Computed Tomography Yield and Predictors of Pulmonary Embolism in Mechanically Ventilated Patients—A Retrospective Study
Erik Bruno, Matilda Kewenter, Angeliki Dimopoulou Creusen, Freyr Einarsson, Gaetano Perchiazzi, Kristina Svennerholm, Christian Rylander

TL;DR
This study finds that about 21% of CT scans for suspected blood clots in ventilated ICU patients show actual clots, with high D-dimer levels and strong clinical suspicion being key indicators.
Contribution
The study identifies specific clinical indicators for pulmonary embolism in ventilated ICU patients using real-world data and free-text analysis.
Findings
21% of CTPA exams in ventilated ICU patients confirmed pulmonary embolism.
Elevated D-dimer and undefined clinical suspicion were linked to positive results.
No patient variables were significantly associated with PE findings.
Abstract
The reported prevalence of pulmonary embolism (PE) detected during intensive care varies substantially. Computed tomography pulmonary angiography (CTPA) is the diagnostic reference method, but assessing pre‐test probability and finding distinct indications for CTPA from clinical observations is difficult in mechanically ventilated critically ill patients. To describe the rate of positive diagnostic outcome (yield) from CTPA exams performed on PE suspicion and to identify predictors in the free text motivational reasons from the referring clinician and among selected patient variables during intensive care for other conditions. CTPA exams and reports in adult, mechanically ventilated patients referred from two intensive care units during a 5‐year period were compared to the radiology order content and to data collected from medical records. The association between a positive exam and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
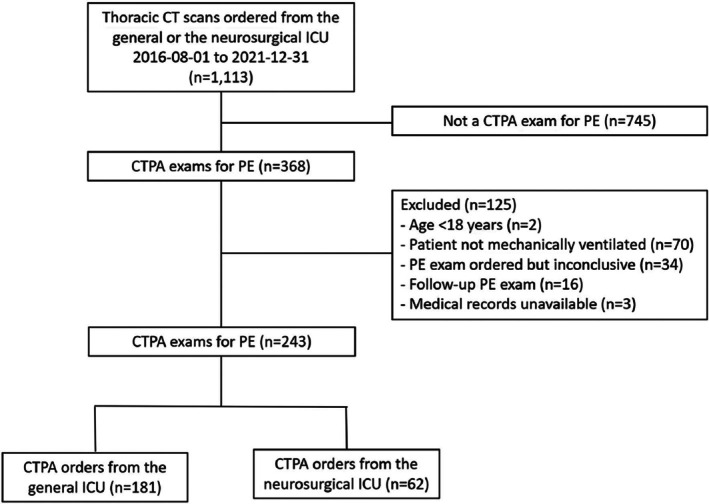 FIGURE 1
FIGURE 1| Variable |
| CTPA positive |
| CTPA negative |
|
|---|---|---|---|---|---|
| Demographics | |||||
| Age (years) |
| 60 (46:68) |
| 66 (54:73) | < 0.01 |
| Female |
| 9 (17) |
| 54 (28) | 0.15 |
| Weight (kg) |
| 88 (77:106) |
| 87 (74:104) | 0.39 |
| BMI (kg/m2) |
| 29 (25:33) |
| 29 (25:34) | 0.5 |
| Co‐morbidities | |||||
| Hypertension |
| 27 (52) |
| 94 (49) | 0.76 |
| Heart failure |
| 1 (1.9) |
| 22 (12) | 0.03 |
| Cardiac arrhythmia |
| 6 (12) |
| 28 (15) | 0.66 |
| Ischemic heart disease |
| 3 (5.8) |
| 22 (12) | 0.31 |
| COPD |
| 0 |
| 13 (6.8) | 0.08 |
| Asthma |
| 1 (1.9) |
| 30 (16) | < 0.05 |
| Restrictive lung disease |
| 0 |
| 0 | — |
| Diabetes Type 1 |
| 0 |
| 2 (1.0) | 1.00 |
| Diabetes Type 2 |
| 14 (27) |
| 35 (18) | 0.18 |
| Chronic renal failure |
| 0 |
| 11 (5.8) | 0.13 |
| Acute on chronic renal failure |
| 0 |
