in anxiety levels across categorical variables—such as age, years of nursing experience, professional title, education level, and hospital level—were examined using one-way analysis of variance (ANOVA), while an independent samples t-test was used to compare anxiety between nurses who worked night shifts and those who did not. Following significant ANOVA results, post-hoc pairwise comparisons were examined using Bayesian 95% credible intervals. Separately, Pearson’s correlation analysis was used to evaluate the bivariate correlations among anxiety, social support, and psychological resilience. Structural Equation Modeling (SEM) was conducted using AMOS 28.0.
To examine the mediating role of psychological resilience in the relationship between social support and anxiety, a series of linear regression models were constructed following the three-step procedure outlined by Baron and Kenny (31). The significance and type of mediation were further verified using the bootstrap method (32). All analyses were conducted in IBM SPSS Statistics 25.0 with the PROCESS macro (v4.0) by Hayes (33, 34), adopting a two-tailed significance level of α = 0.05.
Results
3
Demographic characteristics
3.1
The study included 1,133 nursing staff with a mean age of 25.8 ± 4.4 years (range: 18–60). All participants had at least 1 year of nursing experience, with a mean duration of 4.2 ± 3.6 years (range: 1–20). The sample’s anxiety level, measured by the SAS, showed a mean score of 38.67 ± 8.16. Among the participants, 404 (35.7%) met the criteria for an anxious state (SAS score ≥ 40). The distribution of anxiety scores across demographic characteristics is presented in Table 1.
As shown in Table 1, gender, age, nursing experience, professional title, and hospital level were significantly associated with anxiety levels among nurses (all p < 0.05). Male nurses exhibited nearly 3 points higher anxiety scores than female nurses, with a 23-percentage-point greater prevalence of anxiety. Post-hoc pairwise comparisons detected a statistically significant difference only for nurses aged <22 years, who reported higher anxiety than all other age groups. No other inter-group differences were significant.
A similar pattern was observed for nursing experience: nurses with less than 3 years of experience reported significantly higher anxiety than their more experienced counterparts. In terms of professional title, nurses with intermediate titles showed the highest anxiety levels, significantly exceeding those with primary titles. Additionally, nurses in Grade 2 hospitals reported anxiety scores nearly 5 points higher than those in Grade 3 hospitals and approximately 3 points higher than those in other hospitals, such as community hospitals.
Although not statistically significant in this sample, descriptive trends suggested that married nurses without children had one of the highest mean anxiety scores, whereas those with only one child had the lowest. The overall difference across reproductive status groups approached but did not reach statistical significance (p = 0.063). Further investigation with larger samples is warranted to validate these preliminary observations.
Correlations between anxiety and social support among Chinese nurses
3.2
The relationship between social support and anxiety among Chinese nurses was examined using correlation analysis (Table 2). Social support and its three dimensions were significantly negatively correlated with anxiety scores, indicating that the more social support nurses receive, the lower their anxiety levels will be. These results support the hypothesis that social support serves as a protective factor against anxiety. Among the dimensions, support utilization showed the strongest negative correlation with anxiety, followed by objective support and subjective support (all p < 0.05). The three dimensions of social support were moderately and positively correlated with each other (0.307 ≤ r ≤ 0.526, all p < 0.05), reflecting their interrelatedness within a comprehensive social support system.
Furthermore, the total social support score was highly correlated with each dimension (r > 0.7), demonstrating good structural validity of the Social Support Rating Scale in this sample.
Correlations between anxiety and psychological resilience among Chinese nurses
3.3
Psychological resilience and its four dimensions—self-efficacy, hope, resiliency, and optimism—were all significantly negatively correlated with anxiety (all p < 0.001), supporting the hypothesis that resilience acts as a protective factor. Among the dimensions, resiliency showed the strongest correlation with anxiety (r = −0.285), followed by optimism (r = −0.239) and hope (r = −0.224), while self-efficacy had the weakest correlation (r = −0.186). Analysis of the scale’s internal structure revealed very high correlations among self-efficacy, hope, and optimism (0.933 ≤ r ≤ 0.955). In contrast, the resiliency dimension was only moderately correlated with the other three (0.278 ≤ r ≤ 0.302), suggesting it represents a distinct facet of psychological resilience in this sample.
The significant correlations demonstrated in Tables 2, 3 satisfy the preliminary conditions for testing a mediation effect, as both the independent variable (social support) and the mediator (psychological resilience) are significantly associated with the dependent variable (anxiety). We therefore proceeded to formally test the proposed mediation model.
