Apalutamide‐Induced Hypothyroidism Associated With Increased Thyroid Hormone Clearance in Metastatic Prostate Cancer Patient: A Case Report
Jun Furumido, Akihiro Yamashita, Ryo Kato, Kanta Hori

TL;DR
A prostate cancer patient with a history of thyroidectomy experienced severe hypothyroidism after starting apalutamide treatment, highlighting the need for close thyroid monitoring.
Contribution
This case report highlights apalutamide's rare but significant effect of increasing thyroid hormone clearance in patients with prior thyroidectomy.
Findings
The patient's TSH levels rose despite increased levothyroxine dosage after apalutamide initiation.
TSH improved rapidly after apalutamide withdrawal, suggesting a direct drug effect.
The case underscores the need for close endocrine monitoring during apalutamide treatment in thyroid-compromised patients.
Abstract
Apalutamide (APA) is an androgen receptor signaling inhibitor widely used for metastatic hormone‐sensitive prostate cancer (mHSPC), though it can induce hypothyroidism. We report a severe case of APA‐induced hypothyroidism in a patient with a history of total thyroidectomy. A 65‐year‐old man receiving levothyroxine (175 μg/day) after thyroidectomy was diagnosed with mHSPC (Gleason score 4 + 4; PSA 13 904 ng/mL) with findings suggestive of cancer‐associated disseminated intravascular coagulation. Following APA initiation (240 mg/day), PSA decreased rapidly to 0.01 ng/mL. However, TSH levels rose progressively despite increasing levothyroxine to 275 μg/day. After a 4‐month follow‐up interruption, TSH reached 187.9 mIU/L. APA withdrawal led to rapid TSH improvement. Careful TSH monitoring is essential during APA treatment, especially in patients with pre‐existing thyroid dysfunction or…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
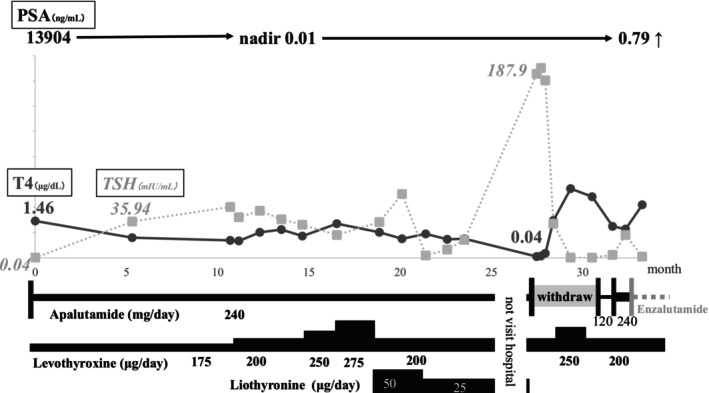 FIGURE 1
FIGURE 1| Case | Age | Prostate cancer | Patient history | After start APA (month) | TSH (mIU/L) | Levothyroxine increase (%) | Outcome |
|---|---|---|---|---|---|---|---|
| 1 | 76 | nmCRPC | Thyroidectomy | 2 | 81.7 | 146 | APA stopped and returned to normal |
| 2 | 56 | mHSPC | Total thyroidectomy | 1 | 37.0 | 82 | Maintenance |
| 3 | 64 | mHSPC | Autoimmune hypothyroidism | 2 | 35.5 | 86 | Maintenance |
| This case | 60 | mHSPC | Total thyroidectomy | 5 | 35.94 | 157 | APA stopped and returned to normal |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsProstate Cancer Treatment and Research · Thyroid Cancer Diagnosis and Treatment · Thyroid Disorders and Treatments
Introduction
1
Prostate cancer is the most frequently diagnosed malignancy among men in many countries and a major cause of cancer‐related mortality [1]. Androgen deprivation therapy (ADT) has long been the mainstay of systemic treatment for advanced prostate cancer. Over the past decade, the introduction of androgen receptor signaling inhibitor (ARSI) has represented a major advance in hormonal therapy for this disease [2, 3, 4, 5]. Among the available medications, apalutamide (APA) was granted FDA approval in February 2018, and in Japan, it received insurance coverage in March 2019 for nonmetastatic castration resistance prostate cancer (CRPC) and in May 2020 for metastatic hormone‐sensitive prostate cancer (mHSPC). APA is a competitive inhibitor of the androgen receptor that suppresses androgen‐mediated transcriptional activity, which is essential for prostate cancer progression. Due to its demonstrated efficacy and manageable safety profile, APA has become widely used in clinical practice. Here, we report a case of APA‐induced hypothyroidism in a patient with metastatic prostate cancer who was receiving levothyroxine sodium hydrate replacement therapy following total thyroidectomy.