| 4 (2.1) | 0.58 |
| Acute kidney injury |
| 3 (5.8) |
| 15 (7.9) | 0.77 |
| Coagulation disorder |
| 1 (1.9) |
| 2 (1.0) | 0.52 |
| Previous DVT |
| 0 |
| 6 (3.1) | 0.35 |
| Previous PE |
| 1 (1.9) |
| 5 (2.6) | 1.00 |
| Malignancy |
| 6 (12) |
| 37 (19) | 0.22 |
| Diagnosis at risk for VTE | |||||
| Sepsis |
| 5 (9.6) |
| 29 (15) | 0.37 |
| Polytrauma |
| 3 (5.8) |
| 8 (4.2) | 0.71 |
| Isolated TBI |
| 6 (12) |
| 16 (8.4) | 0.58 |
| COVID‐19 |
| 21 (40) |
| 74 (39) | 0.87 |
| Surgery within 30 days |
| 17 (33) |
| 43 (23) | 0.15 |
| Thromboprophylaxis | |||||
| Low molec. weight heparin |
| 36 (69) |
| 128 (67) | 0.84 |
| ICU stay | |||||
| Days in ICU in total |
| 14 (9:22) |
| 11 (5:21) | 0.06 |
| Days in ICU before CT |
| 3 (1:10) |
| 3 (1:8) | 0.19 |
| Survival | |||||
| Alive at ICU discharge |
| 44 (85) |
| 155 (81) | 0.68 |
| Alive 30 days after CTPA |
| 42 (81) |
| 136 (71) | 0.15 |
| Parameter |
| CTPA positive |
| CTPA negative |
|
|---|---|---|---|---|---|
| pH |
| 7.41 (7.37:7.45) |
| 7.40 (7.34:7.45) | 0.55 |
| PaCO2 (kPa) |
| 5.60 (5.10:6.50) |
| 5.60 (5.15:6.40) | 0.84 |
| PaO2 (kPa) |
| 10.6 (9.80:12.80) |
| 10.80 (9.35:12.65) | 0.62 |
| Base excess (mmol/L) |
| 2.8 (−0.1:4.1) |
| 2.1 (−0.9:4.9) | 0.80 |
| Bicarbonate (mmol/L) |
| 27 (24:28) |
| 26 (23:29) | 0.75 |
| Lactate (mmol/L) |
| 1.2 (0.9:1.7) |
| 1.3 (0.9:1.7) | 0.27 |
| Sodium (mmol/L) |
| 141 (137:144) |
| 140 (137:143) | 0.17 |
| Potassium (mmol/L) |
| 4.2 (3.9:4.5) |
| 4.0 (3.8:4.3) | 0.02 |
| Glucose (mmol/L) |
| 8.3 (7.4:9.7) |
| 8.8 (7.3:10.1) | 0.49 |
| CRP (mg/L) |
| 126 (51:196) | 2 | 123 (48:206) | 0.67 |
| Leukocytes (109/L) |
| 12.5 (10.1:14.5) |
| 12.0 (8.3:16.0) | 0.58 |
| Platelets (109/L) |
| 279 (190:382) |
| 234 (169:358) | 0.21 |
| PT (INR) |
| 1.1 (1.0:1.2) |
| 1.1 (1.0:1.2) | 0.12 |
| APTT (sec) |
| 40 (34:101) |
| 46 (38:101) | 0.04 |
| Fibrinogen |
| 6.25 (4.38:6.98) |
| 5.70 (4.25:7.12) | 0.12 |
| D‐dimer (mg/L) |
| 11 (5.8:17) |
| 3.6 (1.9:9.1) | 0.10 |
| Troponin T (ng/L) |
| 17 (8.2:77) |
| 38 (26:99) | 0.76 |
| Troponin I (ng/L) |
| 18 (4.5: 53) |
| 34 (9.1;119) | 0.13 |
| Creatinine (μmol/L) before CTPA |
| 84 (62:120) |
| 79 (61:121) | 0.58 |
| Creatinine (μmol/L) the day after CTPA |
| 82 (64:145) |
| 83 (61:124) | 0.91 |
| Creatinine (μmol/L) at ICU discharge |
| 68 (53:101) |
| 71 (52:108) | 0.45 |
| Variable |
| CTPA positive |
| CTPA negative |
|
|---|---|---|---|---|---|
| Body temperature (°C) |
| 37.6 (37.1:38.2) |
| 37.4 (36.6:38.1) | 0.05 |
| SaO2 (%) |
| 97 (95:98) |
| 97 (95:99) | 0.95 |
| FiO2 |
| 0.55 (0.40:0.65) |
| 0.55 (0.40:0.65) | 0.74 |
| PaO2/FiO2 (kPa) |
| 21.0 (15.8:26.7) |
| 20.2 (15.0:29.5) | 0.51 |
| Heart rate (BPM) |
| 78 (68:88) |
| 80 (68:95) | 0.49 |