Correlation analysis between social support and psychological resilience among Chinese nurses
3.4
Table 4 presents the correlation results. A significant positive correlation was found between the total scores of social support and psychological resilience (r = 0.361, p < 0.001). Specifically, the correlation of total social support with the individual resilience dimensions, ranked in descending order of strength, was optimism, hope, self-efficacy, and resiliency (all p < 0.001). Furthermore, among the social support dimensions, their correlations with total psychological resilience showed an ascending order of strength: support utilization, objective support, and subjective support (all p < 0.001).
Analysis of the mediating role of psychological resilience
3.5
As presented in Table 5, three regression models were constructed to examine the relationships among the variables. Model 1 showed that, after controlling for other covariates, social support remained a significant negative predictor of anxiety scores among nurses (β = −0.313, p < 0.01). In Model 2, social support was found to be independently and positively associated with psychological resilience (β = 1.295, p < 0.01). Model 3 further revealed that psychological resilience had a significant negative effect on anxiety (β = −0.051, p < 0.01), while the direct effect of social support on anxiety, though still significant, decreased in magnitude from–0.313 to–0.247. These results suggest that psychological resilience partially mediates the relationship between social support and anxiety. The increase in R^2^ from 0.124 to 0.150 indicates that the inclusion of psychological resilience improved the explanatory power of the model. All key pathways—social support to psychological resilience and psychological resilience to anxiety—were statistically significant (p < 0.001).
Path coefficients along with statistical inference results are summarized in Table 6. The total effect of social support on anxiety (without the mediator) yielded a 95% confidence interval (CI) of (−0.378, −0.248), which excludes zero. Similarly, the direct effect of social support on anxiety, after adjusting for psychological resilience, had a 95% CI of (−0.315, −0.179), also excluding zero. The indirect effect of social support on anxiety through psychological resilience was significant, with a 95% CI of (−0.080, −0.038) that does not include zero. These findings support a significant partial mediating role of psychological resilience in the relationship between social support and nurses’ anxiety. The mediation effect accounted for approximately 21.1% of the total effect (indirect effect/total effect = −0.066/–0.313 ≈ 21.1%).
The hypothesized mediation model was tested using structural equation modeling (SEM) with latent variables (Figure 1). To enable comparison across paths, standardized regression coefficients are presented. As all variables were modeled as latent factors, this approach accounts for measurement error. All path coefficients were significant (p < 0.05; Supplementary Table S1). The results indicate that, in addition to a direct negative effect on anxiety, social support had a significant positive effect on psychological resilience. Its effect on anxiety was also transmitted indirectly via this enhanced resilience. This latent-variable analysis confirms the findings from the observed-variable model, demonstrating result robustness.
Path diagram of the relationships among social support, psychological resilience, and nurses’ anxiety.
To delineate the specific roles of each dimension, we decomposed the effects of the three social support facets within the mediation model (Figure 2; all paths significant per Supplementary Table S2). Analysis of the standardized path coefficients revealed a divergence: support utilization and objective support had relatively larger direct effects on anxiety, while the direct effect of subjective support was minimal. Notably, the pattern of indirect effects told a different story. The pathway mediated by psychological resilience was strongest for subjective support, with an indirect effect constituting 41% of its total impact.
Psychological resilience mediates the relationship between three dimensions of social support and anxiety. (A) Schematic diagram of psychological resilience mediating the relationship between objective support and anxiety. (B) Schematic diagram of psychological resilience mediating the relationship between subjective support and anxiety. (C) Schematic diagram of psychological resilience mediating the relationship between utilization of support and anxiety.
Discussion
4
Grounded in a public health perspective, this study examines the interaction between social-environmental factors and individual characteristics in relation to nurses’ occupational mental health. Based on a cross-sectional survey in Chengdu, China, the findings support the hypothesized mediation model, wherein psychological resilience mediates the effect of social support on anxiety. This reveals a salient psychological mechanism among nursing staff: the pathway from the acquisition of external resources to the building of internal capacity, ultimately shaping emotional outcomes.