Case Report
2
A 65‐year‐old male patient had undergone total thyroidectomy for papillary thyroid cancer 8 years previously and had been receiving levothyroxine replacement therapy. During routine blood testing at an otolaryngology department, markedly elevated coagulation markers were detected: FDP level of 264.1 μg/dL and a D‐dimmer level of 113.0 μg/dL. The patient was subsequently referred to the department of hematology for bone marrow biopsy, which revealed AMACR‐positive adenocarcinoma. Based on these findings, bone metastasis from prostate cancer was suspected and he was referred to our department. PSA levels were elevated at 13 904 ng/mL; however, digital rectal examination revealed no obvious malignant findings. Positron emission tomography (PET) showed heterogeneous uptake in the ribs, right scapula, and spine. Due to right shoulder pain, the patient underwent palliative radiotherapy (30 Gy/10 fr), followed by surgical castration and transrectal prostate biopsy. The diagnosis revealed adenocarcinoma, with a Gleason score of 4 + 4, and the clinical stage was cT1cN0M1 (bone: ribs, right scapula, and spine). He was started on a dosage of 240 mg/day of APA, resulting in a rapid decline in PSA levels to 0.01 ng/mL within 7 months. However, 5 months after starting APA, the TSH level was 35.94 mIU/L, and 17 months later, it remained high, the levothyroxine dosage was increased to 275 g/day. In addition, 50 μg of Liothyronine was used, but thyroid function did not stabilize. After that, he was not allowed to visit the hospital for 4 months. Twenty‐six months later, the TSH level had reached 187.9 mIU/L prompting the suspicion of APA‐induced hypothyroidism (Grade 2). APA was discontinued, after which TSH levels improved, therefore APA was restarted at a reduced dose of 120 mg/day, however, PSA levels were elevated. The dose of APA was increased to 240 mg/day again; regardless of this, the PSA increase was not suppressed, and the treatment was switched to enzalutamide. The clinical course of this patient is summarized in Figure 1.
PSA level decreased rapidly after starting APA. TSH level increased to 35.94 mIU/L at 5 months, 50.12 mIU/L at 9 months, and 187.9 mIU/L at 26 months after APA treatment initiation. APA‐induced hypothyroidism was suspected, and TSH level improved rapidly after withdrawal of APA. However, systemic treatment was switched to enzalutamide due to disease progression.
Discussion
3
APA, a novel ARSI, was approved in Japan in March 2019 and has since been widely used in clinical practice. The most commonly reported adverse events are fatigue and skin rash [4, 5]. However, hypothyroidism has also been reported. In the SPARTAN study of nonmetastatic CRPC (nmCRPC), hypothyroidism was reported in 8.1% of patients [4], and in the TITAN study of mHSPC, it was reported in 6.5%–7.1% of patients [5, 6]; but no cases of grade 3 or higher hypothyroidism were reported.
APA induces UDP‐glucuronosyltransferase (UGT) in the liver, promoting the glucuronidation of levothyroxine and subsequent excretion of thyroid hormones in the bile [7]. In other words, the pharmacokinetic interaction between APA and levothyroxine results in an increase in levothyroxine clearance, thereby reducing its therapeutic effect. This results in a reduction of thyroid hormone levels within the body, consequently leading to an elevated TSH level through negative feedback. Additionally, Quattrochi et al. indicate that APA reduces the intestinal absorption of levothyroxine, thereby explaining the higher prevalence of hypothyroidism observed in patients receiving levothyroxine therapy during APA treatment [8]. In the present case, the complete absence of thyroid reserve capacity due to total thyroidectomy when APA‐induced UGT metabolism was triggered led to a significant increase in TSH.