| Systolic BP (mmHg) |
| 123 (110:148) |
| 123 (108:142) | 0.45 |
| Diastolic BP (mmHg) |
| 62 (56:66) | 2 | 60 (53:68) | 0.51 |
| RV/LV ratio |
| 0.89 (0.84:0.97) |
| 0.86 (0.81:0.97) | 0.22 |
| RV/LV ratio > 0.9 |
| 10 (19) |
| 68 (36) | 0.39 |
| Reason | CTPA positive | CTPA negative |
|
|---|---|---|---|
| Hypoxemia | 27 (52) | 106 (55) | 0.75 |
| Hypercapnia | 0 | 4 (2.1) | 0.58 |
| Unstable circulation | 5 (9.6) | 38 (20) | 0.10 |
| Elevated D‐Dimer | 21 (40) | 32 (17) | < 0.05 |
| Undefined clinical suspicion | 9 (17) | 17 (8.9) | 0.12 |
| Reason | OR | 95% CI |
|
|---|---|---|---|
| Hypoxemia | 1.28 | 0.62–2.7 | 0.51 |
| Hypercapnia | 0.80 | 0.01–8.4 | 0.88 |
| Unstable circulation | 0.88 | 0.29–2.3 | 0.81 |
| Elevated D‐Dimer | 4.03 | 1.9–8.8 | < 0.01 |
| Undefined clinical suspicion | 3.73 | 1.3–11 | 0.02 |
| Variable | OR | 95% CI |
|
|---|---|---|---|
| Biometrics | |||
| Male | 2.06 | 0.96–4.8 | 0.08 |
| Co‐morbidities | |||
| Diabetes Type 2 | 1.87 | 0.88–3.9 | 0.09 |
| ICU diagnosis at risk for VTE | |||
| Surgery within 30 days | 1.88 | 0.93–3.7 | 0.07 |
- —Uppsala Universitet10.13039/501100007051
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVenous Thromboembolism Diagnosis and Management · Ultrasound in Clinical Applications · Central Venous Catheters and Hemodialysis
Introduction
1
Venous thromboembolism (VTE), including deep venous thrombosis (DVT) and pulmonary embolism (PE), is a well‐known complication in patients admitted to the intensive care unit (ICU) for other conditions [1]. During intensive care, risk from specific circumstances such as immobilization, sedation, mechanical ventilation, and pro‐thrombotic states is added to general risk factors for VTE [2]. The reported incidence of VTE varies substantially depending on the diagnostic method and population of critically ill patients studied [1]. The reference diagnostic test for PE is computed tomography pulmonary angiography (CTPA) using intravenous iodine contrast [3]. However, the exam may be withheld due to a perceived risk of contrast‐associated acute kidney injury and hazards associated with transporting critically ill patients to the radiology department [4, 5]. Furthermore, PE occurring in the ICU is often silent, with typical respiratory and circulatory failure ascribed to alternative diagnoses [6]. Clinical instruments developed for assessing pre‐test probability of acute PE are less useful in mechanically ventilated, critically ill patients [7]. This makes it uncertain on what grounds a CTPA exam for PE is ordered by intensive care clinicians. It is also sparsely described in the literature to which extent clinical variables are associated with PE during intensive care [8].