The primary finding confirms that psychological resilience mediates the effect of social support on anxiety. Conceptually, social support—an external resource encompassing connections with leaders, colleagues, family, and friends (35)—serves a dual function: it directly reduces anxiety, and it is also converted into psychological resilience. This internal resource, characterized by self-efficacy, hope, resiliency, and optimism (36), enhances nurses’ ability to deploy cognitive and emotional strategies under stress, thereby buffering against anxiety. This mechanism is not unique to our sample; it has been replicated in diverse populations. For example, Eliza et al. reported a significant mediation effect of psychological resilience (explaining up to 30.9% of the total effect) between social support and anxiety among nurses, foreign domestic helpers, and residents in Hong Kong (37). Consistent evidence from varied contexts supports this mechanism from nurses. First, in a study of people living with HIV/AIDS, psychological resilience fully mediated the social support-anxiety link, accounting for 68.42% of the effect (38). Second, research among postpartum women found that resilience partially mediated the relationship between increased support and reduced anxiety (39). Third, the COVID-19 pandemic underscored this pathway under crisis conditions; multiple studies confirmed that resilience mediated the effects of specific stressors—such as perceived pandemic stress, job stress, occupational exposure, and fear of infection—on the anxiety, depression, and distress of healthcare workers (40–43). Thus, psychological resilience emerges as a key mediator, defining a resource-transformation pathway: external support builds internal resilience, which ultimately safeguards emotional well-being. This pathway aligns with and elaborates upon two key theories. It concretely illustrates the COR Theory’s principle of resource investment and gain (44), showing how social support, as an external resource, translates into psychological resilience to prevent mental health depletion. It also provides a specific cognitive-personal mechanism for the Stress-Buffering Model (14), demonstrating that support alleviates anxiety by building resilience, thereby enacting the stress-buffering process.
Building on the confirmed partial mediation model, this study provides a nuanced understanding of how different dimensions of social support relate to anxiety. The pathways diverged markedly: while “support utilization” and “objective support” had stronger direct links to anxiety, “subjective support” exerted its influence predominantly indirectly through psychological resilience, with its mediated effect being nearly double. This underscores that the protective mechanism is not uniform; the subjective perception of available support is uniquely channeled through the development of internal resilience. This pattern diverges from findings in other contexts, such as among lung cancer patients, where resilience mediated the link for subjective support and support utilization but not for objective support (45), suggesting important population or context-specific moderators. Furthermore, a study of older adults in China demonstrated a gender difference: the association between subjective support and cognitive function was fully mediated by psychological resilience in men, whereas it was only partially mediated in women (46). Therefore, interventions should be population-specific. For the nursing population, our study yields two practical recommendations. First, reinforce the provision and accessible use of objective, material support. This involves securing necessary resources and training to utilize them effectively. Simultaneously, fostering a supportive climate that enhances nurses’ subjective perception and experience of support is critical, as this directly cultivates psychological resilience. Building this internal resource is key to safeguarding mental health and alleviating anxiety.
Our analysis revealed differential correlations between the constituent dimensions of psychological resilience—self-efficacy, hope, resiliency, and optimism (36)—and anxiety. Notably, resiliency (defined as focused persistence in adversity) (47) showed the strongest inverse association, highlighting the paramount importance of stable adaptability under stress for anxiety reduction. Similarly, optimism (48) and hope (49) were significantly negatively correlated with anxiety. Optimism fosters adaptive stress appraisal (50), whereas hope underpins the pursuit of viable pathways despite obstacles (49, 51), both mitigating anxiety. Of the four dimensions, self-efficacy exhibited the weakest, albeit significant, negative correlation. This likely reflects that while professional confidence facilitates proactive stress coping, its direct protective effect against anxiety may be less pronounced than that of other resilience facets.
It is also noteworthy that the anxiety levels observed among nurses in Chengdu, China, were relatively high, nearing the upper bound of prevalence estimates for Chinese nurses in a global synthesis (52). This elevated prevalence points to acute mental health strains within the current healthcare environment. The immediate context includes the legacy of the pandemic, specifically 3 years of lockdown measures in China. These pressures are compounded by longer-term structural factors, such as the ongoing economic slowdown and stricter healthcare payment reforms, which may adversely affect nurses’ socioeconomic stability and mental health (53). The high anxiety levels likely result from a confluence of acute, sub-acute, and chronic stressors. First, anxiety may be a lingering psychological sequel of the extreme stress nurses faced during the pandemic. Second, this is compounded by sustained post-pandemic pressures, as healthcare systems address care backlogs, potentially maintaining high workloads (54). Finally, these are exacerbated by the profession’s inherent, chronic stressors—including extended hours, high-intensity tasks, and shift-work disruption—which continuously elevate burnout risk and undermine mental health (55).
Policy and practice should focus on evidence-based interventions targeting psychological resilience—the critical mediator identified. For instance, individual-focused approaches like resilience training, mindfulness, and cognitive-behavioral therapy have proven effective (56). Simultaneously, healthcare institutions must implement system-level strategies, including mental health education, competency training, and confidential counseling. Implementing structured peer-support networks within clinical teams is also essential, as they facilitate mutual assistance and open communication, fostering team cohesion and sustained well-being (57, 58). This multi-pronged approach builds the core facets of resilience (self-efficacy, hope, resiliency, optimism), leading to significant anxiety reduction.