Daviduck et al. reported that patients with pre‐existing hypothyroidism are more susceptible to the thyroid dysfunction during APA therapy, and worsening hypothyroidism was observed in 30% of these patients [9]. Moffatt et al. reported a two‐ to threefold increase in levothyroxine supplementation but a standardized management strategy was not proposed [10]. David et al. summarized three similar cases, all of whom showed rapid TSH elevation 1–2 months after APA initiation [11]. In all three patients, a markedly increased serum TSH level (> 30 mIU/L) was observed within this short timeframe, which was much earlier than the median time to the first TSH elevation of 113 days reported in the SPARTAN study [4]. In some cases, the levothyroxine dose could be reduced after discontinuing APA, while in other cases, normalization required a longer duration. Although there were no data available immediately after the start of APA in this case, the patient's TSH level was as high as 35.94 mIU/L 5 months after starting APA, suggesting that hypothyroidism had already developed at that time and possibly earlier. This clinical course closely resembles that reported in the three previously described cases (Table 1). Furthermore, this case suggests that the patient's physical condition was poor before the sudden rise in TSH levels at 26 months and that he may not have been able to take enough levothyroxine. This finding means the critical importance of close and continuous monitoring in patients receiving levothyroxine therapy.
The standardization of thyroid function monitoring during APA treatment is desirable in future clinical practice. The current guideline recommends measuring TSH and FT4 at baseline, reassessing after 4–6 weeks, continuing at 4–6 month intervals until stabilization, and subsequently performing annual evaluations [12]. However, in this case, TSH and T4 levels underwent a precipitous change following a four‐month period of nonvisitation at the hospital. Particularly in patients with pre‐existing hypothyroidism who are receiving levothyroxine replacement therapy, routine follow‐up may prove to be inadequate in such cases. Consequently, the necessity of monthly blood tests may be necessary. Nevertheless, with careful endocrine monitoring, it is probable that APA therapy can be safely continued.
APA is an effective prostate cancer treatment, but the potential development of hypothyroidism should be closely monitored in patients with pre‐existing thyroid disease. With regular TSH and FT4 monitoring, appropriate levothyroxine supplementation, and collaboration with other departments, we consider that APA treatment can be continued safely, especially in patients with pre‐existing thyroid disease.
Consent
Informed consent was obtained from all individual participants included in the study.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1H. Sung , J. Ferlay , R. L. Siegel , et al., “Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries,” CA: A Cancer Journal for Clinicians 71 (2021): 209–249.33538338 10.3322/caac.21660 · doi ↗ · pubmed ↗
- 2C. J. Ryan , M. R. Smith , J. S. de Bono , et al., “Abiraterone in Metastatic Prostate Cancer Without Previous Chemotherapy,” New England Journal of Medicine 368 (2013): 138–148.23228172 10.1056/NEJ Moa 1209096 PMC 3683570 · doi ↗ · pubmed ↗
- 3T. M. Beer , A. J. Armstrong , D. E. Rathkopf , et al., “Enzalutamide in Metastatic Prostate Cancer Before Chemotherapy,” New England Journal of Medicine 371 (2014): 424–433.24881730 10.1056/NEJ Moa 1405095 PMC 4418931 · doi ↗ · pubmed ↗
- 4M. R. Smith , F. Saad , S. Chowdhury , et al., “Apalutamide Treatment and Metastasis‐Free Survival in Prostate Cancer,” New England Journal of Medicine 378 (2018): 1408–1418.29420164 10.1056/NEJ Moa 1715546 · doi ↗ · pubmed ↗
- 5K. N. Chi , N. Agarwal , A. Bjartell , et al., “Apalutamide for Metastatic, Castration‐Sensitive Prostate Cancer,” New England Journal of Medicine 381 (2019): 13–24.31150574 10.1056/NEJ Moa 1903307 · doi ↗ · pubmed ↗
- 6H. Uemura , G. Arai , H. Suzuki , et al., “Apalutamide for Metastatic, Castration‐Sensitive Prostate Cancer in the Japanese Population: A Subgroup Analysis of the Randomized, Double‐Blind, Placebo‐Controlled Phase 3 TITAN Study,” International Journal of Urology 28 (2021): 280–287.33295007 10.1111/iju.14447 · doi ↗ · pubmed ↗
- 7T. A. Richardson and C. D. Klaassen , “Role of UDP‐Glucuronosyltransferase (UGT) 2B 2 in Metabolism of Triiodothyronine: Effect of Microsomal Enzyme Inducers in Sprague Dawley and UGT 2B 2‐Deficient Fischer 344 Rats,” Toxicological Sciences 116 (2010): 413–421.20421340 10.1093/toxsci/kfq 125PMC 2905399 · doi ↗ · pubmed ↗
- 8F. Quattrochi , S. Grunenwald , and P. Caron , “Apalutamide Treatment and Refractory Hypothyroidism: Effects of Apalutamide on Levothyroxine Metabolism,” European Thyroid Journal 14, no. 5 (2025): e 250185.40905521 10.1530/ETJ-25-0185 PMC 12433934 · doi ↗ · pubmed ↗