The aim of this retrospective study was to describe the diagnostic outcome and to identify predictors in the free‐text motivation from the referring clinician and among selected patient variables in mechanically ventilated patients referred to CTPA on clinical suspicion of PE during intensive care for other conditions.
Methods
2
This single‐center cohort study was approved by the Swedish Ethical Review Authority (DNr 2022‐03568‐01). Patient consent was waived due to the nature of the retrospective analysis of pseudonymized data. The study is reported according to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement [9].
Patients and Settings
2.1
The study was conducted in the Uppsala University Hospital, an 800‐bed tertiary center for mid‐northern Sweden, serving a population of ~2 million. The study period lasted from August 1, 2016, to December 31, 2021. All adult (> 18 years), mechanically ventilated patients in the 8‐bed general ICU and the 8‐bed neurosurgical ICU who underwent a CTPA exam for clinically suspected PE were eligible. Patients with an inconclusive CTPA exam for any reason were excluded.
Data
2.2
The patients were identified through procedure codes in the local radiological archive from which CTPA exams, the radiology reports and text details of the orders were extracted. The presence of PE was established from the radiology reports, for which the standard operating procedure stated that findings must be assessed by two radiologists, of whom at least one is a consultant in radiology. The right‐to‐left ventricular transverse diameter (RV/LV) ratio was measured for the purpose of the study in axial sections on the CTPA images by one of the authors (MK) after saturated training by a consultant in radiology. Demography, medical history including past and present relevant ICD‐10 diagnosis, surgery, clinical, and laboratory parameters, and any dose of pharmacological thrombosis prophylaxis were collected from digital patient record systems. The physiological and laboratory parameters were taken from the last entry available before the CTPA exam except for creatinine which was sampled from three occasions: The last value before CTPA, the first value after CTPA, and the last value before discharge from the ICU. We recorded established risk factors for PE including a main ICU diagnosis of sepsis, polytrauma, isolated traumatic brain injury (TBI), surgery within 30 days, and COVID‐19 [10, 11, 12]. Admission to the neurosurgical ICU, a history of malignancy and the presence of thromboprophylaxis were also added to the analysis [13].
From the free text in the radiology orders, we identified thematic motivational reasons, used by the referring clinicians for motivation of PE suspicion, and arbitrarily grouped them into five categories: “Hypoxemia,” “Hypercapnia,” “Unstable circulation,” “Elevated D‐dimer,” and “Undefined clinical suspicion.” We did not use predefined operational definitions or threshold values but assessed the qualitative content as reflecting the clinical decisions to perform the exam. One CTPA order could contain more than one reason. Text referrals without motivation were not categorized.
Outcomes
2.3
Outcomes were defined as the crude proportion of positive CTPA exams (yield) and their association with five arbitrarily defined reasons for ordering the exam. Additionally, we examined the association between selected patient variables and a positive exam.