Limitations of the study
5
This study has several limitations. First, the cross-sectional design precludes causal inference regarding the relationships among social support, psychological resilience, and anxiety, so there may be confounding bias related to time. Second, as the sample was drawn exclusively from Sichuan Province, China, the generalizability of the findings to other regions or cultural contexts may be limited, there may be selection bias. Future research should adopt longitudinal or experimental designs to examine the long-term and causal effects of social support and resilience on anxiety. It would also be valuable to validate the current model in diverse healthcare systems and cultural settings. Furthermore, future studies should design, implement, and evaluate multi-level interventions based on the present findings, and conduct cost-effectiveness evaluations to inform public health resource allocation. Nurse characteristics were accounted for as confounders in this study and thus were not analyzed in detail. A fruitful direction for future research would be to conduct stratified analyses based on these or other clinically meaningful variables to uncover potential subgroup differences and elucidate nuanced intervention targets.
Conclusion
6
This empirical survey study, conducted among nurses in Chengdu, Sichuan Province, China, in the post-pandemic era, reveals two key findings. First, anxiety levels within the nursing cohort remain notably elevated. Second, psychological resilience plays a partial mediating role in the relationship between social support and anxiety. Notably, the strongest mediating effect of psychological resilience is observed on the pathway linking subjective support to anxiety. This suggests that the anxiety-alleviating function of social support may operate through the internalization of psychological resilience. Moreover, the interaction between perceived support from the social environment and individual nurse characteristics—such as psychological resilience—appears to be a critical factor in emotional regulation. The findings further indicate that, to advance public-health policy implementation through nurses’ occupational well-being, it is essential not only to foster a supportive environment but also to adopt systematic strategies that enhance nurses’ subjective perception of support, thereby cultivating their psychological resilience to mitigate anxiety.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Søvold LE Naslund JA Kousoulis AA Saxena S Qoronfleh MW Grobler C . Prioritizing the mental health and well-being of healthcare workers: an urgent global public health priority. Front Public Health. (2021) 9:679397. doi: 10.3389/fpubh.2021.679397, 34026720 PMC 8137852 · doi ↗ · pubmed ↗
- 2Li LZ Yang P Singer SJ Pfeffer J Mathur MB Shanafelt T. Nurse burnout and patient safety, satisfaction, and quality of care: a systematic review and meta-analysis. JAMA Netw Open. (2024) 7:e 2443059. doi: 10.1001/jamanetworkopen.2024.43059, 39499515 PMC 11539016 · doi ↗ · pubmed ↗
- 3Asefzadeh S Kalhor R Tir M. Patient safety culture and job stress among nurses in Mazandaran, Iran. Electron Physician. (2017) 9:6010. doi: 10.19082/6010, 29560154 PMC 5843428 · doi ↗ · pubmed ↗
- 4Bautista JR Lauria PAS Contreras MCS Maranion MMG Abeleda RD. Specific stressors relate to nurses’ job satisfaction, perceived quality of care, and turnover intention. Int J Nurs Pract. (2020) 26:e 12774. doi: 10.1111/ijn.12774, 31423700 · doi ↗ · pubmed ↗
- 5Starc J. Stress factors among nurses at the primary and secondary level of public sector health care: the case of Slovenia. Open Access Maced J Med Sci. (2018) 6:416–22. doi: 10.3889/oamjms.2018.100, 29531616 PMC 5839460 · doi ↗ · pubmed ↗
- 6Lu G Xiao S He J Xie W Ge W Meng F . Prevalence of depression and its correlation with anxiety, headache and sleep disorders among medical staff in the Hainan Province of China. Front Public Health. (2023) 11:1122626. doi: 10.3389/fpubh.2023.1122626, 37441641 PMC 10333496 · doi ↗ · pubmed ↗
- 7Pang Y Dan H Jung H Bae N Kim O. Depressive symptoms, professional quality of life and turnover intention in Korean nurses. Int Nurs Rev. (2020) 67:387–94. doi: 10.1111/inr.1260032633425 · doi ↗ · pubmed ↗
- 8Chen J Liu X Wang D Jin Y He M Ma Y . Risk factors for depression and anxiety in healthcare workers deployed during the COVID-19 outbreak in China. Soc Psychiatry Psychiatr Epidemiol. (2021) 56:47–55. doi: 10.1007/s 00127-020-01954-1, 32914298 PMC 7483060 · doi ↗ · pubmed ↗