Statistical Analysis
2.4
For group statistics, continuous variables are presented as mean (SD) or median (first and third quartile; Q1:Q3) according to distribution and dichotomous variables are presented as numbers (%). Wilson exact score confidence intervals (CI) are given for the main outcome proportions. The Mann–Whitney U‐test or Fisher's exact test was used for respective comparisons between the groups. The association between the reasons given in the CTPA orders and a positive CTPA exam, expressed as the event odds ratio (OR) with corresponding 95% CI, was assessed using multivariable penalized logistic regression with Firth's correction, entering all categorized reasons into the model. To assess the association between selected patient variables and a positive CTPA exam, we applied first univariable, then multivariable logistic regression. Variables showing an OR above 1 and a p ≤ 0.20 in the univariable analysis and with less than 5% missing values were included in the multivariable model. Statistical analysis was performed using R version 4.5.2 (The R Foundation for Statistical Computing, Vienna, Austria), with penalized logistic regression implemented using the logistf package.
Results
3
During the 5‐year study period, there were 7498 patient admissions and 1113 computed tomography exams of the chest registered for the two ICUs. After exclusions, 243 adult patients with a mean (SD) age of 60 (15) years met criteria for a unique CTPA exam on PE suspicion (Figure 1). PE was found in 43/180 (24% [95% CI: 18–31]) men and in 9/63 (14% [95% CI: 7.7–25]) women, totaling 52/243 (21% [95% CI: 17–26]) patients. The emboli were located in the pulmonary artery bifurcation in 2 (3.8%), the central/lobar arteries in 17 (33%), the segmental arteries in 21 (40%), and the subsegmental arteries in 14 (27%) cases.
Flow chart.
Patients with a positive finding on CTPA were younger and had a lower prevalence of heart failure and asthma. Thromboprophylaxis using low molecular weight heparin was administered to 36 (69%) of the patients with and to 128 (67%) of the patients without a positive exam for PE (Table 1). There was no non‐pharmacological thromboprophylaxis used alone. There was no difference between the groups as to creatinine levels before and after CTPA exams (Table 2), vital signs, or RV/LV ratio (Table 3).
The reason for ordering a CTPA was not specified for 2 (3.8%) of the patients with and 32 (17%) of the patients without a positive exam. “Elevated D‐dimer” was the only reason being more prevalent among patients with a positive CTPA exam (Table 4). “Elevated D‐dimer” and “Undefined clinical suspicion” were significantly associated with a positive exam in the multivariable logistic regression (Table 5).
The selection of patient variables associated with a positive CTPA exam in the univariable logistic regression (Table S1) included male sex, diabetes Type 2, and surgery within 30 days, but none of these was significantly associated with a CTPA finding of PE in the multivariable analysis (Table 6).
Discussion
4
In this study, we found a diagnostic yield of 21% [95% CI: 17–26] from 243 CTPA exams, performed due to suspicion of PE in mechanically ventilated, critically ill patients. In a recent report, including 2713 patients having undergone CTPA to rule out PE in a tertiary center, 54/352 (15%) patients referred from the ICU had a positive exam, but there was no information about the degree of PE suspicion or the content of the radiology orders [14]. Very few studies of PE in intensive care patients report the rate of positive CTPA exams according to pre‐test clinical suspicion, but we found one comparable study from a single ICU where all patients, requiring mechanical ventilation and a thoracic contrast‐enhanced CT for any reason, were subjected to radiographic analysis of PE signs. PE was diagnosed in 33 of 176 (19%) patients, of whom 20 were “silent” (not suspected) [15]. A key issue when interpreting the yield of a diagnostic test is whether it was applied to patients with specific indications, or whether all patients were screened regardless of symptoms and signs. In the referenced study with an overall CT positivity of 19%, the yield was 16% (20/127) among 127 referred without PE suspicion and 26% (13/49) among patients where PE was suspected [15]. Several other studies report a low CTPA diagnostic yield (2%–8%), having divided detected PE cases by the number of total ICU admissions [6, 13, 16, 17, 18], but these likely underestimate the yield among suspected cases. The true prevalence of PE occurring in patients during intensive care remains largely unknown, especially considering the high number of missed PE found in autopsy studies [19]. Studies of CTPA yield are more common in patients referred from emergency departments (EDs) or hospital wards on PE suspicion with results varying from small fractions to almost 35% depending on pretest probability requirements for ordering the exam [20, 21, 22, 23]. For the ED setting, the UK Royal College of Radiologists advises an acceptable level of positive CTPA yield to be between 15% and 37% [24]. Similar recommendations for patients referred from the ICU are lacking but the result of our study falls within that span.
We also found that, among the five categories of motivational reasons motivating the clinical PE suspicion in the CTPA orders, “Elevated D‐dimer” and “Undefined clinical suspicion” were predictors of a PE finding. These two reasons constituted 30% of all reasons identified, which may be interpreted as clinicians being less precise in predicting a positive PE exam from the patient characteristics they observed. To our knowledge, this question has not previously been investigated in the ICU setting. However, one study investigating the content of radiology orders from an ED also found that a high D‐dimer value, as a reason for ordering CTPA in suspicion of PE, was among the strongest predictors of a positive finding [22]. Although an increased D‐dimer level has a low specificity for PE in critically ill patients in general [25], it may strengthen the clinical picture when other potential signs of PE are present. However, although male sex, diabetes mellitus Type 2, and surgery within 30 days seemed important in the first univariable analysis, we did not find any of the selected patient variables significantly associated with a positive CTPA exam. This contrasts with a number of studies that have established similar patient properties and contextual factors purporting risk for developing VTE in the ICU [8, 26]. Contrarily to what may have been expected, a COVID‐19 diagnosis did not turn out to be a significant PE predictor in spite of the well described high incidence of VTE in these critically ill patients during the pandemic [27, 28]. This discrepancy from the literature was also observed for ICU diagnoses of trauma and TBI, which did not significantly predict a positive finding on CTPA [11, 29]. The lack of significant association between specific patient predictors and positive CTPA findings in our study may be explained by the limited number of patients in each diagnostic category.
The proportion of patients on pharmacological thromboprophylaxis did not differ between patients with and without a positive PE exam. The fact that more than 30% did not receive this treatment despite recommendations is of concern, albeit not uncommon in the literature [30]. Lastly, we found no difference between renal function before and after the CTPA exam. This agrees with a recent study of intensive care patients submitted to radiographical exams that included intravenous contrast media and the recently reported general low risk of contrast‐associated acute kidney injury [31, 32].
Limitations
4.1
This study has several limitations. We focused on sedated, mechanically ventilated patients to study a population where symptoms are concealed and physiological signs of PE are difficult to distinguish but that reduced the number of clinical patient variables available for analysis. The CTPA outcome should be regarded as robust, but the categorization of the reasons given in the CTPA orders was based on qualitative interpretation of free‐text in the referral orders which introduced observer bias and precluded imputation for missing information. The absence of standardized referral criteria and the frequent lack of physiologically defined indications in referral texts limit the precision and reproducibility of this categorization method. The retrospective design resulted in a number of missing values for variables such as coagulation lab tests, and we did not have access to possible dead‐space ventilation which may be important for suspecting undetected PE. The penalized logistic regression approach in the analysis of the order reasons was chosen due to sparse data and the absence of events for some of the reasons, which would have resulted in non‐estimable coefficients under standard logistic regression. However, we did not perform any imputation due to the skewed nature of the data. We did not have data to classify the PE risk according to the guidelines issued by the European Society of Cardiology, but the low RV/LV ratios indicated PE of less severe character, which limits the generalizability of the findings to unstable patients. Yet, our results support the well‐known need for better tools for structured assessment of the clinical risk of PE among patients in the ICU.
Conclusion
5
The diagnostic yield of clinical CTPA exams for suspected PE in mechanically ventilated patients fell within a range commonly cited for suspected acute PE in emergency department populations, but its association with clinical signs described in the CTPA order and with selected patient variables was low.
Author Contributions
Erik Bruno: Acquired data, analyzed data and drafted the first version of the manuscript. Matilda Kewenter: Acquired and analyzed data. Angeliki Dimopoulou Creusen: Designed the work and assisted in the acquisition of data. Freyr Einarsson: Substantially revised the manuscript. Gaetano Perchiazzi: Substantially revised the manuscript. Kristina Svennerholm: Substantially revised the manuscript. Christian Rylander: Conceptualized the study and designed the work, interpreted the data and substantially revised the manuscript. All authors read and approved the final manuscript.
Funding
This study was supported by departmental funding from the Uppsala University Hospital and the Uppsala University. Gaetano Perchiazzi and Christian Rylander are holders of the Alvar Gullstrand research grant (Gaetano Perchiazzi ALF‐938050; Christian Rylander ALF‐978293) but did not receive any specific grant from funding agencies in the public, commercial, or non‐profit sectors.
Ethics Statement
The study was approved by the Swedish Ethical Review Authority (DNr 2022‐03568‐01). Patient consent was waived due to the retrospective nature of the analysis.
Consent
The authors have nothing to report.
Conflicts of Interest
Freyr Einarsson and Kristina Svennerholm declare having received lecture fees from Leo Pharma. All other authors declare no conflicts of interest.
Supporting information
Data S1: aas70216‐sup‐0001‐Supinfo.docx.
Table S1: Association between single patient variables and a positive CTPA exam.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1X. Gao , L. Zeng , H. Wang , et al., “Prevalence of Venous Thromboembolism in Intensive Care Units: A Meta‐Analysis,” Journal of Clinical Medicine 11, no. 22 (2022): 6691.36431168 10.3390/jcm 11226691 PMC 9698016 · doi ↗ · pubmed ↗
- 2C. Minet , L. Potton , A. Bonadona , et al., “Venous Thromboembolism in the ICU: Main Characteristics, Diagnosis and Thromboprophylaxis,” Critical Care 19, no. 1 (2015): 287.26283414 10.1186/s 13054-015-1003-9PMC 4539929 · doi ↗ · pubmed ↗
- 3M. Remy‐Jardin , M. Pistolesi , L. R. Goodman , et al., “Management of Suspected Acute Pulmonary Embolism in the Era of CT Angiography: A Statement From the Fleischner Society,” Radiology 245, no. 2 (2007): 315–329.17848685 10.1148/radiol.2452070397 · doi ↗ · pubmed ↗
- 4L. M. Bergman , M. E. Pettersson , W. P. Chaboyer , E. D. Carlström , and M. L. Ringdal , “Safety Hazards During Intrahospital Transport: A Prospective Observational Study,” Critical Care Medicine 45, no. 10 (2017): e 1043–e 1049.28787292 10.1097/CCM.0000000000002653 · doi ↗ · pubmed ↗
- 5J. H. Rundback , D. Nahl , and V. Yoo , “Contrast‐Induced Nephropathy,” Journal of Vascular Surgery 54, no. 2 (2011): 575–579.21741789 10.1016/j.jvs.2011.04.047 · doi ↗ · pubmed ↗
- 6D. Schramm , A. G. Bach , H. J. Meyer , and A. Surov , “Thrombotic Events as Incidental Finding on Computed Tomography in Intensive Care Unit Patients,” Thrombosis Research 141 (2016): 171–174.27058274 10.1016/j.thromres.2016.03.030 · doi ↗ · pubmed ↗
- 7C. Katsios , M. Donadini , M. Meade , et al., “Prediction Scores Do Not Correlate With Clinically Adjudicated Categories of Pulmonary Embolism in Critically Ill Patients,” Canadian Respiratory Journal 21, no. 1 (2014): 36–42.24083302 10.1155/2014/296161 PMC 3938238 · doi ↗ · pubmed ↗
- 8C. S. Vrettou , E. Dima , and I. Sigala , “Pulmonary Embolism in Critically Ill Patients‐Prevention, Diagnosis, and Management,” Diagnostics (Basel) 14, no. 19 (2024): 2208.39410612 10.3390/diagnostics 14192208 PMC 11475110 · doi ↗ · pubmed ↗